Khusanov A. M.1, Akilov Kh. A.1, Ibadov R. A.2
1Center for the Development of Professional Qualifications of Medical Workers
2Republican Specialized Scientific and Practice Medical Center of Surgery Named after Academician V.Vakhidov, Tashkent, Uzbekistan
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The article presents the results of applying modern strategies for the development of inpatient care as part of the modernization of a specialized multidisciplinary medical center designed to treat patients with coronavirus infection COVID-19. Possible ways of solving organizational issues are discussed in order to improve the quality and availability of medical care for patients with coronavirus infection COVID-19.
Keywords:
COVID-19, Public health, Healthcare organization, Healthcare management, Reforming a specialized multidisciplinary medical center
Cite this paper: Khusanov A. M., Akilov Kh. A., Ibadov R. A., The Main Directions of Improving and Intensifying the Work of a Specialized Medical Center in the Context of the COVID-19 Pandemic, American Journal of Medicine and Medical Sciences, Vol. 10 No. 12, 2020, pp. 1014-1019. doi: 10.5923/j.ajmms.20201012.18.
1. Introduction
The devastating impact of the COVID-19 pandemic has become a truly serious test for the entire global community in 2020 [1,2]. The spread of this virus has long passed from the category of the most significant challenge to the sustainability of public health systems ”into an existential threat to all spheres of human activity. In the fight against the COVID-19 pandemic, almost all countries of the world have chosen the path of isolation, which means the closure of national borders, the cessation of civil transport links, and the suspension or restriction of the activities of industrial enterprises [3,4].The current pandemic has served as a test of the effectiveness of management, preparedness for extraordinary situations and the strength of national health systems, has led to a sharp increase in the role of government, the main tasks of which are making systemic decisions for public health in order to prevent the spread of COVID-19, improving the regulatory framework for timely and coordinated response to emergency situations and the introduction of innovative management methods [5].In the context of the COVID-19 pandemic, on the basis of the adopted Decrees and Decrees of the President of the Republic of Uzbekistan and the Decree of the Cabinet of Ministers of the Republic of Uzbekistan, attention was focused on supporting and optimizing the healthcare organization system, which helped to quickly increase the availability and efficiency of a large-scale infectious diseases hospital, created on the basis of a new specialized multidisciplinary medical center in Zangiata district of Tashkent region.To solve the tasks specified in the relevant regulatory documents, support the preparedness of the specialized medical center and the response to the management of patients with COVID-19, strategies for the development of the specialized medical center were formulated and several algorithms were developed. The elements described in these algorithms meet the requirements of the national health system, but may not apply to all hospitals, and may need to be adapted to the specific characteristics of each hospital and the legislation that regulates it.
2. Results of Our Experience
At the initial stage of the implementation of the tasks set, the paramount was to ensure the continuity of basic medical services (Fig. 1). The action plan was drawn up on the basis of the analysis of the dynamics of the number of admitted and discharged patients. In this connection, the maximum patient throughput was calculated and the growth in demand for hospital services during the COVID-19 outbreak was estimated. | Figure 1. Action plan to ensure continuity of essential health services in a specialized center |
The study of the dynamics of quantitative indicators of admission and discharge of patients (Fig. 2) showed that in the period until August 22, 2020, there was a significant increase in hospitalization of patients with COVID-19 (mass admission). Later, due to the development and adherence to the criteria for assessing the condition of patients preparing for discharge, the indicators of the hospital's throughput were improved. As a result, the center was prepared for the next outbreak and an increase in morbidity and hospitalizations, which was noted already 2 weeks after the weakening of quarantine measures in the country.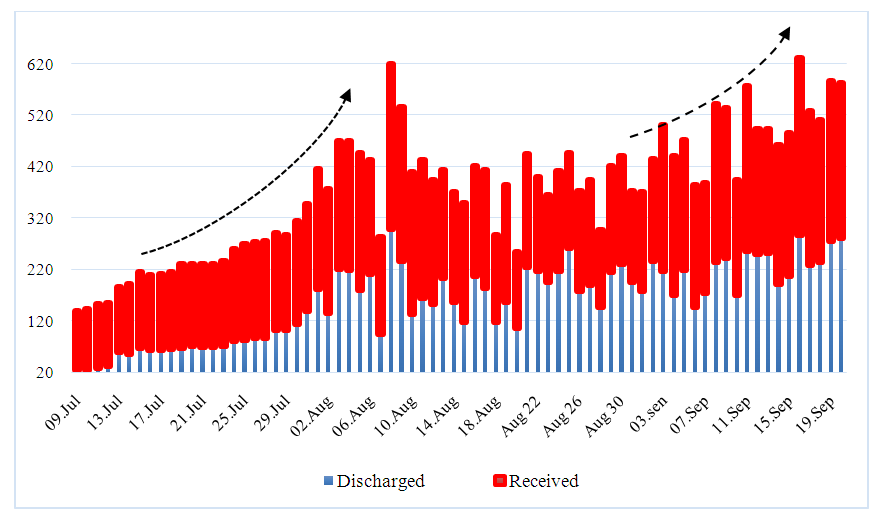 | Figure 2. The ratio of admitted and discharged patients |
Initially, only 2000 beds were organized in the Center and the construction of Zangiata-1 (5 blocks) was completely completed. As demand increased, the remaining blocks were completed, i.e. Zangiata-2 (5 blocks), the number of beds was increased to 3167, 8 intensive care and intensive care units were formed with a capacity of 288 beds, which made it possible to close other hospitals in Tashkent and their reverse profiling. Also, intensive care units were additionally organized and equipped in each block of the center (a total of 240 beds), which made it possible to relieve the intensive care units, in which the treatment of severe and extremely difficult patients continued.Thus, taking into account the required physical space, available personnel, materials and treatment processes, the task was solved to define and create additional zones that can be used to increase patient care opportunities (reserve capacity). All rooms that provide medical care to critically ill patients were equipped with pulse oximeters, oxygen delivery systems and disposable oxygen therapy devices (nasal cannulas, Venturi masks and breathing bag masks).Also, criteria for reassigning conventional wards to boxes and semi-boxes were defined as soon as the number of patients reaches a threshold, and the transfer of non-isolated patients is planned.By August 21, the ratio of admitted and discharged patients became equal (49% to 51%), which was achieved by expanding the bed capacity and using patient triage protocols.All hospital services were prioritized and nonessential services identified that could be suspended if necessary. For example, operating rooms, a maternity complex and dressing rooms were converted into intensive care units, thereby increasing the hospital's capacity for hospitalizing seriously ill patients.We have analyzed the dynamics of changes in the ratio of the frequency of moderate, severe and extremely severe cases admitted to a specialized center (Fig. 3). According to the results, there was a massive admission of seriously ill patients in the period up to August 18 (the maximum number reached 230 hospitalizations on August 8). At the same time, an important component of admissions departments has become the correct distribution of patients to the appropriate departments for the provision of standardized care.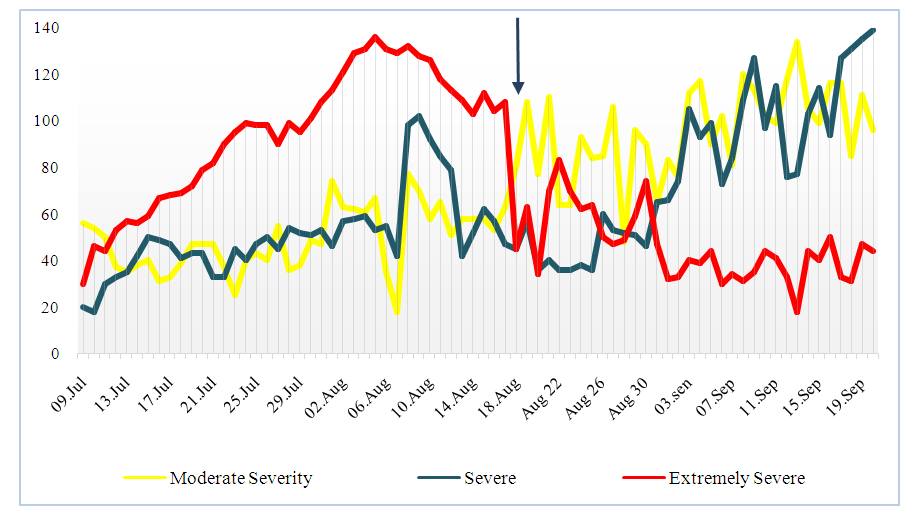 | Figure 3. The condition of patients upon admission to a specialized center in dynamics |
It should also be noted that the creation of local COVID-19 specialized outpatient clinics and diagnostic triage centers served as an equation for the percentage of admitted and discharged patients. Under these conditions, the center was able to hospitalize severe and extremely severe patients with COVID-19 with damage to more than 70% of the lung tissue.In this connection, an algorithm was developed for the transfer of patients with a confirmed or doubtful diagnosis of COVID-19, which is based on an assessment of the respiratory status.Factor analysis showed that predictors of severe and extremely severe course of coronavirus infection COVID-19 are the presence of concomitant pathology of vital organs, including diabetes mellitus, malignant tumors, cerebrovascular pathology, arterial hypertension ≥ 2 tbsp., Immunosuppressive conditions, chronic lung pathology, acute abdominal pathology, acute thoracic pathology, leukocytosis more than 10x109 / l and C-reactive protein more than 50 mg / l.Based on the data obtained, strategies for the provision of services for patients at risk during the outbreak that are not related to COVID-19 were identified.Thus, a demographic and analytical study of persons admitted with severe and extremely severe forms of COVID-19 to a specialized multidisciplinary clinic was carried out. As a result, the most vulnerable groups of patients were identified and predictors were formed to predict the likelihood of unfavorable outcomes of the disease. Tactics and criteria for assessing the condition of patients and clinical manifestations of COVID-19 have been developed with the aim of transferring them to the appropriate departments for providing standardized care. Adopted hospitalization and discharge criteria and prioritized patients and clinical interventions according to available treatment options and needs. Also, the resources (human resources and logistics) required to ensure the continuity of those hospital services that are identified as important are identified.It should be noted that the implementation of this program began with the task of requesting and attracting specialists from the leading medical centers of the country, as well as the creation of a consulting group for severe and extremely difficult patients, which included leading specialists in the field of resuscitation and intensive care (by order of the Ministry of Health of the Republic of Uzbekistan 10 -5/2111 from 07/10/2020).The creation of a coordination scheme for the activities of a specialized medical center to combat the COVID-19 pandemic (Fig. 4) led to optimization in several directions. In particular, a patient management system was created and activated with the participation of heads of all departments and departments; a well-equipped reception area with functioning communication facilities was organized; the main response team has been formed, including the chief physician, the epidemiological control group, the heads of the relevant departments and departments (for example, the intensive care unit and intensive care unit) and an infectious disease specialist; roles and responsibilities for different response functions are assigned, with sufficient trained personnel to ensure continuity of work; compile an up-to-date directory of telephone numbers, places of residence and email addresses of employees; a contingency plan developed for staffing, logistics, budgeting and procurement; coordination mechanisms with local and health authorities identified and established.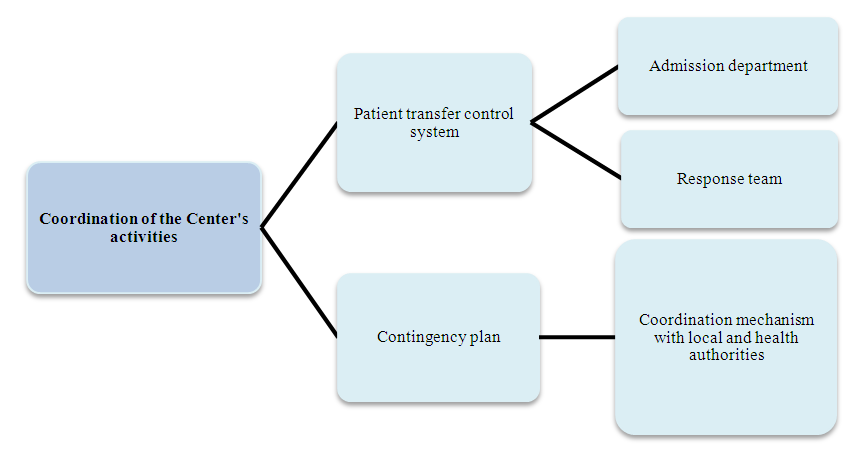 | Figure 4. Coordination of the activities of a specialized center to combat the COVID-19 pandemic |
At the same time, mechanisms of communication and cooperation with the integrated network of medical services at the local level have been activated, taking into account the timeliness of the supply of necessary medicines, laboratory services, materials and equipment, as well as the peculiarities of patient transportation.Priorities for improving logistics, providing operational support and proper supply management were facilitated by (Figure 5):- a developed and constantly updated list of all equipment, materials and drugs. At the same time, their consumption was assessed on the basis of the most probable scenarios of outbreaks, a situational approach;- ensuring the supply chain management procedure, taking into account the increased requirements with respect to quality, technical characteristics and established protocols. It also defines the conditions for a continuous supply of essential drugs and supplies (eg, inpatient and central stocks, contingency agreements with local suppliers);- the formation of storage facilities for additional stocks that meet all the requirements for temperature, humidity, cold chain, etc.;- activation of legally accessible and authorized administrative and financial mechanisms;- ensuring the order of management of work teams, including cleaning services, recreation areas, safe transport and the well-being of personnel;- provision of mechanisms for timely maintenance and repair of all equipment required for basic services;- ensuring the management of ambulances for transport between hospitals and an inventory of the vehicles available, as well as procedures for protecting the ambulance team and disinfecting machinery and equipment after each use;- ensuring that adequate back-up facilities are available for vital lines, including water, electricity and oxygen.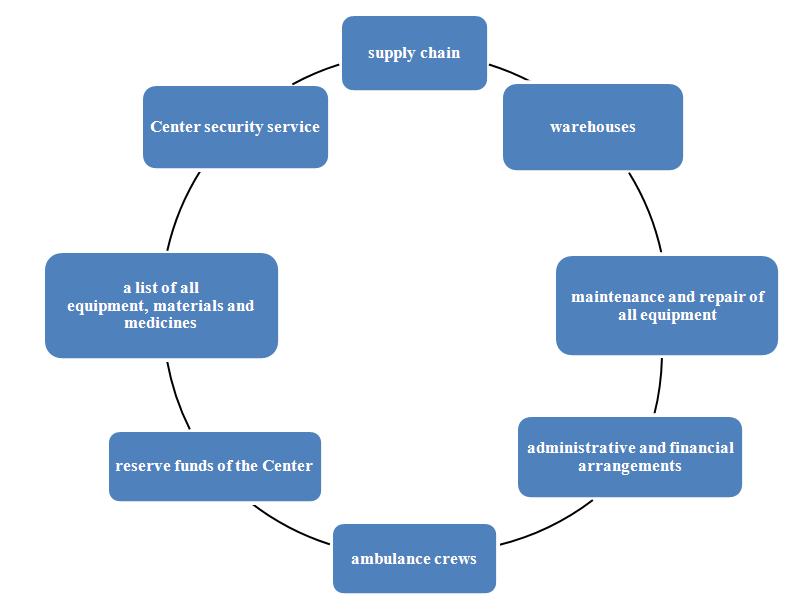 | Figure 5. System of operational support, logistics and supply management |
All of the above procedures were carried out using information technology. In particular, accessible procedures were established and personnel assigned to collect, validate and verify data and information on patient movement; a standardized reporting form was developed for hospitalizations (including intensive care), the frequency of suspected and confirmed cases, the clinical situation and cases of mortality; mechanisms for internal and external communication with a dedicated team have been created, including one person responsible for facilitating the exchange of information in real time; an official public information spokesman and a deputy have been appointed to coordinate and ensure consistent communications with the public, media and health authorities.As a result of these activities at the specialist center, staff and stakeholders are regularly informed about triage, transfer and case management (e.g. adapted admission and discharge criteria), infection prevention and control measures, hospital epidemiology, reporting requirements and safety measures.Today, the Center has adapted its staff management to ensure the continuity of the Center in response to increased demand, while maintaining the services identified as important.Today, all internal protocols, communication lines and standard operating procedures are easily accessible to all personnel, and information is easily accessible, concise, targeted and regularly updated (minimizes information overload); collection, processing and provision of information to controlling stakeholders (health authorities) is ensured; secured reliable and stable primary and backup communication systems (landline phones, internet, mobile devices, walkie-talkies, satellite phones, two-way radio communication equipment) and access to updated contact lists.
3. Conclusions
Thus, as a result of addressing a number of key evidence-based issues, a structured plan has been drawn up for intensive care units to manage the situation and manage critically ill COVID-19 in mass admissions. At the same time, it was noted that an important aspect of the transfer of patients with COVID-19 to provide standardized care is the development of criteria for assessing the clinical manifestations of COVID-19, the main link of which is the respiratory status.Special protocols were applied, on the basis of which complete isolation of premises, staff and patients was realized. The opening of the department and the entire emergency care process in the hospital required interdisciplinary, multi-level involvement of healthcare providers and hospital leaders who worked towards a common goal of patient care and hospital safety.The implementation of a target group of specialists from the leading centers of the republic made it possible to develop practical recommendations on the principles of organized response. The focus was on increasing hospital throughput, developing workflow algorithms related to patient care, replenishment of medical personnel and limited resources.Schemes have been developed to improve the structure of the new multidisciplinary COVID-19 Center, new personnel decisions have been made, a general pandemic response plan has been developed and the team is prepared for the next wave of COVID-19.
References
| [1] | Khalifa SAM, Mohamed BS, Elashal MH, et al. Comprehensive Overview on Multiple Strategies Fighting COVID-19. Int J Environ Res Public Health. 2020; 17(16): E5813. |
| [2] | Coronavirus Disease (COVID-19) Situation Report–133. Available online: https://4m.cn/c8FoU (accessed on 1 July 2020). |
| [3] | Coronavirus Disease (COVID-19) Situation Report–163. Available online: https://4m.cn/rqabe (accessed on 1 July 2020). |
| [4] | Centers for Disease Control and Prevention. Discontinuation of isolation for persons with COVID-19 not in healthcare settings (interim guidance). 2020. Available at: https://www.cdc.gov/coronavirus/2019-ncov/hcp/disposition-in-home-patients.html. Accessed June 8, 2020. |
| [5] | WHO. Director-General’s opening remarks at the media briefing on COVID-19. March 18, 2020. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML