-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2020; 10(12): 1010-1013
doi:10.5923/j.ajmms.20201012.17
Received: Nov. 19, 2020; Accepted: Dec. 2, 2020; Published: Dec. 15, 2020

Ways of Prevention and Treatment of Complications after Hernioplasty for Hernias (An Original Article)
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMuazzamov Boʙir Bakhodirovich1, Akimov Vladimir Pavlovich2, Muazzamov Baxodir Rakhmonovich1, Khakimov Murod Shavkatovich3, Norov Firuz Khakʙerdievich1
1Bukhara State Medical Institute, Bukhara, Uzbekistan
2Federal State Budgetary Educational Institution of Higher Education North-Western State Medical University Named after I.I. Mechnikov "Ministry of Health of Russia
3Tashkent Medical Academy, Tashkent, Uzbekistan
Correspondence to: Muazzamov Boʙir Bakhodirovich, Bukhara State Medical Institute, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The technique of operations performed for hernias of the anterior abdominal wall has achieved tremendous success to date, the uniqueness and respectability of which is given in many literary sources. The aim of the study is to assess the possibilities of modern herniology in the surgical treatment of ventral hernias. Information about the methods of treatment of ventral hernias and the prevention of complications after treatment is provided by examining 114 patients with this pathology. The most frequent complications with methods of their prevention and treatment are considered. In recent surgery, the main place is given to endovideoscopic methods of treating hernias, which, unlike previously existing methods, are more reliable and adequate.
Keywords: Ventral hernia, Endovideoscopy, Allohernioplasty
Cite this paper: Muazzamov Boʙir Bakhodirovich, Akimov Vladimir Pavlovich, Muazzamov Baxodir Rakhmonovich, Khakimov Murod Shavkatovich, Norov Firuz Khakʙerdievich, Ways of Prevention and Treatment of Complications after Hernioplasty for Hernias (An Original Article), American Journal of Medicine and Medical Sciences, Vol. 10 No. 12, 2020, pp. 1010-1013. doi: 10.5923/j.ajmms.20201012.17.
Article Outline
1. Relevance
- The technique of operations performed for hernias of the anterior abdominal wall has achieved tremendous success to date, the uniqueness and respectability of which is given in many literary sources [3,5,12]. Since the mid-50s of the last century, the methods of hernia repair went through many stages and improved to the highest point of its development so that it became possible to strengthen the defects in modern surgery without a single suture [4,6,7,9]. The problem that worried the world society of surgeons engaged in herniologyseems to have been resolved, however, despite progress in this area, the question arises about the occurrence of postoperative complications, which, along with the improvement of surgical technique, are noted according to the literature from 12.3% to 19.5% of cases [1,10]. If earlier, when carrying out the method of hernia repair with the use of hernia orifice plastic using one's own tissues, a large number of postoperative complications were observed, such as purulent-necrotic and purulent-septic complications, causing secondary wound healing, and in some cases leading to repeated surgery, due to the traumatic factor in conducting wide incisions for adequate access to the elements of hernias, then at present, recurrence [2,7,8,11]. To address these issues, we set ourselves a task aimed at eliminating these problems and improving the quality of life of patients.
2. Objective
- To review the complications in open and laparoscopic hernioplasty and show the possibilities of increasing the efficiency of surgical treatment of patients with ventral hernias.
3. Material and Methods
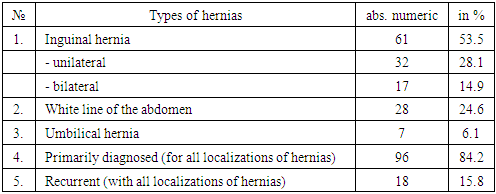
- The research was carried out at the Department of Faculty and Hospital Surgery, Urology of the Bukhara State Medical Institute together with the Department of Surgery named after N.D. Monastyrsky North-Western State Medical University named after I.I. Mechnikov Ministry of Health of the Russian Federation. The study involved 114 (100%) patients with abdominal hernias of various localization. Of these, 87 (76.3%) were men, 27 (23.7%) were women. The patients' age ranged from 22 ± 1.9 to 68 ± 3.4 years.The number of patients with inguinal hernia was 61 (53.5%), 17 (14.9%) with bilateral pathology, and the remaining 32 (28.1%) with unilateral lesion. With a hernia of the white line of the abdomen, 28 (24.6%) patients were observed. The number of persons with recurrent hernia was 18 (15.8%). 7 (6.1%) patients with umbilical hernia were examined. 54 (47.4%) patients underwent endo-video surgery, with 46 (40.4%) performed using the TAPP method, and 8 (7%) patients using the TEPP method. Moreover, 3 (2.6%) patients underwent TAPP surgery with recurrent inguinal hernia. In the remaining 60 (52.6%) cases, laparotomy herniotomy was performed. All patients used endoprostheses - Esfield meshes for the purpose of hernia repairsizes 15×25 cm, 15x30 cm, depending on the size of the defect. To fix the mesh during endovideosurgical interventions, polyacrylate glue was used, in open operations - suture material produced by Ethicon, synthetic threads with a needle with a cross section of 2.0. To diagnose hernias, a clinical method was used to determine the presence of a defect and the contents of the sac, using the symptom of "cough impulse". From instrumental diagnostic methods, ultrasound examination (ultrasound) was used using Sonoscape - 4000 and Vivid devices - M 40. This research method was mandatory for all patients, regardless of the location and size of the hernial protrusion. In addition, all patients underwent clinical and biochemical analyzes of blood and urine. The patients were hospitalized, the timing of discharge was determined depending on the time of wound healing, regression of concomitant diseases, normalization of the general condition and averaged from 3-4 ± 1.3 to 10-11 ± 3.7 days. Dynamic observation of the patients was carried out 1, 3, 6, 9 and 18 months after the operation.
|
4. Results and Its Discussion
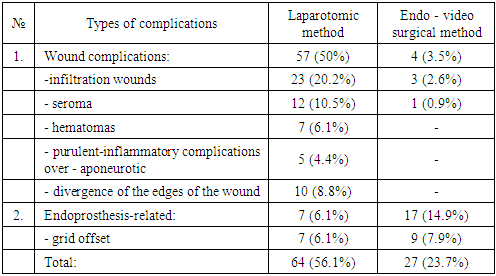
- The performed surgical interventions showed that complications in the postoperative period depended on the preoperative preparation, technique and materials used during the operation, in compliance with the rules of asepsis and antiseptics. Complications observed after hernioplasty, depending on the method of the operation, were a different ratio, which is shown in Table 2.
|
|
|
5. Conclusions
- Currently, various methods of laparoscopic herniotomy are being actively introduced into surgical practice for hernias of the anterior abdominal wall, which have shown themselves as alternative methods of treatment compared to methods of laparotomic access and can be recommended for widespread use. Complications arising both with laparotomy access and with endo video surgery can be associated with the technique of surgical treatment, significantly reducing wound complications with the latter method, the body's response to embedded foreign bodies, such as drainage tubes, which is mainly used in laparotomy method, as well as mesh endoprostheses, which can also cause various pathological manifestations. A thorough study of patients in the preoperative period and an assessment of the volume of the forthcoming operation, considering the size and nature of the hernial protrusion, as well as the prevention and treatment of concomitant diseases, affect the outcome and long-term results in the postoperative period.
Conflicts of Interest
- The authors have no conflicts of interest. Information about the source of support in the form of grants, equipment, and drugs. The authors did not receive financial support from manufacturers of medicines and medical equipment.