-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2020; 10(11): 924-928
doi:10.5923/j.ajmms.20201011.20
Received: Sep. 29, 2020; Accepted: Oct. 21, 2020; Published: Nov. 28, 2020

Peculiarities of Wound Complications Prophylaxy at Alloplasty of Strangulated Postoperative Ventral Hernias
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLB. R. Abdullajanov, A. Kh. Babadjanov, M. F. Nishanov, P. M. Isakov
Andijan State Medical Institute, Uzbekistan
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Aim of the study was to improve the results of surgical treatment of strangulated ventral hernias by enhancement of tactical and technical approaches to preventing the development of postoperative complications. Material and methods. The authors conducted a study of 147 patients with strangulated ventral hernias operated on an emergency basis in the surgery department of the Andijan State Medical Institute clinics for the period from 2015 to 2020. All patients were divided into two groups: the main group included 56 patients with the indicated diagnosis; the comparison group included 91 patients. The age of the patients varied from 23 to 83 years. The mean age was 53.5 ± 1.3 years in the comparison group and 54.5 ± 1.4 years in the main group.The authors used a method for the prevention of wound purulent-inflammatory complications at alloplasty of strangulated postoperative ventral hernias, including the introduction of a drug into the operation wound. After fixation of the synthetic implant, Redon-type drainage systems were placed in the operating wound; 50 ml of “FarGALS” solution in a ratio of 1: 3 was used as a drug. Conclusion. The authors concluded that during the entire postoperative period statistically better indicators of the pain syndrome point scale were observed in the main group of patients (t = 2.43-3.18; p <0.05).
Keywords: Strangulated hernia, Alloplasty, Postoperative complications prophylaxy
Cite this paper: B. R. Abdullajanov, A. Kh. Babadjanov, M. F. Nishanov, P. M. Isakov, Peculiarities of Wound Complications Prophylaxy at Alloplasty of Strangulated Postoperative Ventral Hernias, American Journal of Medicine and Medical Sciences, Vol. 10 No. 11, 2020, pp. 924-928. doi: 10.5923/j.ajmms.20201011.20.
1. Introduction
- The use of mesh polymer endoprostheses in the treatment of ventral hernias has reduced the number of relapses, but has led to an increase of wound complications frequency. Not only purulent-inflammatory processes in the wound are distinguished among the complications, but also their effect on the probability of hernia recurrence. The problem of reducing the risk of wound infection development remains relevant [1].A special category is made by patients with urgent indications for hernioplasty: at the development of a stargulated hernia, fistulas and other complications during the elimination of which the surgical wound is always susceptible to the development of microbial contamination [2]. The frequency of wound infection in these cases can reach 37% and more, which affects not only the outcome of the operation, but also leads to a significant increase in costs due to the need for additional procedures and a longer hospital stay [3]. All preventive measures should be comprehensively aimed at the three points of the surgical operation, which the World Health Organization summarizes as preoperative, intra- and postoperative measures [4]. Until now, various methods of antibiotic prophylaxis of hernioplasty wound complications, suturing of an operation wound, introduction of cytokines in the postoperative period, injection of a complex of autologous cytokines, puncture of the paraprosthetic cavity followed by the introduction of antiseptics, treatment of the operation wound surface and prosthesis with a flow of low-temperature argon plasma have been introduced into the practice of herniology. At the same time, the authors attribute to the disadvantages of antibiotic prophylaxis in hernia surgery their insufficient effectiveness in conditions of antibiotic resistance of nosocomial microflora and the appearance of antibiotic-resistant strains of microorganisms [5-6].The disadvantages of methods of an operation wound suturing in order to prevent the formation of a residual cavity that contributes to the formation of seroma are their trauma and additional production of serous fluid due to the biological properties of the suture material. The necessity for special PVC tubes for the introduction of cytokines and the complexity of the preparation of the cytokines themselves in the conditions of urgent surgery, when the average time from the moment of the patient’s admission to the surgery is 1 hour, is impossible [7,8].Puncture procedures of the peri-prosthetic cavity followed by the introduction of antiseptics and evacuation of the contents from the cavity formations [9]; long-term vacuum aspiration of postoperative wounds seromas [10]; installation of drains and flow-through washing of the wound under ultrasound control [11] give a relatively short-term effect. All this creates the need for multiple punctures of seromas, suppuration of postoperative wounds and their drainage which can cause the development of a wound infection associated with pain for the patient.Techniques for treating the surface of an operation wound and prosthesis with a flow of low-temperature argon plasma also have their disadvantages. Low-temperature plasma sources are technically sophisticated equipment with low economic efficiency. They can lead to the destruction of materials at the points of contact between the plasma and the treated surface. The use of atmospheric pressure discharges at high voltage (10-40 kV) requires a high level of safety [12]. Aim of the study was to improve the results of surgical treatment of strangulated ventral hernias by enhancement of tactical and technical approaches to preventing the development of postoperative complications.This article presents a comparative analysis of the results of the application of an optimized technique for the prevention of wound complications at alloplasty of strangulated postoperative ventral hernias.
2. Material and Method
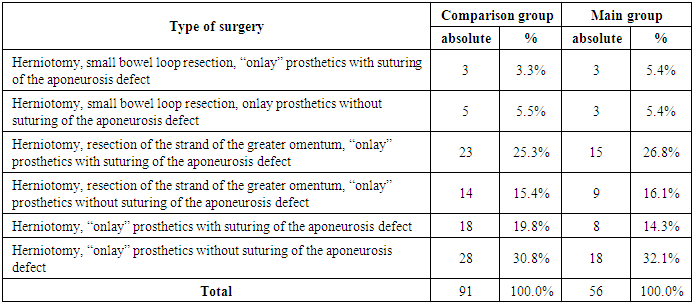
- The study was based on the results of treatment of 147 patients with strangulated ventral hernias. All patients were performed emergency surgery in the department of surgery of the Andijan State Medical Institute from 2015 to 2020. All patients were divided into two groups: the main group included 56 patients with the indicated diagnosis; the comparison group included 91 patients. The age of the patients varied from 23 to 83 years. The mean age was 53.5 ± 1.3 years in the comparison group and 54.5 ± 1.4 years in the main group.The average time of strangulation in both groups did not exceed 8 hours. Most often patients admitted within the first 2-4 hours after the strangulation of the hernia. The frequency of patients addressing for medical care later than 4 hours after strangulation was practically the same in both groups and made up 23.2% and 20.9% in the main and comparison groups, respectively, which excluded the negative impact of the strangulation time on the study results. The severity of the general condition of patients was assessed as average in the overwhelming majority - 91.1% (51) and 92.3% (84) in the main and in the comparison groups, respectively. There was a severe degree of the disease only in 3.6% (2) cases of the main and in 2.2% (2) cases of the comparison groups. By the nature of the performed surgeries, the patients were distributed as follows: “onlay” prosthetics with suturing of the aponeurosis defect was performed in 44 (48.4%) patients in the comparison group and in 26 (46.4%) cases of the main group. “Onlay” prosthetics without suturing the aponeurosis defect was performed in 47 (51.6%) cases in the comparison group and in 30 (53.6%) patients in the main group. The distribution of patients by surgery type is presented in Table 1.
|
3. Results and Discussion
- According to the data obtained on a 10-point visual analogue scale, the intensity of pain on the 1st day after surgery was assessed as strong by patients both in the comparison group and in the main group, the mean values made up 7.8 and 7.2 points, respectively. On the second day, against the background of the adopted treatment tactics in the main group, the intensity of pain was lower than in the comparison group, and corresponded to 5-6 points (mean value - 6.5). In the future, this trend continued, and on the 6th day after the operation, patients in the main group noted moderate pain, while in the comparison group, patients noted pain of moderate intensity. The dynamics of differences in the intensity of postoperative pain can be more clearly traced in Fig. 1.
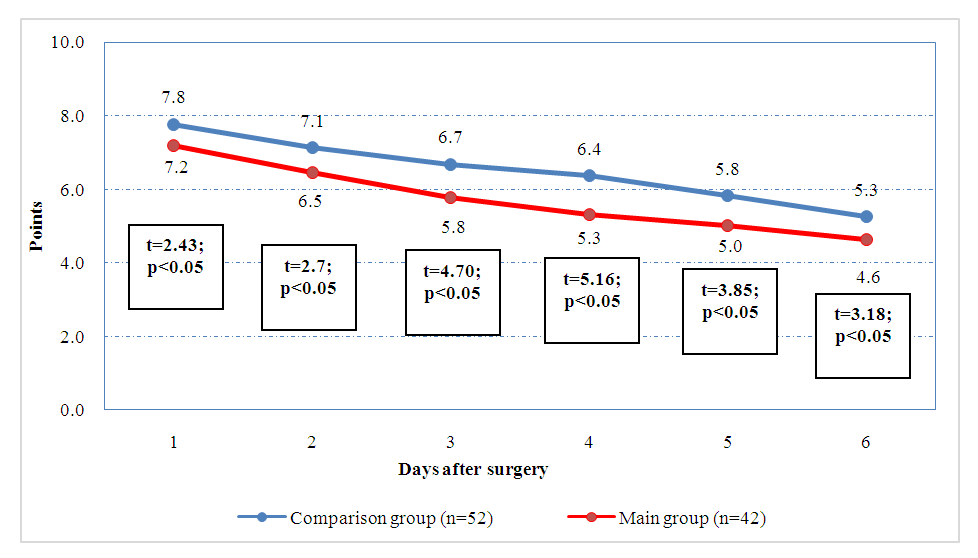 | Figure 1. Dynamics of pain intensity by an analogue scale |
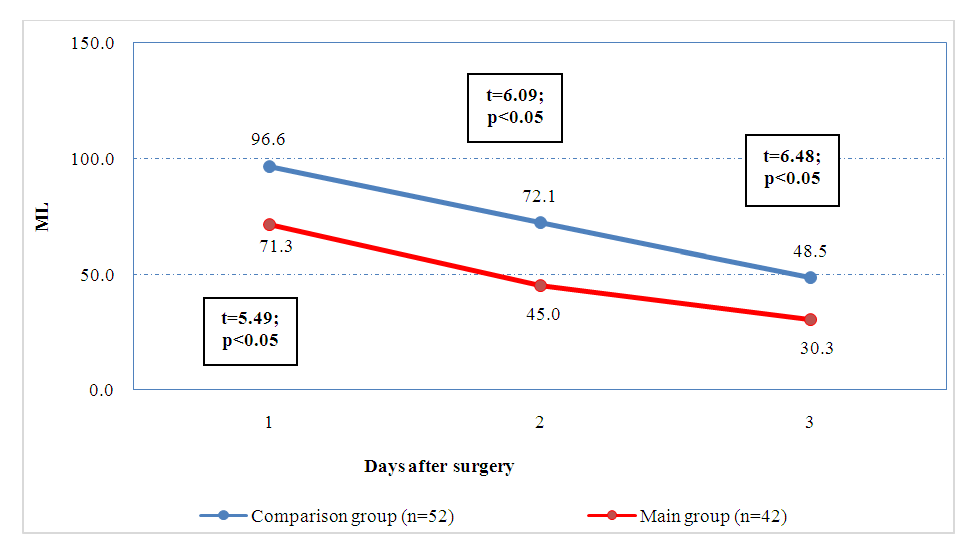 | Figure 2. Dynamics of changes in the amount of drainage secretions (ml) |
|
|
4. Conclusions
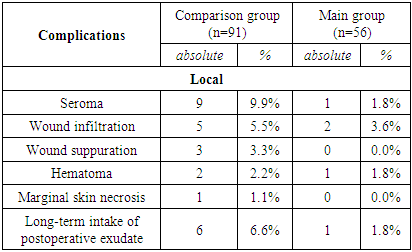
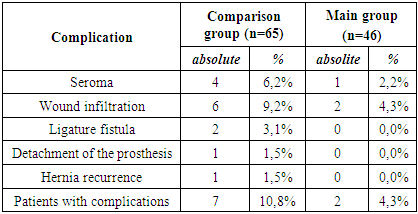
- The use of the proposed method for intraoperative prevention of the wound complications development as preventive measures allowed to improve generally the results of surgical treatment of patients with strangulated ventral hernias. These measures made it possible to reduce the incidence of wound complications in the immediate period from 20.9% (in 19 from 91 patients in the comparison group) to 7.1% (in 4 from 56 patients in the main group). The patients stay in the intensive care unit also decreased from 1.5 ± 0.1 (in the comparison group) to 1.2 ± 0.1 days (in the main group), and in general, the hospital stay decreased from 7.7 ± 0.1 to 6 . 7 ± 0.1 days. The risk of developing long-term specific complications decreased from 10.8% (in 6 of 65 observed patients in the comparison group) to 4.3% (in 2 of 46 observed patients in the main group).