Tillyashaikhov Mirzagolib Nigmatovich, Djanklich Saide Mustafaevna, Berkinov Alisher Alievich, Adilkhodjaev Askar Anvarovich, Imamov Olimdjon Abdilkhodjaevich, Ibragimov Shavkat Narzikulovich, Sabirdjanova Zulfiya Rashidovna, Bazarov Bekzod Bakhtiyarovich
Republican Specialized Scientific and Practical Medical Center of Oncology and Radiology, Tashkent, Uzbekistan
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
For the first time, a cancer registration system has been already created to process data on cancer patients in the Republican Specialized Scientific and Practical Medical Center of Oncology and Radiology (RSSPMCOR) and in its several branches. However, the existing system was found to be insufficient for data management across the regions of Uzbekistan. Along with the growth of cancer morbidity and the increase in the need for cancer care, it is necessary to develop a perfect model for registering cancer in Uzbekistan. A qualitative study using the data collection method by interviewing employees associated with registration activities has been conducted. The result of this research is the creation of a network skeleton for cancer registration based on RSSPMCOR and its affiliates, including compliance with data transfer security and a disaster recovery plan of information in case of possible system failures. The number of employees involved in cancer registration and the technical devices required to support the system has been also estimated.
Keywords:
Cancer registration system, Medical institutions, Oncology service, RSSMPCOR and its branches
Cite this paper: Tillyashaikhov Mirzagolib Nigmatovich, Djanklich Saide Mustafaevna, Berkinov Alisher Alievich, Adilkhodjaev Askar Anvarovich, Imamov Olimdjon Abdilkhodjaevich, Ibragimov Shavkat Narzikulovich, Sabirdjanova Zulfiya Rashidovna, Bazarov Bekzod Bakhtiyarovich, Development of a Population Cancer Register Model in the Republic of Uzbekistan, American Journal of Medicine and Medical Sciences, Vol. 10 No. 11, 2020, pp. 919-923. doi: 10.5923/j.ajmms.20201011.19.
1. Introduction
Further deepening of the reforming processes has been carrying out in the health care system of the Republic of Uzbekistan for the recent years. An important role in these processes is played by the Decree of the President of the Republic of Uzbekistan PP No. 2866 dated by 04.04.2017 " About measures for the further development of the oncologic service and improvement of oncologic care for the population for 2017-2021", including a section on the creation and implementation of a cancer registry for all regional divisions of oncologic service during this period. According to the above mentioned decree, the structure of the oncologic service is given in the diagram below (Fig. 1) [1-2]. | Figure 1. Unified vertically integrated cancer care service |
According to many researches, the calculation of indicators during manual training is very laborious and routine. In addition, it is almost impossible to check the quality of data and to control duplicates. There is no flexibility in obtaining new indicators in such technology, except those ones which are included in standard statistical reports. All these phenomena lead to mistrust and unsatisfactory attitude towards medical statistics [3-6]. The volume of data entered into the register depends on the primary documents used by the register to obtain high-quality medical information. In the hospital register such a document is called ‘Case history,’ in the population register - special registration forms. In the case of unqualified or incomplete filling of primary documents, the register's possibilities for conducting scientific research and obtaining reliable results are reduced. Cancer is a chronic disease by its nature; the treatment process often takes several years. The monitoring of cancer patients does not stop even after the end of treatment. All information not only about the primary, but also about the following treatment, about the occurrence of complications, relapses or metastases, about the death of the patient (from cancer or from other causes) is also included into the register. It allows us to estimate the long-term (five-, ten-year) survival rate of patients. But obtaining such information requires a proven technology for monitoring patients [7,5].Until only paper forms were stored, all statistical processing of the accumulated data was consisted of the annual obtaining of State Statistics Reports. At the same time, it was impossible to analyze the data in cases where the corresponding column was not provided for the studied groups of patients. It was also impossible to move from the numbers in the statistical table to its constituent cases of the disease: for example, for verification or clarification, without repeating all the work of calculating the table. It led to the fact that more attention was paid by statisticians not to obtaining high-quality information, but to making the statistical reports submitted to higher authorities to be looked well.The introduction of modern automated technologies allows to automate the counting process of any tables and indicators instead of paying more attention to the quality of primary medical information and conducting scientific research [8,6,9- 10].Initially, a database of patients who underwent diagnostics and treatment at the Republican Specialized Scientific Practical Medical Center of Oncology and Radiology (RSSMPCOR) was created in the Republic of Uzbekistan based on the Access program in 2009. This database (hospital register) was installed in all departments of RSSMPCOR in order to conduct test work with the subsequent elimination of the identified deficiencies. It was revealed after testing that the program did not fully meet the requirements of the Ministry for the Development of Information Technologies and Communications of the Republic of Uzbekistan and the standards for software products. It required correction, and therefore, new software based on MSQL - the Cancer Registry information system (practically a population cancer registry) was created in 2012. The Cancer Registry information system was installed with technical difficulties in almost all regional divisions of the oncologic service and in the RSSMPCOR. However, over time, it turned out that this cancer registry did not correspond to the generally accepted international standards for cancer registration. At the moment, three questions have been raised to implement the cancer registry in all RSSMPCOR branches and primary care in Uzbekistan: What is the network architecture, security and implementation plan for a cancer registration system? What is the capacity of staff to implement the cancer registry? What is the provision of the necessary technical equipment to support the cancer registration system?Aim of this study is to analyze the requirements for registering cancer in Uzbekistan in a network of RSSMPCOR and its regional branches. The developed model of the cancer registration system will serve as a template for the implementation of the cancer registry in each regional branch of the Republic. Cancer patient data will be collected and coded according to an international standard allowing to provide comparison and exchange of information between hospitals. Moreover, adequate security will be applied between branch offices and RSSMPCOR so that access, theft and destruction of data can be prevented.
2. Material and Methods
This study was conducted by a method classified as a qualitative study, without experimental methods and without data processing. The study design was divided into four stages to meet international requirements (Fig. 2). | Figure 2. Design of the study |
Information for planning the creation of a cancer registration system model as well as an architectural plan was obtained from interviews of RSSMPCOR staff, its branches and district oncologists whose work was related with cancer registration. The questions in the questionnaire were created on the base of elements for developing a cancer registration system.
3. Results and Discussion
This study was aimed to develop a model for the implementation of a cancer registry program as a cancer registration tool and as a part of development plan for a national cancer registration system. According to the President's decree, this software will be used with minimum requirements. Additional requirements will depend on the needs of each healthcare facility, such as computer specifications and staff qualifications.The development of the model began with the collection of information on the networked cancer registry system in the Republic of Uzbekistan. First of all, it is necessary to build a systematic plan for cancer registration structured according to the district-regional model - "Network system of the population cancer registry in the Republic of Uzbekistan" (Fig. 3).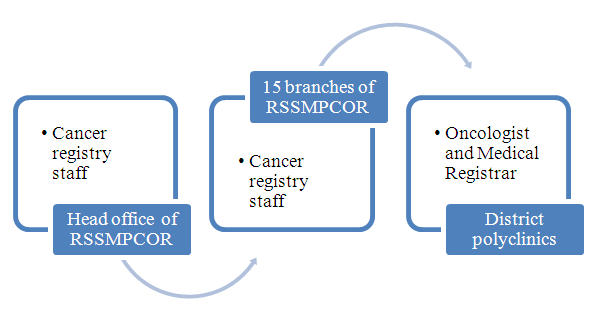 | Figure 3. Systematic plan for cancer registration structured according to the district-regional model |
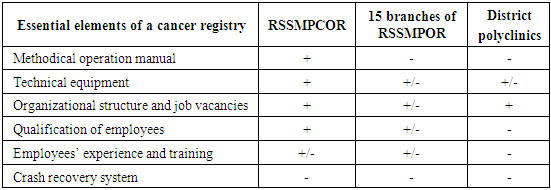
In this model, each regional branch is responsible for a specific area, where data is collected, compiled and initially analyzed which are sent to the cancer center (RSSMPCOR). According to this model, it is possible to avoid duplication, poorly collected data, as well as ensure regular collection and monitoring of filling in data from regional areas. This model has several advantages: it is possible to analyze the epidemiological characteristics in each region. The collected data can be used to plan and evaluate cancer programs, including cancer mapping. The progress of each regional branch of RSSMPCOR and district health facilities can be monitored, as well as capacity building in regional hospitals. Information on the available technical and human resources to assess the effectiveness of the cancer registry in Uzbekistan is also needed. This study outlined six main components necessary to develop a cancer registry (Tab. 1).Table 1. Essential elements for developing a cancer registry
 |
| |
|
Standard technical resources among all medical institutions of the oncology registry were found only in RSSMPCOR and its several branches (Samarkand, Bukhara, Andijan and Khorezm regions), while organizational structure and job responsibilities were found in district polyclinics.The crash recovery system is a very important element for working with information, but it was not found either in RSSMPCOR or in its affiliates. This design is intended to use existing human and technical resources, to improve its functioning and transition to a web-based cancer registration system. The developed system will be a network that includes users, who can be individuals or medical institutions, both offline and in a virtual network. The unique part of the cancer registration system in this design is the operation of a virtual private network (VPN) This technology uses hubs that will provide connectivity from / to the main center to all departments including doctors and staff. VPN hubs have encryption and authentication systems and data transmission security methods built for remote access (Fig. 4).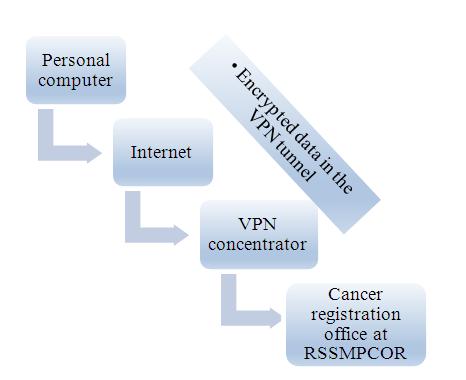 | Figure 4. Model for implementing data security using VPN |
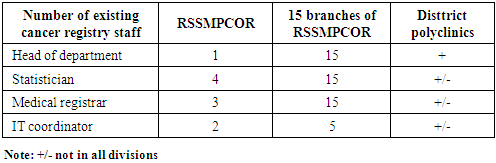
VPN (Virtual Private Network) is a technology that allows to organize virtual networks on top of existing real networks. Any VPN construction means the creation of tunnels; a tunnel means a channel between two devices through which data is transmitted. An important condition is that the data is isolated from the features of the channel construction. The device transmitting important data does it as if there was no tunnel, and the configuration of the tunnel itself is allocated in a separate task. Tunneling is organized between an application on the employee's computer and a server in RSSMPCOR and organizes connections from various medical institutions. Each user in this system can exchange and transmit data online and will be protected from hacking by unauthorized people. That is why this method of transmission over VPN is more secure than over email, because VPN has built-in encryption to protect data during transmission. The cancer registry system in this design is cost effective by using less office space and reducing overall costs. The main center (RSSMPCOR) can communicate with its branches through a secure, confidential and reliable connection, regardless of their location. Data will be transmitted only via VPN or offline method. It is forbidden to transfer data about cancer patients through personal e-mail, because the data may be intercepted or redirected to other recipients. In the current situation of data processing, which is still done manually, after entering the data in the district polyclinics, the paper data is sent to the regional branches of RSSMPCOR and then in paper form is sent to the RSSMPCOR. The advantage of this modern cancer registration system is that all data on cancer patients and their analysis does not require the work of special employees and there is no need to waste time sending this data in paper form, because all data is automatically centralized and stored on the server. Regional employees do not need to submit a paper report to RSSMPCOR on a quarterly basis because all processes will be performed electronically over a secure connection.After reviewing each medical institution related to the registration of cancer patients, the following were determined: workload and availability of staff, as well as the number of staff for cancer registration (Tab. 2).Table 2. Evaluation the number of employees for cancer registration
 |
| |
|
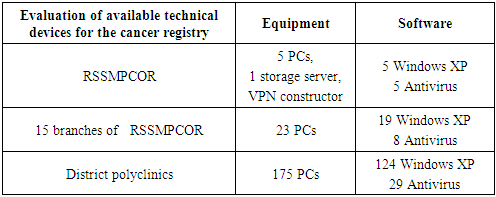
Also, an assessment of the available technical devices necessary for planning, allocating resources, for working in the cancer registration system in all regional medical institutions of Uzbekistan was made Also, the assessment of the available technical devices necessary for planning, resource allocation, for work in the cancer registration system in all regional medical institutions of Uzbekistan has been done (Tab. 3).Table 3. Evaluation of technical devices for cancer registration
 |
| |
|
4. Conclusions
The results of this study are the formation of a network plan of oncologic medical institutions for a cancer registration system with special protection for data transmission, as well as the formation of a technical structure for recording cancer patients. The system of data crash recovery in case of technical failures of the process is carried out through the technology of a virtual private network (VPN). It also provides an assessment of the number of employees associated with the work in the cancer registry and an assessment of the technical devices required for supporting the system. The successful implementation of this model will provide the basic platform for the cancer registration system in the Republic of Uzbekistan.
References
| [1] | Decree of the President No. PP-2866 of April 4, 2017 "On measures for the further development of cancer care for the population of the Republic of Uzbekistan for 2017-2021." |
| [2] | Kaprin A.D., Starinskiy V.V., Petrova G.V. "The state of cancer care in Russia in 2018" / Book // - Moscow, 2019. |
| [3] | Valkov M.Yu., Karpunov A.A., Coleman M.P., Allemany K., Pankrateva A.Yu., Potekhina E.F., Valkova L.E., Grzhibovsky A.M. Population cancer registry for science and practical health care // Human Ecology. 2017 No. 5. P. 54-62. |
| [4] | Vinogradova N. N. Possibilities of the population-hospital cancer registry in improving cancer care. Author's abstract. diss. doct. med. sciences M. -2015. |
| [5] | Brenner H, Hakulinen T (2009). Implications of in complete registration of deaths on long-termsurvival estimates from population-based cancerregistries. Int J Cancer. 125(2): 432–7. http://dx.doi.org/10.1002/ijc.24344 PMID: 19422045. |
| [6] | Buemi A (2008). Pathology of Tumours for Cancer Registry Personnel. Lyon: International Agency for Research on Cancer and International Association of Cancer Registries. The publication is posted on the website: http://www.iacr.com.fr/PathologyManualApr08.pdf. Jensen OM, Storm HH (2016). 30. Reporting of results. In: Jensen OM, Parkin DM, MacLennan R, Muir CS, Skeet RG, editors. Cancer Registration: Principles and Methods. Lyon: International Agency for Research on Cancer (IARC ScientificPublications, pp. 108–125. The publication is posted on the website: 2016. |
| [7] | Bockeria L. A., Lischuk V. A. Formation of the concept of health care using modern information and intellectual means // Scientific works of the Russian scientific and practical conference (Moscow, 2829 May 2003) -M. -2013. -P.25-29. |
| [8] | Bray F, Parkin DM (2009). Evaluation of dataquality in the cancer registry: principles andmethods. Part I: comparability, validity andtimeliness. Eur J Cancer. 45(5): 747–55. http://dx.doi.org/10.1016/j.ejca.2008.11.032 PMID: 19117750. |
| [9] | Jensen OM, Whelan S (2011). Planning acancer registry. In: Jensen OM, Parkin DM, MacLennan R, Muir CS, Skeet RG, editors. Cancer Registration: Principles and Methods. Lyon: International Agency for Research oCancer (IARC Scientific Publications, No. 95); pp. 22–28. The publication is posted on the website: http://www.iarc.fr/en/publications/pdfs-online/epi/sp95/index.php. |
| [10] | MacLennan R (2014). Items of patient informationwhich may be collected by registries. Source: Jensen OM, Parkin DM, MacLennan R, Muir CS, Skeet RG, editors. Cancer Registration: Principlesand Methods. Lyon: International Agency for Research on Cancer (IARC Scientific Publications, No. 95); pp. 43–63. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML