-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2020; 10(10): 784-787
doi:10.5923/j.ajmms.20201010.13
Received: Aug. 15, 2020; Accepted: Sep. 10, 2020; Published: Oct. 17, 2020

Morphophysiopathology of the Synovial Plicae of the Knee
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLIrismetov M. E., Tadjinazarov M. B.
Republican Specialized Scientific and Practical Medical Centre of Traumatology and Orthopedics, Tashkent, Uzbekistan
Correspondence to: Tadjinazarov M. B., Republican Specialized Scientific and Practical Medical Centre of Traumatology and Orthopedics, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Objective. The aim of this study was to determine the features of morphophysiopathology in synovial plicae of the knee. Material and methods. We studied the biopsy, surgical and sectional materials of 54 tissue samples, including 25 medial, 18 suprapatellar, 9 lateropathellar and 2 infrapatellar plicae of the knee. For optical microscopy there was used the tissue samples fixed in 10% formalin solution on phosphate buffer. Paraffin sections were stained with hematoxylin and eosin. In a histological examination of biopsy samples ofsynovial plicae, we evaluated the structural, proliferative, and inflammatory signs of the stroma. Results. It was revealed that the duration of the disease is associated with the severity of proliferation of synoviocytes, the severity of the fibroblastic reaction and the severity of the macrophage reaction. In the presence of obvious clinical course, pathological changes in pronounced manifestations of an inflammatory reaction and proliferative infiltration were determined. In the older age group, these phenomena were less pronounced than in younger patients. In patients with acute knee trauma, insignificant focal lymphoid and plasma cell infiltration was determined. With a prolonged clinical course and the formation of chronic synovitis, a slight severity of changes was noted, while the macrophage reaction was significantly pronounced. In cases of traumatic and inflammatory nature of the synovial plicae syndrome, the monolayer mesotheliocytes emerged above the fibrous surface. Conclusion. Pathological synovial plicae of the knee depending on their type, nature of damage and stage of development have various structural transformations, the severity of proliferative and inflammatory reactions. The gradual progression of the pathological process with the prolonged existence of synovial plicaeof the knee leads to an increase in inflammatory processes and the formation of severe chronic synovitis, the multiply increasing risk of chondromalation and recurrent synovitis.
Keywords: Knee, Physiological and pathological synovial plicae, Morphology
Cite this paper: Irismetov M. E., Tadjinazarov M. B., Morphophysiopathology of the Synovial Plicae of the Knee, American Journal of Medicine and Medical Sciences, Vol. 10 No. 10, 2020, pp. 784-787. doi: 10.5923/j.ajmms.20201010.13.
1. Introduction
- According to the numerous literature data, 4 types of synovial folds of the knee are found. Pathological changes in synovial folds are due to a number of reasons. Possible causes may be acute direct and indirect injuries or chronic traumatization in the process of sports activities, localized hemorrhages, etc. [1,2,3].In the process of progression of the process, elasticity is lost, the synovial membranes thicken and become inflamed. The inflammatory process causes plicae fibrosis with subsequent intra-articular disorders [4,5]. A thickened and inelastic synovial plicae prohibite with the normal functioning of the knee joint and can cause gonarthrosis [6].The aim of this study was to determine the features of morphophysiopathology in synovial plicae of the knee.
2. Material and Methods
- The basis of the study was the biopsy, surgical and sectional materials of 54 tissue samples, including 25 medial, 18 suprapatellar, 9 lateropathellar and 2 infrapatellar plicae of the knee. Optical micrographs were obtained with an Axioscop 40 - ZEISS microscope connected to a digital camera and a computer. All photomicrographs were processed and data saved on a computer using Microsoft Windows XP-Professional software. For optical microscopy there was used the tissue samples fixed in 10% formalin solution on phosphate buffer. Paraffin sections were stained with hematoxylin and eosin. In a histological examination of biopsy samples of synovial plicae, we evaluated the structural (changes in the synovial membranes), proliferative (fiber hyperplasia, degree of granulation, fibroblastic reactions and angiomatosis), and inflammatory signs (plasma cell, lymphoid and macrophage infiltration) of the stroma.The results of this study are expected to provide a scientifically proven justification for the correctness of the chosen treatment tactics – surgical arthroscopic intervention in the presence of pathological synovial plicae of the knee.
3. Results
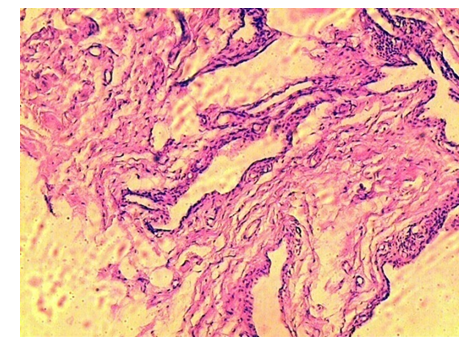
- Histological examination of the bioptic material of the normal synovial plicae revealed have the following morphological characteristics:- thin layer of fibrous, fatty and vascular membranes,- elasticity, which is determined by the high content of fibroblasts.Optical studies showed that the basis of all four types of synovial plicae is the same and composed of a fibrous loose conjunctive tissue with a rather large volume of microvessels and layers of fat cells, which are located under the covering layer of synoviocytes (Fig. 1). This conditions are determined by their common genesis - the origin from the synovial membrane of the knee.
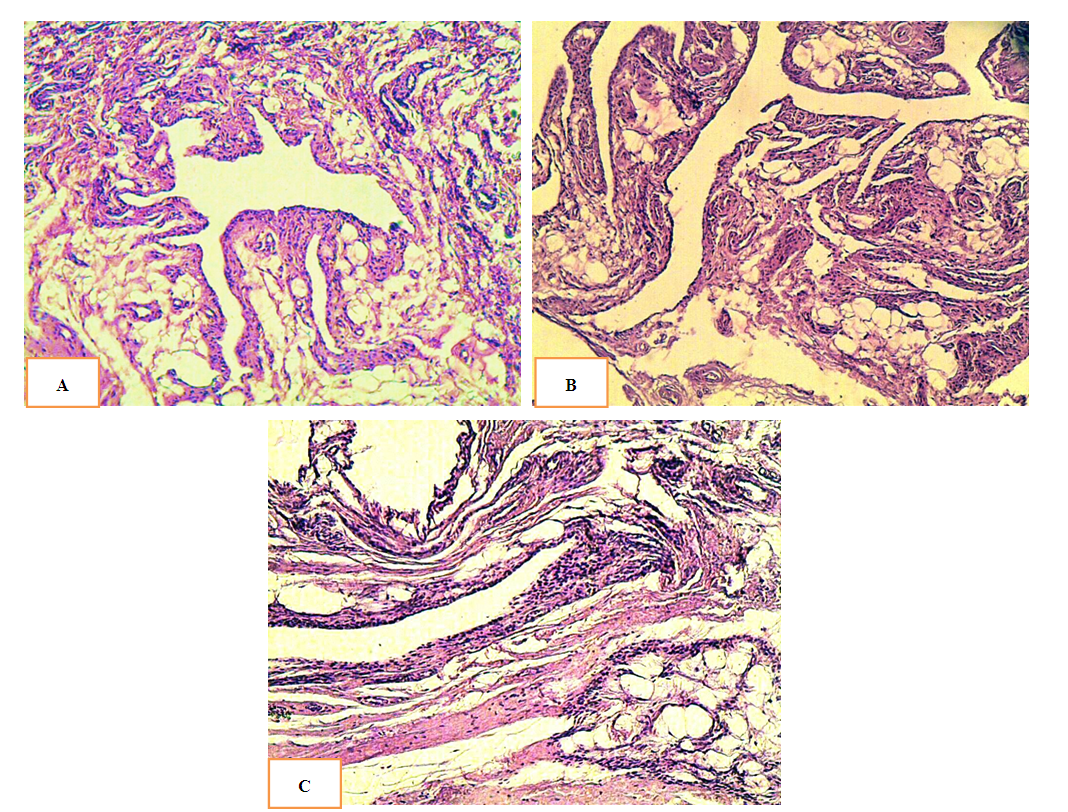 | Figure 1. Non-fibrous conjunctive tissue medial plicae (A), suprapatellar (B) and lateropatellar plicae (C), blood vessels with lumens of different caliber, accumulations of fat cells |
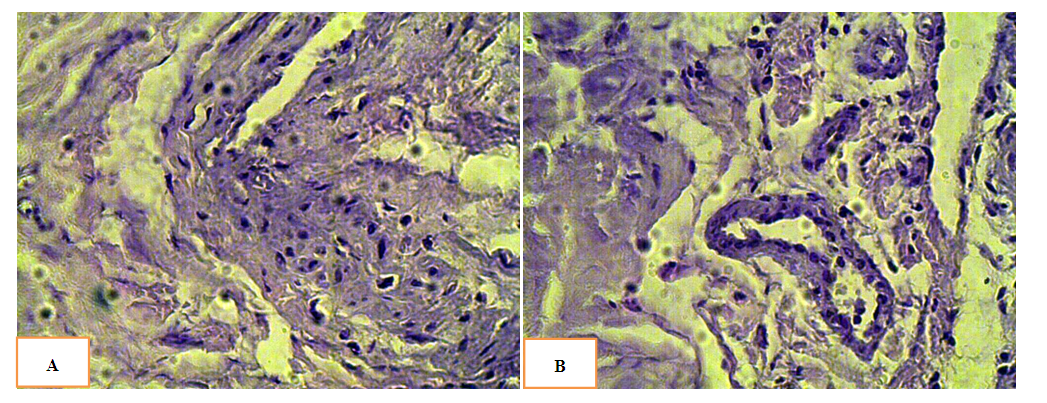 | Figure 2. Weakly expressed structural changes. Moderate inflammatory perivascular infiltration: A) medial plicae in case of polyarthritis; B) suprapatellar plicae with shaped elements of blood visible in the lumen of the vessel |
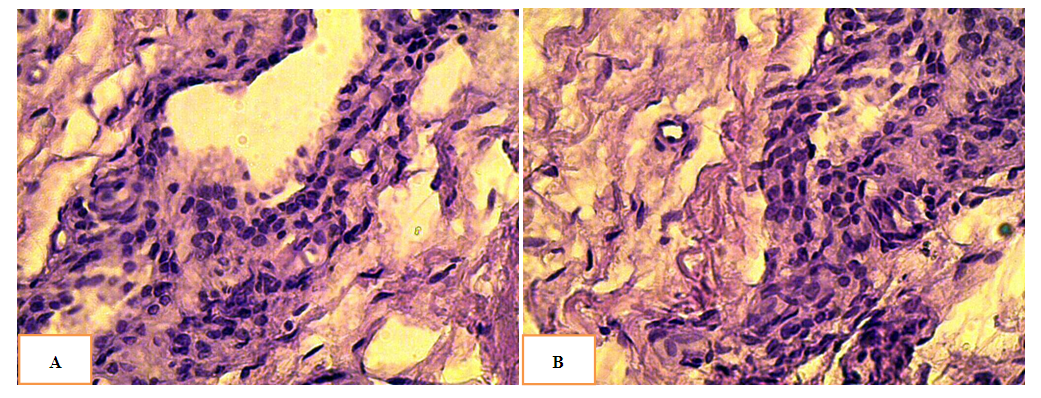 | Figure 3. Severe inflammatory perivascular infiltration: A) medial plicae; B) suprapatellar plicae. Pronounced villous hyperplasia with prolonged existence of the knee pathology |
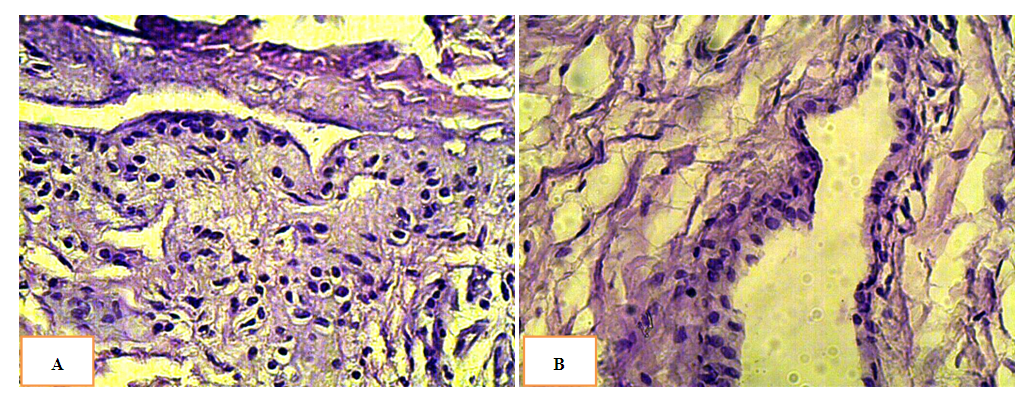 | Figure 4. A) Lateral synovial plicaewith severe inflammatory perivascular infiltration of; B) Medial plicaewith rough fibrous connective tissue, vessels of different caliber and gaps between the fibers |
 | Figure 5. Medial synovial plicae: severe inflammatory perivascular infiltration, false multi-row mesothelium |
4. Conclusions
- The pathological synovial plicae of the knee, depending on their type, damage nature and the stage of development, have various structural transformations, the severity of proliferative and inflammatory reactions, signs of focal lymphoid or plasma cell infiltration in most patients.Pathological suprapatellar and medial plicae undergo pronounced polymorphism of wall layers, dissection and swelling in cases of acute knee traumatization and the addition of an inflammatory process. In most cases, the structural disorders are a consequence of the long existence and progression of the pathological process.In addition, the gradual progression of the pathological process leads to an increase in inflammatory processes and the formation of pronounced chronic synovitis, increase the risk of degenerative-dystrophic processes, chondromalation and recurrent synovitis.