-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2020; 10(10): 766-768
doi:10.5923/j.ajmms.20201010.08
Received: Jul. 3, 2020; Accepted: Sep. 30, 2020; Published: Oct. 15, 2020

Vitamin D Efficiency for Prevention of Pregnancy Complications
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLDzhumanov B. A., Zufarova S. A.
Tashkent Pediatric Medical Institute, Tashkent, Uzbekistan
Correspondence to: Dzhumanov B. A., Tashkent Pediatric Medical Institute, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

When studying the level of vitamin D in the risk group for pre-eclampsia development pregnant women, reliably low rates were found in relation to pregnant women with physiological course of pregnancy without complications. Dependence of preeclampsia development in at-risk pregnant women on prophylactic vitamin D intake have been studied too. We have hypothesized that pregnant women having taken vitamin D have a more favorable course of pregnancy, which in turn affected the state of newborns. Therefore we have found that hypoxia of the fetus was observed 2 times less in the group of pregnant women who were taking vitamin D since 20 weeks than women who were not taking vitamin D.
Keywords: Vitamin D deficiency, Pregnancy complications, Pre-eclampsia
Cite this paper: Dzhumanov B. A., Zufarova S. A., Vitamin D Efficiency for Prevention of Pregnancy Complications, American Journal of Medicine and Medical Sciences, Vol. 10 No. 10, 2020, pp. 766-768. doi: 10.5923/j.ajmms.20201010.08.
- At present, vitamin D deficiency is considered to be a global health problem affecting a wide range of acute and chronic diseases [1,2].Over the past ten years, the physiological role of 25 (OH) 2D3 has been widely studied, but data on its role in human reproduction are limited. Since vitamin D receptors have been found in reproductive tissues, including the ovaries, uterus, placenta, testicles and pituitary gland, vitamin D association with many reproductive health outcomes is requested [5,6]. Vitamin D induces more than 3000 genes, many of which play a role in fetal development. 26 of them have a wide range of proven biological actions, including inhibition of cell proliferation and induction of final differentiation, inhibition of angiogenesis and renin production, stimulation of insulin production and production of macrophages, apoptosis induction [3,8]. Hypertension during pregnancy and especially preeclampsia (PE) are the most studied pregnancy complications. PE syndrome is defined as the occurrence of hypertension and proteinuria after 20 weeks of pregnancy, and with a prevalence of 3-5% of all pregnancies worldwide, it is the leading cause of maternal mortality and perinatal morbidity and mortality [4,7].Purpose of the study: to evaluate the role of vitamin D during gestation in pregnant women at risk for pregnancy complications.
1. Materials and Methods
- The study enrolled 90 pregnant women with 18-22 weeks gestation period. The age gradation was from 19 to 40 years, the average age was 27.9±1.5 years. Based on cohort observation we identified a risk group for PE development consisting of 60 pregnant women.Vitamin D was determined in all cases. Vitamin D was determined by ELISA method on Elecsys-2010 (Switzerland). M.Hollick (2005) criteria were used to evaluate serum vitamin D status. Vitamin D level is considered to be sufficient at 25(ON)D level in serum over 30 ng/ml. Vitamin D deficiency means a decrease in serum concentration of 25(OH)D below 20 ng/ml (50 nmol/l); vitamin D deficiency is the concentration of 25(OH)D in serum preserved in the range of 21-29 nanograms/ml. All pregnant women were prescribed calcium 1.5 g and vitamin D in a dose of 1500 units. During observation 30 pregnant women did not take vitamin D (comparison group), and 30 followed the prescription of a gynecologist (main group); 30 patients with physiological course of pregnancy were included in the control group. Vitamin D level was administered again at admission for childbirth. Statistical processing of the study results was performed using Statistica for Windows packages (version 6.1) using parametric and non-parametric statistics (Student, Mann - Whitney criteria).
2. Research Results
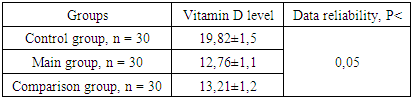
- Based on our studies, we found that in PE risk pregnant women, vitamin D was significantly decreased with respect to the control group (Table 1).
|
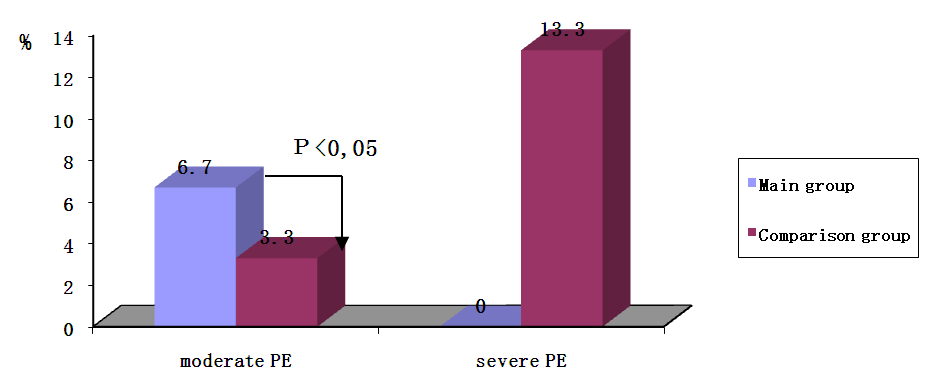 | Figure 1. Percentage of PE development among the surveyed pregnant women, depending on the use of vitamin D |
|

3. Conclusions
- Thus, it can be proved that vitamin D deficiency is a risk factor for the development of PE, an increase in vitamin D- level confirms the presence of polyorganic failure, which is also a risk factor for obstetric complications. The increased endothelion level in the serum causes an increase in blood pressure. As experts from the World Health Organization (2010) emphasized, the maternal status of vitamin D is very important in the prevention of complications during pregnancy.