-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2020; 10(10): 755-758
doi:10.5923/j.ajmms.20201010.05
Received: Aug. 15, 2020; Accepted: Sep. 8, 2020; Published: Sep. 28, 2020

Our Experience in Arthroscopic Treatment of Tibial Plateau Fractures
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLIrismetov M. E., Shamshimetov D. F., Tadjinazarov M. B., Kholikov A. M., Usmonov F. M., Rajabov K. N.
Republican Specialized Scientific and Practical Medical Centre of Traumatology and Orthopedics, Tashkent, Uzbekistan
Correspondence to: Tadjinazarov M. B., Republican Specialized Scientific and Practical Medical Centre of Traumatology and Orthopedics, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Objective. The aim of the study was to improve the treatment outcomes for tibial plateau fractures using recent minimally invasive surgical methods. Material and methods. The prospective study. Fractures of the tibial plateau in 65 patients with were treated in the sports trauma department of the Republican Specialized Scientific and Practical Medical Centre of Traumatology and Orthopedics (Tashkent, Uzbekistan) for the period 2015-2020. In 69% (n=45) cases, a fracture of the external condyle was diagnosed, in 30.7% (n=20) cases - a fracture of the internal condyle. There were 46 men (70.8%) and 19 (29%) women. Main complaints: pain, swelling and limitation of knee movement. The following instrumental imaging methods were used: X-ray, computed tomography and magnetic resonance imaging. In addition, the patients underwent densitometry and doppler ultrasonography of the lower extremities. Knee arthroscopy was performed in all cases. Fresh cleft-depression fractures were treated with reposition and fixed with cannulated cancellous screws. The combination of fractures with soft tissue injuries of the knee was observed in 11 (22%) cases in lateral meniscus damages; in 6 (12%) cases with medial meniscus damage; in 10 (20%) cases with anterior cruciate ligament damage; in 2 (4%) damages of posterior cruciate ligament and in 9 (18%) patients with damage to the lateral ligament. Results. We studied the early outcomes at 3 and 6 months in 35 (70%) patients. Long-term outcomes were studied in 17 (34%) patients. Good results were noted in 48 (96%) patients, satisfactory in 2 (4.1%) patients (in whom additional plastic surgery of the bag-ligamentous apparatus was performed). In the postoperative period, immobilization was maintained until the sutures were removed, and the axial load was resolved after 3-6 months. after surgery, depending on the volume of the bone defect of the tibial condyle. Conclusion. The proposed method of minimally invasive techniques under arthroscopic control ensures the accuracy of reduction and the reliability of fixation of bone fragments, shortens the surgical duration, reduces intraoperative blood loss, leaves a minimal cosmetic defect and helps to shorten the hospital stay.
Keywords: Knee, Tibia, Plateau, Arthroscopic diagnostics and surgery
Cite this paper: Irismetov M. E., Shamshimetov D. F., Tadjinazarov M. B., Kholikov A. M., Usmonov F. M., Rajabov K. N., Our Experience in Arthroscopic Treatment of Tibial Plateau Fractures, American Journal of Medicine and Medical Sciences, Vol. 10 No. 10, 2020, pp. 755-758. doi: 10.5923/j.ajmms.20201010.05.
Article Outline
1. Introduction
- Treatment of tibial plateau fractures remains a major challenge in orthopedics and traumatology. The significant proportion of fractures of the tibial condyles, accounting for 2% to 5% of all bone fractures, up to 30% of all injuries of the lower extremities and up to 60% of movable joint injuries, determines the problem urgency [1,2]. High-energy shear and compressive forces acting on the knee create significant tension in the menisci and ligaments and increase the risk of injury, the overall incidence of which is reported to be 39% to 99% and 16.7% to 57%, respectively [3]. Damage to soft tissues correlates with increased displacement of fragments in fractures of the tibial plateau [4]. The prevalence of concomitant meniscus injuries in fractures of the tibial plateau varies according to various sources from 38.9% to 99.0%, [5].The frequency of unsatisfactory long-term anatomical and functional treatment results reaches 6-39%, and disability - 6% [6]. The early development of post-traumatic deforming arthrosis of the knee joint in 60-80%, the occurrence of persistent contractures in 29-50% and deformities of the knee joint in 12-20% of patients with fractures of the tibial condyles encourage surgeons to introduce modern highly informative methods for assessing the nature of damage to the condyles and intra-articular soft tissue structures of the knee joint, as well as new approaches to the reduction and fixation of bone fragments using modern techniques of internal stable-functional osteosynthesis. In recent years, arthroscopy has been increasingly used at different stages of surgical intervention [7].Closed reposition of tibial fragments is a difficult task, and it is possible to restore the congruence of the articular surfaces only in the absence of impressions of bone fragments. However, it is even more difficult to keep the bone fragments in the correct position during conservative treatment. In addition, the conservative method cannot meet the requirement for early development of movements in the damaged joint, which inevitably leads to the development of contractures. Therefore, plaster immobilization in severe fractures of the localization under consideration practically guarantees the development of persistent contractures and rapidly progressing deforming arthrosis of the knee joint, lengthens treatment and rehabilitation, and also often leads to limitation or disability.Early development of post-traumatic deforming arthrosis of the knee joint in 60-80%, the occurrence of persistent contractures in 29-50% and deformities of the knee joint in 12-20% of patients with fractures of the tibial condyles encourage surgeons to introduce modern highly informative methods for assessing the nature of damage to the condyles and intra-articular soft tissue structures of the knee joint, as well as new approaches to the reduction and fixation of bone fragments using modern techniques of internal stable-functional osteosynthesis [8].The improvement of the surgical treatment of complex fractures of the tibial condyles continues, which requires a scientific search for both more perfect structures for osteosynthesis and new methods of their application. It is the internal fixation that develops especially intensively, which is most reliably carried out by a fairly wide open revision of the articular surfaces and fixation of intermediate bone fragments under visual control. In addition, subsequent development, which is key to restoring movement, requires the absence of wire wounds in the projection of the tibial condyles, where trauma to the mobile skin is possible. The latter point narrows the indications for the use of external fixation devices, which are used during combined osteosynthesis in severe open trauma or in the presence of contraindications to internal osteosynthesis [9].At different stages of surgical intervention, arthroscopy is increasingly used, which allows you to visually monitor the position of fragments and fixators, restore ligaments and menisci, and remove free intraarticular bodies. Despite the widespread use of various methods for stabilizing bone fragments and the increasingly frequent arthroscopic accompaniment of surgical interventions, traditional surgical tactics are not without a number of disadvantages. According to many surgeons, the most significant among them are: the lack of clear criteria that determine the choice of the most adequate method of reduction and the method of fixation of fragments depending on the nature and complexity of bone damage, the optimal degree of correction of the biomechanical axis of the limb during reduction condyles, as well as the place of endovideosurgical technologies in the complex treatment of patients.Purpose. Improving the results of treatment of fractures of the tibial plateau, through the use of modern methods of treatment.
2. Material and Methods
- The study was based on 65 patients with fractures of the tibial condyles who received treatment in the sports injury department of the RSNPMTSTO for the period 2015-2020. Moreover, patients with fractures of the external condyle accounted for 69% (n = 45), and the internal condyle - 30.7% (n = 20). Among them were 46 men (70.8%), 19 women (29%) who complained of pain, edema, limitation of the knee joint movement, deformity and hypotrophy of the soft tissues of the thigh and lower leg.In order to determine the complexity, nature of the fracture and tactics of fracture treatment, the following instrumental imaging methods were used: radiography, MSCT and MRI. In addition, the patients underwent densitometry and Doppler ultrasonography of the lower extremities.In 19 (29%) patients, the X-ray revealed a fracture without displacement of bone fragments, MRI or MSCT showed intra-articular fractures of the condyles with displacement of bone fragments.
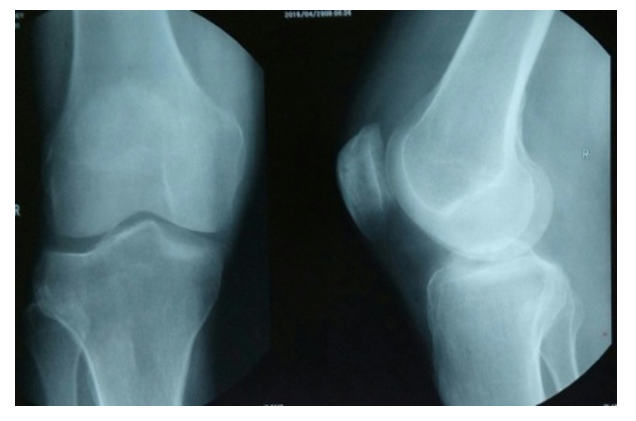 | Figure 1. Knee X-ray. Fracture of the outer condyle of the tibia |
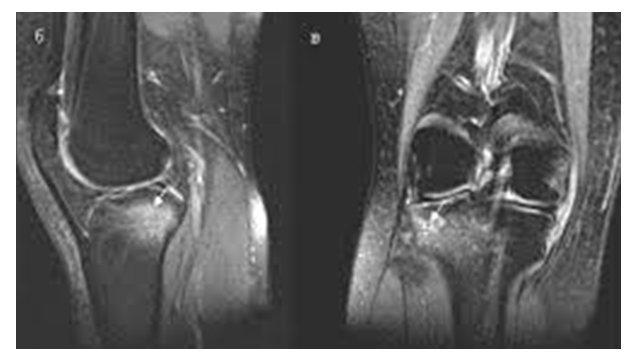 | Figure 2. MRI. Fracture of the external condyle |
3. Clinical Case, Results and Discussion
- Patient K. was injured when falling from a height. X-ray and CT-scanning showed a comminuted fracture of the external condyle with displacement of bone fragments (Fig. 3, 4).
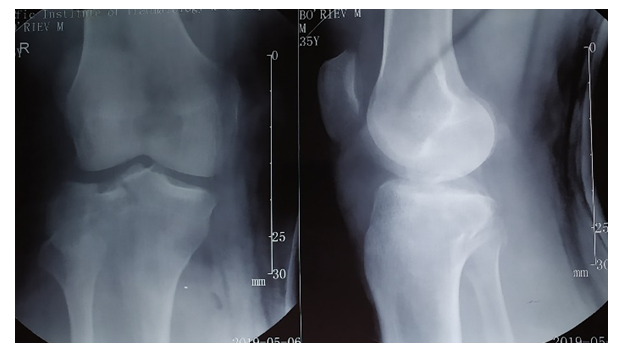 | Figure 3. X-ray of the right knee joint |
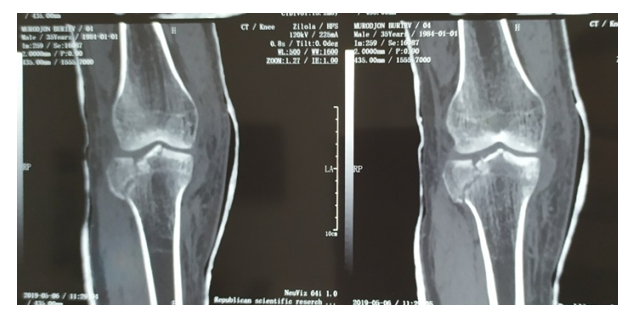 | Figure 4. MSCT of the right knee joint |
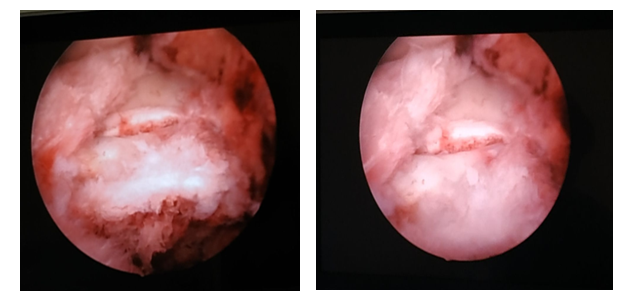 | Figure 5. Arthroscopy and osteosynthesis with cancellous screws |
 | Figure 6. X-ray of the right knee joint was performed. Bone fragments in satisfactory standing |
 | Figure 7. Patient’s condition after 3 months after surgery |
4. Conclusions
- The proposed method of surgery ensures the accuracy of reduction and reliability of fixation of bone fragments, shortens the duration of surgery, reduces intraoperative blood loss and shortens the duration of pain syndrome, minimal risk of infectious complications, leaves a minimal cosmetic defect, and helps to shorten the length of hospital stay.The use of this technique of surgical treatment allows to restore the normal range of motion in 3-6 months in most patients with fractures of the tibial condyles. Arthroscopy of intra-articular fractures of the tibial condyles allows an accurate diagnosis.