-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2020; 10(9): 725-727
doi:10.5923/j.ajmms.20201009.20
Received: Aug. 17, 2020; Accepted: Aug. 30, 2020; Published: Sep. 15, 2020

Comparative Characteristics of Morphometric Parameters of Children with Scoliosis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSh. M. Kamalova, Sh. J. Teshaev
Anatomy, Clinical Anatomy (OSTA) Department, Bukhara State Medical Institute, Bukhara, Uzbekistan
Correspondence to: Sh. M. Kamalova, Anatomy, Clinical Anatomy (OSTA) Department, Bukhara State Medical Institute, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Scoliosis is called a biological tragedy of humanity. In scoliosis, there are violations not only of the functions of the musculoskeletal system, but also the emergence and development of negative shifts in the functioning of internal organs, cardiovascular, respiratory nervous systems and anthropometric indicators of physical development of children, which is primarily due to the process of pathological curvature of the spine. We studied the results of a survey of 80 children aged 10 years, of which the control group consisted of 40 healthy children and 40 children with scoliosis. During the research, it was found that due to severe deformity of the vertebral column, children with scoliosis of 10 years of age are shorter, their body weight and breast parameters are less than in healthy children.
Keywords: Morphometric indicators, Scoliosis, Violation of posture, Anthropometry, Chest circumference, Body length
Cite this paper: Sh. M. Kamalova, Sh. J. Teshaev, Comparative Characteristics of Morphometric Parameters of Children with Scoliosis, American Journal of Medicine and Medical Sciences, Vol. 10 No. 9, 2020, pp. 725-727. doi: 10.5923/j.ajmms.20201009.20.
Article Outline
1. Introduction
1.1. The Relevance of the Problem
- Scoliosis is a common disease of the musculoskeletal system, which is characterized by a multi-plane deformity of the vertebral column and chest. Due to the pronounced deformation of the chest, its full excursion during breathing is difficult, which is accompanied by a violation of the functions of organs and systems of the body [1]. While 20% of cases of scoliosis can be attributed to neuromuscular, syndromic or congenital disorders, up to 80% of all scolioses are called "idiopathic" or of unknown etiology [2,3,4]. According to some authors, the leading causes of this disease are genetic predisposition and metabolic disorders in the body [5,6]. According to modern literature, the prevalence rate of idiopathic scoliosis ranges from 0.47-5.2%, on average 2-3% of the total population. The severity and prevalence of scoliosis in girls is higher than in boys [7]. However, some authors claim that scoliosis occurs in 2-9% of children and adolescents under the age of 16, and the prevalence of this severe disease in school-age children reaches 15-30% or more [8,9]. According to the literature, it was found that girls with idiopathic scoliosis were generally taller and heavier than healthy children. In particular, it was found that girls with this disease were significantly taller and heavier at age 12, while boys with scoliosis were significantly taller at age 14 than their healthy peers [10].Other studies have shown that girls with scoliosis were generally taller, with a longer arm span, but with a lower body mass index than healthy children in the control group. It was found that girls with a complex degree of scoliosis were significantly shorter in height and arm span at the age of 12 years, but caught up and overtook the control group at the age of 14 to 16 years [11,12,13]. Also, even though the Cobb angle method is the standard way of quantifying the curvature of the scoliotic spine, it is difficult to detect small changes in curvature due to errors in the measurements [14,15].The spine deformity progress in children is directly related to their continued growth. The lack of full etiology understanding doesn’t allow predicting the course of scoliosis [16,17].There is no objective data that determines the possible development of scoliosis in the early stages. There is no consensus on the early diagnosis and prevention of possible consequences of scoliosis, which justifies the need for research in this area.
1.2. The Aim of the Study
- The aim of the study was to study the anthropometric indicators of 10-year-old children with scoliosis and compare them with the anthropometric indicators of healthy children.
2. Materials and Research Methods
- The research was conducted at secondary school No. 2 and boarding school No. 23 in Bukhara for children with scoliosis. The results of examination of 40 children (20 boys and 20 girls) aged 10 with idiopathic scoliosis of thoracic localization of I - III degree according to Chaklin were studied. All examined children were divided into 2 groups by simple randomization, comparable in age, gender, and clinical and functional indicators. The main group consists of 40 children with scoliosis, and the control group consists of 40 healthy children (20 boys and 20 girls). The method of anthropometric research of children was used for anthropometric measurements (guidelines of N. H. Shomirzaev, S. A. Ten and I. Tukhtanazarova, 1998).The diagnosis of idiopathic scoliosis was established on the basis of a standard examination conducted in the clinic and including clinical and neurological, instrumental, radiographic methods of investigation (radiography) of the craniovertebral region, thoracic and lumbar spine. The assessment of anatomical and anthropometric features (measurement of the trunk, chest, waist, limbs and vertebral column using a centimeter tape and a tasometer) of the vertebrae of the thoracic and lumbar spine was carried out on the basis of data obtained by digital radiography. Radiography was performed in the patient's standing position using the TITAN 2000 M device (Korea, 2012), followed by statistical data processing.Mathematical processing was performed directly from the General Excel 7.0 data matrix using the capabilities of the STTGRAPH 5.1 program, and the standard deviation and representativeness errors were determined.
3. The Results of the Study
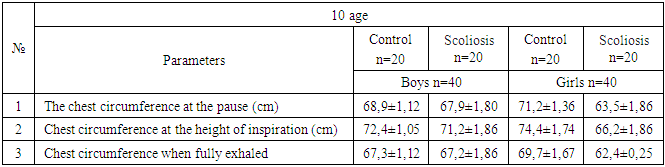
- All examined children showed clinical and radiological signs of scoliosis, the direction of the thoracic scoliotic arch was right-sided (42,5%) or left-sided (57,5%). Studies have shown that the height of 10 year old healthy male children ranges from 1,31 cm to 147 cm, with an average of 138.0±0.99 cm. The body weight ranged from 25 kg to 45 kg, with an average of 30.3±1.24 kg. In a study of children with scoliosis, it was found that the height of 10 year old boys ranged from 128 cm to 136 cm, with an average of 131.8±1.05 cm. The average body weight is 30.0±1.74 kg (from 24 kg to 52 kg).The height of 10 year old healthy girls ranged from 136 cm to 155 cm, on average it was equal to 140.7±1.18 cm. The average body weight is 35.4±1.74 kg (from 28 kg to 56 kg).Studies have shown that the height of 10 year-old girls with scoliosis ranges from 118 cm to 139 cm, with an average of 123.0±1.3 cm. The body weight varied from 22 kg to 29 kg, with an average of 25.4±0.62 kg.Conducted anthropometric studies among 10 year-old male and female children with scoliosis have shown that the growth parameters of male children are 1.05 times, and that of female children are 1.09 times behind the parameters of healthy children. The breast circumference in the pause in boys with scoliosis of 10 years of age is 1.01 times less, and in girls of this age with scoliosis is 1.12 times less than in healthy children. The chest circumference at the height of inspiration in boys with scoliosis 10 years of age is 1.02 times less, and in girls 1.12 times less, in contrast to healthy children of this age. The breast circumference at full exhalation in male children of 10 years of age with scoliosis is 1.0 times less, and in girls it is 1.12 times less in comparison with healthy children (see the table).
|
4. Discussion and Conclusions
- Several risk factors have been identified by previous studies as affecting the progression of AIS. Age is commonly cited as a key indicator of progression. Younger patients at diagnosis carry a greater risk for progression due to the onset of puberty. In children with Idiopathic Scoliosis, gains in sitting height need to be compared with angular development of the spine [18,19,20].Based on the data obtained, it was found that 10-year-old children with male and female scoliosis lag behind in height and body weight than their healthy peers. This is due to the fact that the bone system of children at this age is in the development stage, but with scoliotic disorders, the bone system is delayed in development in children.The chest circumference in the pause, at the height of inspiration and at full exhalation in 10 year old boys and girls with scoliosis is less. X-ray and anthropometric studies have shown that in scoliosis in children of 10 years of age, due to pronounced curvature of the vertebral column, the chest is deformed, and this leads to the fact that the parameters of the breast circumference are significantly reduced in comparison with the same parameters of healthy children.