Sharipov Alisher Mirkhamidovich, Artikova Magina Akmalovna
Department of Emergency Pediatrics, Disaster Medicine, Tashkent Pediatric Medical Institute
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Metabolic disorders nephropathy (MDN) is a large group of kidney diseases with various etiologies and pathogenesis, but combined in that their development is associated with metabolic disorders that can lead to changes in the functional state of the kidneys or structural changes at the level of various structures of the nephron. Statistical variation in the registration of MDN ranges from 27% to 64% in the structure of the incidence of the urinary system in children, and in every day practice of a pediatrician, almost every third patient has a syndrome of metabolic disorders in the urine. We analyzed the influence of risk factors on the formation of secondary oxalate nephropathies in children. Therefore, our results showed that decrease in the volume of fluid consumed, artificial feeding, a violation of the nature of nutrition in children contributes to the formation of calcium oxalate crystalluria and secondary oxalate nephropathy in childhood.
Keywords:
Metabolic nephropathy, Secondary oxalate nephropathy, Crystalluria, Calcium oxalate crystalluria, Risk factors, Exogenous factors
Cite this paper: Sharipov Alisher Mirkhamidovich, Artikova Magina Akmalovna, Analysis of the Influence of Risk Factors on the Formation of Secondary Oxalate Nephropathies in Children, American Journal of Medicine and Medical Sciences, Vol. 10 No. 9, 2020, pp. 715-718. doi: 10.5923/j.ajmms.20201009.18.
1. Introduction
Despite significant progress in the development of pediatric nephrology, over the past decade, the problem of kidney disease remains relevant. At the present stage, the issue of the spread of pathology of the urinary system organs and risk factors for its development is debatable. In pediatrics, the problem of the formation of metabolic nephropathy in children is widely discussed [9]. Statistical data show that in the structure of the pathology of the urinary system in the pediatric population, the share of metabolic nephropathy accounts for from 27% to 64% of cases of morbidity [2]. It was found that among metabolic nephropathies, the frequency of occurrence of secondary oxalate nephropathy (SON) associated with impaired oxalic acid metabolism is significantly higher [7] and ranges from 68 to 71% in the crystalluria structure [1]. An excess of the level of oxalate in the urine helps to establish calcium oxalate crystalluria (COC), and a significant increase in plasma oxalate should alert doctors to the development of nephropathy and nephrolithiasis. The spectrum of diseases associated with hyperoxaluria ranges from recurrent kidney stones, nephrocalcinosis and urinary tract infections to chronic kidney disease and end-stage renal disease.At present, there is a shift in the peak incidence of SON towards an earlier age. In this regard, the question of the risk factors under the influence of which the development of SON is noted is urgent. The factors of exogenous and endogenous character are distinguished [4]. In our work, we wanted to analyze the factors of an exogenous nature that contributed to the development of COC and SON. The exogenous risk factors include: climatic (dry and hot climate), the composition of drinking water and insufficient drinking regime [13,6], the nature of food [4,5,6,7] including ketogenic nutrition [11].Considering the above data, in our study we analyzed the impact of exogenous factors on the development of COC and SON in children.Research material: In order to identify exogenous factors, the analysis of data from 76 children with SON at the age from 6 months to 7 years was carried out. The control group consisted of 30 children of the same age.
2. Research Methods
The following data were taken from the child's outpatient card: age, gender, life history, medical history of the child, frequency of prescribed and taken antibiotic therapy over the last 6 months. Parents of children were questioned for the presence of chronic diseases, the nature and characteristics of the diet of children under 12 months and after, the nature of the volume of fluid consumed during the day. We determined anthropometric indicators (height, weight of the child), and also measured blood pressure (systolic and diastolic), and calculated the mass-to-body index. The diagnosis of oxalate nephropathy was verified on the basis of generally accepted clinical and laboratory tests (complete blood count, urine analysis, urine flow cytometry, urine analysis according to Nechiporenko, determination of oxalates in daily urine, biochemical blood analysis: determination of total protein, albumin, creatinine, calcium, potassium, phosphorus, magnesium in the blood) and instrumental research methods (ultrasound). All children in the study groups were tested for intestinal microflora. The determination of the daily excretion of oxalates was carried out by the titrimetric method of permanganatometry. Hyperoxaluria was an increase in oxalates above 0.5 mg / kg / day.
3. Results and Discussion
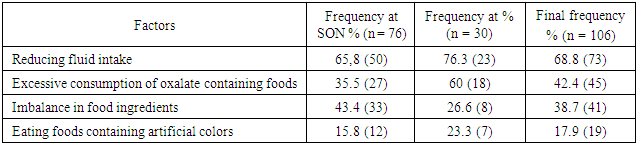
Our results showed that in more than 68% of cases in both compared groups, the fact of a decrease in the volume of fluid consumed with some, but not significant excess of the number in the control group of children was established. For the rest of the studied risk factors, significant was observed in the main study group. We identified an imbalance in food consumption, which was noted more often in the main group (43.4%) compared with the control group (26.6%). However, we found excessive consumption of products containing oxalates in both study groups, but to a greater extent in the control group of children (60%) and almost two times less (35.5%) in the main study group. In our research, we also found cases of abuse of products containing artificial colors. In the main group, we established this factor in 15.8% of cases, and in the control group - in 23.3% of cases, i.e. with an insignificant difference.Table 1. Frequency of exogenous factors in children with COC and SON
 |
| |
|
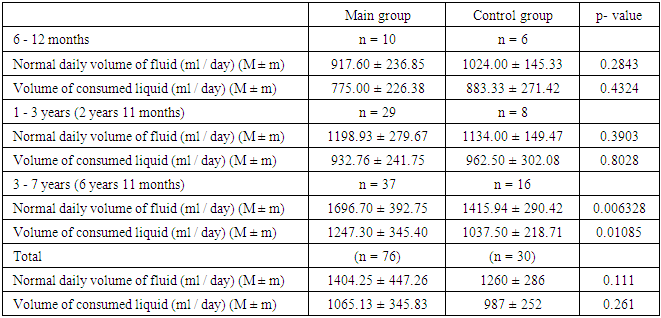
Despite the fact that violation of the drinking regimen as an exogenous factor was more common in the control group, in our study we compared the level of deficit in the volume of fluid consumed during the day in children in both groups, depending on age, based on the existing body weight.The analysis of the volume of fluid consumed during the day showed, depending on the age and weight of the child (see Table 2), that the deficit of the received fluid in infants of the main group was 16%, and in the control group - 14%, while in children aged 1 to 3 years in the main group, the deficit of consumed water was 29%, and in the control group - 18%. In children aged 3 to 7 years in the main and control groups, the deficit of consumed water was the same 36%.Table 2. Analysis of fluid intake per day in children in the study groups
 |
| |
|
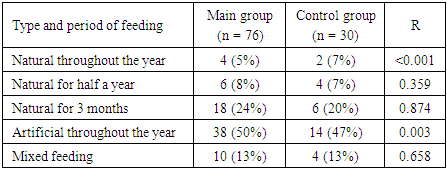
Thus, despite the fact that water deficiency was not significantly more often as a risk factor of an exogenous nature for the development of oxaluria was noted in the control group, the degree of water deficiency was significantly more pronounced in oxaluria in children of the main group, i.e. with signs of SON. In turn, a more pronounced decrease in the volume of urine leads to an increase in its concentration, loss of bicarbonates and urinary acidosis, which creates favorable conditions for the onset of crystalluria. Therefore, from a theoretical and practical point of view, the problem of insufficient consumption of the volume of drinking is of considerable interest, and the degree of inadequacy of the drinking regime is considered as one of the main risk factors for the development of SON.In order to further study the exogenous risk factors for the development and maintenance of hyperoxaluria, we analyzed the nature of nutritional disorders in the studied children. According to a number of authors, the occurrence of metabolic disorders in childhood is influenced by late attachment to the breast, early transfer to mixed or artificial feeding [2,13], which can cause deviations in the health status of children and an increase in the number of nephrological diseases. Therefore, in our study, we analyzed the nature of feeding in infants.The study showed (table 3) that in the studied groups the most of the children who were artificially fed (50% and 47%, respectively) were anamnestically identified. At the same time, in the main group there was not a significantly greater number of "artificial" people than in the control group. The same picture was observed in the group with a short period of breastfeeding, when the frequency of the number of children exceeded, but not significantly, in the main group (24% and 20%, respectively). The smallest number in both compared groups was identified as breastfed children (5% and 7%, respectively). It should be noted that in both groups, an equal amount of mixed and natural duration of up to 6 months was found in children in both groups. types of feeding.Table 3. Comparative characteristics of the types of feeding in children in the first year of life in the studied groups of patients with SON (main) and COC (control)
 |
| |
|
Consequently, according to the data of our study, it was found that both in the main (in 74% of cases) and in the control (in 67%) groups, the majority of children were on artificial and natural feeding with a short period of time. These data are consistent with the results of previous studies, indicating that artificial feeding is one of the factors contributing to the emergence and manifestation of oxalate crystalluria [14]. Therefore, our data confirm that artificial feeding is a risk factor for the initiation of hyperoxaluria, but not oxalate nephropathy.In this regard, we studied nutritional disorders, including excessive use of certain food ingredients and the use of foods rich in oxalates, as an exogenous risk factor in the development of UHI, comparing the results in children of both groups. The comparison was carried out with medical standards for the food set for children (Recommended standards for food consumption in preschool educational institutions, SanPin No. 0348-17 - Hygienic requirements for the organization of high-grade and safe nutrition in preschool educational institutions of the Republic of Uzbekistan). The following set of products was taken into account: meat and fish, milk and milk products, bakery products, vegetables and fruits and their juices, sugar, fat.Analysis of the nature of food showed (see Table 4) that children aged 1-3 years in the main group consumed 105.3 g of bread products, 35.7 g. cereals and pasta, which corresponded to the normative indicators. Established an increased consumption of sugar - 65.2 grams. at a rate of 50 gr., fruit juices 170 gr. at a rate of 150 gr., potatoes 135 gr at a rate of 120 gr., cocoa products-2 gr. at a rate of 1 gr., confectionery 65 gr. at a rate of 55 gr., fat-65 gr. at a rate of 55 grams. There was an insufficient consumption of such food products as milk and dairy products 250 grams at a rate of 400 grams. Meat, poultry - 45 grams. at a rate of 120 gr, cottage cheese-30 gr. at a rate of 50 g .. Children aged 1-3 years in the main group did not eat fish in the diet.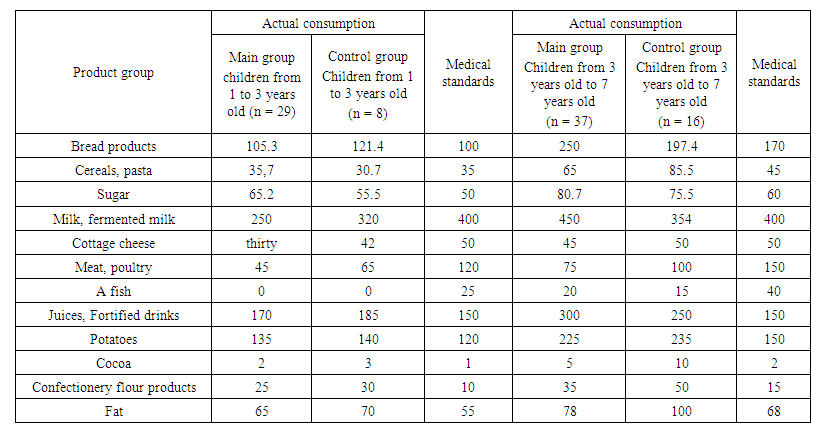 | Table 4. Comparative characteristics of food consumption of children in study groups (g / day) depending on age |
In children in the main group aged 3-7 years, there was an increased consumption of bakery products - 250 g at the norm of 170 g, cereals and pasta 65 g at the norm of 45 g, sugar 80.7 g at the norm of 60 g, cocoa 5 g at the norm 2 gr, potatoes-225 gr at a rate of 150 gr, fruit juices and fortified drinks 300 gr at a rate of 150 gr., Confectionery 35 gr at a rate of 15 gr, fat 78 gr at a rate of 68 gr. Insufficient consumption of meat products was noted - 75 g at the norm of 150 g, fish - 20 g at the norm of 40 g.In the control group at the age of 1-3 years and 3-7 years, an increased consumption of bakery products, sugar, fruit juices, confectionery, potatoes, cocoa, confectionery and fats was also noted.From the presented results it can be seen that in the diet of children in both study groups, regardless of age, a general pattern can be traced: the lack of meat products, dairy products. But in children aged 3 to 7 years in both groups, an excessive consumption of fruits (in most cases in the form of boxed fruit juices), baked goods, pasta, sugar, fat, cocoa, and potatoes (mainly due to fried) was found. Further analysis of the data showed that children aged 3 to 7 years in both study groups consumed juices more than normal. Recent Research Getting JE. et al. [6] prove that excessive consumption of fruit juices leads to the development of secondary oxalate nephropathy.
4. Conclusions
Analyzing the data, we came to the conclusion that a pronounced decrease in urine volume due to a decrease in the volume of fluid consumed leads to an increase in its concentration, as a result of which favorable conditions are created for the occurrence of COC. Artificial feeding is one of the risk factors for the initiation of COC, but not oxalate nephropathy. It was found that a violation of the nature of nutrition in children contributes to the formation of COC and SON.
References
| [1] | Dlin V. V. Dysmetabolic nephropathy with calcium oxalate crystalluria / V. V. Dlin, I. M. Osmanov // Effective pharmacotherapy. - 2013. - No. 42. - P. 8-16. [Google. Scholar] |
| [2] | The role of renal infection in the formation and progression of tubulointerstitial kidney damage in children / I.V. Zorin [et al.] // Attending Physician. - 2017. - No. 9. - P. 9–12. [lvrach.ru] |
| [3] | The effectiveness of enterosgel in the complex treatment of ecologically determined kidney diseases in children / MV Kudin [et al.] // Russian Bulletin of Perinatology and Pediatrics. - 2013. - No. 4. - P. 72–76. [cyberleninka.ru] |
| [4] | Yurieva E.A., Dlin V.V., Kudin M.V., Novikova N.N., Vozdvizhenskaya E.S., Kharabadze M.N., Knyazeva D.L. Metabolic nephropathy in children: causes of development, clinical and laboratory manifestations. Russian Bulletin of Perinatology and Pediatrics. 2016; 61 (2): 28-34. [Perinatologiya] |
| [5] | Dharmaratne, R.W. Fluoride in drinking water and diet: the causative factor of chronic kidney diseases in the North Central Province of Sri Lanka / R.W. Dharmaratne // Environ Health Prev Med. 2015. – V. 20. – P. 237–242. [PubMed] |
| [6] | Getting JE, Gregoire JR, Phul A, Kasten MJ. Oxalate nephropathy due to ‘juicing’: case report and review. Am J Med. 2013; 126: 768–772. [PubMed] |
| [7] | Lande, M. B. Role of urinary supersaturation in the evalution of children with urolithiasis / М. В. Lande, W. Varade // Pediatr Nephrol. – 2005. – V. 20. – № 4. – P. 491–494. [PubMed] |
| [8] | Miller LA, Stapleton FB. Urinary volume in children with urolithiasis. J Urol. 1989; 141:918-920. [PubMed] |
| [9] | Patology of the urinary system in the children's population of the Kharkiv region: incidence and some risk factors / G. R. Muratov [et al.] // Ukrainian Journal of Nephrology and DIALIS. – 2015. – № 3. – P. 21–26. [ukrjnd] |
| [10] | Rango, T. Nephrotoxic contaminants in drinking water and urine, and chronic kidney disease in rural Sri Lanka / T. Rango, M. Jeuland, H. Manthrithilake // Sci Total Environ. – 2015. – V. 518. – Р.574–585. [PubMed] |
| [11] | Van’t Hoff WG. Aetiological factors in pediatric urolithiasis. Nephron Clin Pract 2004; 98:c45-c48. [PubMed] |
| [12] | Wasana, H.M.S. Drinking water quality and chronic renal disease of unknown etiology (CKDu): synergistic effects of fluoride, cadmium and water hardness / H.M.S. Wasana, D. Aluthpatabendi, W.M.T.D. Kularatne // Environ Geochem Health. – 2016. – V.38. – P. 157–168. [PubMed] |
| [13] | Selman R. Calcium oxalate stone disease: role of lipid peroxidation and antioxidants.//Urol Res. - 2002 - Vol.30. - N. 1. - P.35-47. [link.springer] |
| [14] | Норре В., Hesse A., Neuhaus Т., Fanconi S. et al. Influence of nutrition on urinary oxalate and calcium in preterm and term infants.// Pediatric Nephrology. - 1997. - Vol.ll. - N.6. - P.687-690. [PubMed] |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML