-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2020; 10(9): 702-704
doi:10.5923/j.ajmms.20201009.15
Received: July 19, 2020; Accepted: August 18, 2020; Published: August 29, 2020

The Importance of Endovideosurgery Technologies in the Treatment and Diagnosis of Large Hernias in Children
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLBerdiev Ergash Abdullaevich1, Jumaev Mamoziyo Yusupovich2, Davlatov Utkir Xamdamovich2
1Termez Branch of Tashkent Medical Academy Research and Innovation Deputy Director, Surkhandarya, Uzbekistan
2Candidate of Medical Sciences, Surkhandarya, Uzbekistan
Correspondence to: Berdiev Ergash Abdullaevich, Termez Branch of Tashkent Medical Academy Research and Innovation Deputy Director, Surkhandarya, Uzbekistan.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This article presents treatment and diagnostic analyzes of 12 pediatric patients with large hernias torsion, which is very rare in children’s abdominal cavity. Of these, 8 had primary hernias torsion and 4 had secondary hernias torsion. Twelve patients underwent endovideolaparoscopic hernias resection, and one of them underwent additional appendectomy. Videolaparoscopic resection was performed in 1 patient with large hernias cyst. A patient with abdominal trauma underwent an upper middle laparotomy and underwent conversion. There were no complications at the time of surgery or in the postoperative period. Histological examination revealed signs of gangrenous omentitis in a large herd. Surgery using endovideolaparoscopic technologies allows to accurately diagnose the disease, to achieve simultaneous resection of hernias, to determine the etiological factors of secondary hernias torsion.
Keywords: Hernias torsion in children, Primary torsion, Secondary torsion, Surgical treatment, Laparoscopy
Cite this paper: Berdiev Ergash Abdullaevich, Jumaev Mamoziyo Yusupovich, Davlatov Utkir Xamdamovich, The Importance of Endovideosurgery Technologies in the Treatment and Diagnosis of Large Hernias in Children, American Journal of Medicine and Medical Sciences, Vol. 10 No. 9, 2020, pp. 702-704. doi: 10.5923/j.ajmms.20201009.15.
1. Introduction
- The urgency of the problem: Torsion of the large cartilage is a rare polyetiological disease in surgical practice, with acute abdominal symptoms in children. This pathology accounts for 0.01-0.32% of patients undergoing emergency abdominal surgery [1,4,7]. The etiological factors of torsion of large hernias have not been fully elucidated. The causative factors of this disease are abdominal adhesions, anterior abdominal hernias, obesity, chronic inflammatory processes in the abdomen, while the production factors are physical stress, abnormalities. p feeding can cause a sudden increase in abdominal pressure or contraction of the anterior abdominal wall muscles. [3,9,11]. Purpose: To analyze the sick children we are under clinical observation, as tetanus is a rare polyetiological disease in surgical practice.
2. Materials and Methods
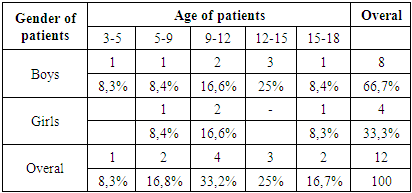
- From 2011 to 2019, 12 patients were treated for pediatric surgery in the pediatric surgery department of the Surkhandarya Regional Children's Multidisciplinary Medical Center. Patients were found to be 3 to 18 years of age. Of these, 8 (66.6%) were boys and 4 (33.4%) were girls. Based on these analyzes, it can be said that the disease is more prevalent in boys. All sick children admitted were admitted to the hospital with "acute appendicitis?" The suspect was hospitalized for examination and treatment.
|
3. Results
- For endovideolaparoscopic surgery, an 8 mm optical trocar was placed over the umbilical region and a 5 mm trocar was placed over the umbilicus and left flank. Endovideolaparoscopic surgery often reveals small amounts of serous-hemorrhagic fluid in the small pelvic cavity. 720° torsion of the large Hernias was detected in 10 patients during videoendolaparoscopic surgery. A 180° rotation of the large hernias was observed in one patient with a thin-walled cyst up to 7 cm in diameter. One patient was diagnosed with acute phlegmonous appendicitis with 360° twisting of the large cartilage. Twisted parts of the curvature are found in the lower abdomen or in the right flank, with longitudinal dimensions ranging from 3 cm to 7 cm in dark red or black, and the necrotic curve is clearly separated from the healthy curve.
4. Discussion
- Monopolar coagulation was used for endovideolaparoscopic resection of the large Hernias torsion, or Reder’s choke was performed in 12 sick children, and 1 of them underwent additional appendectomy at the time of surgery. Videoendolaparoscopic resection of a large Hernias cyst was performed in 1 patient. The resected drug was removed from the abdomen by inserting a large trocar instead of a 5 mm trocar placed in the umbilical region. Only one patient with abdominal trauma underwent conversion due to total infiltration of the large cartilage, and the surgery was performed using the upper middle laparotomy. No complications were observed during the postoperative and postoperative periods. Inpatient treatment ranged from 5 to 15 days, with an average bed rest of 7 days. Histological examination revealed signs of gangrenous omentitis in most cases due to circulatory disorders in the animal. The first information about the twisting of a large hernias was written by Oberst in 1882. There are primary and secondary types of Hernias twisting. Primary Hernias torsion is more common in boys Primary Hernias torsion is more common in children aged 11-15 years. Secondary hernias torsion, hernias cyst, hernias tumor, and herniasgematoma have been reported. One of the main causes of hernias twisting in children is its anatomical structure. Another factor is that children become obese as a result of obesity. The diagnosis of hernias torsion is very complicated, and in many cases the diagnosis is made at the time of surgery. In the diagnosis of hernias torsion in children it is necessary to make a comparative diagnosis with acute appendicitis, in girls with pathological diseases of the small pelvic cavity. In patients with large hernias torsion pain in the abdomen begins very sharply, pain in the abdomen In the first half, it is manifested by symptoms such as nausea, vomiting, dizziness. Sometimes the pain is caused by overeating and increased abdominal pressure. Clinical signs appear slowly, with no signs of long-term intoxication. On palpation of the abdomen there is a slight pain in the right half of the abdomen, and in most cases patients present 2-4 days after the onset of the disease. On palpation of the abdomen there is pain in the right half of the abdomen, muscle tension is not observed. Patients have normal or subfebrile body temperature. General blood tests show no changes at the onset of the disease, hernias necrosis, leukocytosis with peritonitis. Ultrasound examination of the abdomen can sometimes reveal circulatory disorders, edema, hyperechoicity of adipose tissue. In such cases, abdominal video laparoscopy plays an important role. In the literature, inadequate conservative treatment of hernias torsion in patients leads to the development of peritoneal adhesions as a result of the development of abscesses in the abdominal cavity. Therefore, the optimal method of treatment of Hernias torsion is surgery. One of the methods of diagnosis and treatment of Hernias torsion is laparoscopy. In 12 of the 13 children, hernias twisting was performed minimally invasively laparoscopically.
5. Conclusions
- 1. Major torsion in children is rare and its clinical signs are often similar to those of acute appendicitis.2. It is advisable to use endoscopic laparoscopy in the diagnosis of Hernias torsion, as there are no specific signs of large torsion in children, and UTT examination provides very little information.3. The rapid use of endoscopic laparoscopy in clinical practice in recent years has made it possible to diagnose large hernias in children in a timely manner.4. Endoscopic laparoscopy is one of the high-tech low-injury surgical procedures performed not only in the diagnosis of large herniated discs in children, but also in the destruction of etiologic factors by performing destructive altered herniation resection.