-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2020; 10(9): 660-663
doi:10.5923/j.ajmms.20201009.07
Received: June 28, 2020; Accepted: August 2, 2020; Published: August 26, 2020

Pathologically Undifferentiated Placental Morphology in Primary Placental Insufficiency
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLR. I. Israilov1, B. A. Sanoev2, A. Z. Olimova2
1Republican Center for Pathological Anatomy, Uzbekistan
2Bukhara State Medical Institute Named after Abu Ali Ibn Sina Ministry of Health of Uzbekistan
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This article describes the forms of pathologically undifferentiated placenta, which are the main morphological feature of primary placental insufficiency, and the specific morphological features of each. It was observed that hypoplasia, dysplasia, pathological formation of the structural units of the placenta, manifested by disorders of the structure, location, attachment of the placenta to the uterus, anomalies and vascularization of cateledons and mammary glands. The following forms were distinguished: 1) the type of survival of embryonic villis, 2) the appearance of incompletely intermediate-shaped villis, 3) sclerosed and chaotically located villis, 4) mixed, ie dissociated appearance.
Keywords: Pregnancy, Placenta, Deficiency, Incomplete stratification, Vascularization
Cite this paper: R. I. Israilov, B. A. Sanoev, A. Z. Olimova, Pathologically Undifferentiated Placental Morphology in Primary Placental Insufficiency, American Journal of Medicine and Medical Sciences, Vol. 10 No. 9, 2020, pp. 660-663. doi: 10.5923/j.ajmms.20201009.07.
Article Outline
1. Introduction
- Pathologically undifferentiated placenta is one of the main manifestations of primary placental insufficiency. Its causes are: genetic, endocrine, infections, and lack of enzymes in decidual tissue, hypoplasia, dysplasia, pathological formation of placental structural units as a result of pathogenic and morphogenesis effects on the zygote, blastocyst and developing placenta [1,2,3,4]. Primary morphological changes are manifested by disruption of the structure, location, attachment of the placenta to the uterus, anomalies of the coteledonand villis, and vascularization. As a result, the fetus also develops anomalies, birth defects, and is clinically manifested by the risk of miscarriage and premature birth [5,6,7,8,9,10].The main goal of the work was to clarify the specific morphological changes of pathologically undifferentiated placental forms.
2. Materials and Methods
- To achieve the goal, the placental tissue of 34 postpartum women with a history of primary placental insufficiency was morphologically studied. Hematoxylin and eosin stains of general morphology, as well as semi-thin incisions were stained with toluidine blue. For general morphology, 3 pieces from each placental, ie 1.5x1.5 cm from the center, middle and periphery, were cut and solidified in 10% neutralized formalin. After washing in running water for 2–4 h, it was dehydrated in concentrated alcohols and chloroform, then paraffin was poured and paraffin blocks were prepared. Incisions of 5–8 μm were made from paraffin blocks and stained with hematoxylin and eosin. To obtain semi-thin incisions, the placental fragments were solidified in osmium 4 oxide, dehydrated, epon wax was poured, and bricks were prepared. Semi-thin incisions 1 μm thick were taken from the Epon bricks on a Leica ultramicrotomy and stained with toluidine blue. Histological preparations were studied under 10, 20, 40, 100 lenses of a light microscope, and the required areas were photographed.
3. Inspection Results and Discussion
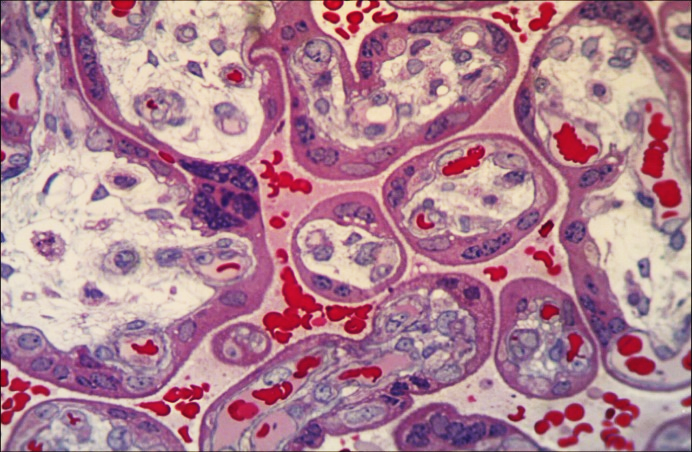
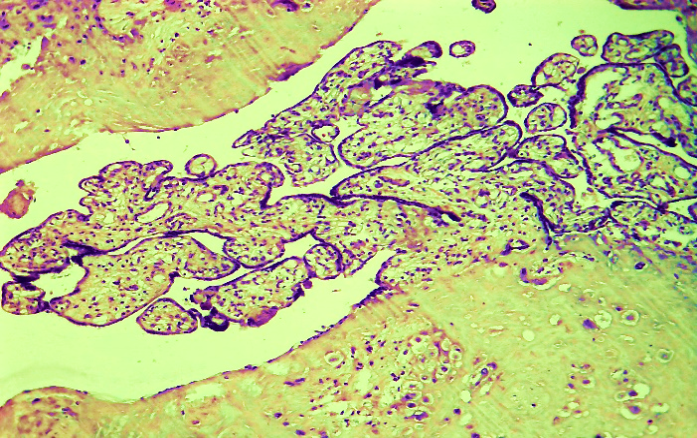
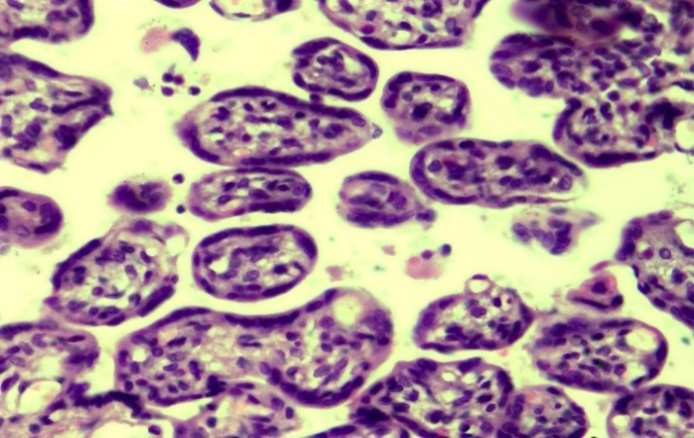
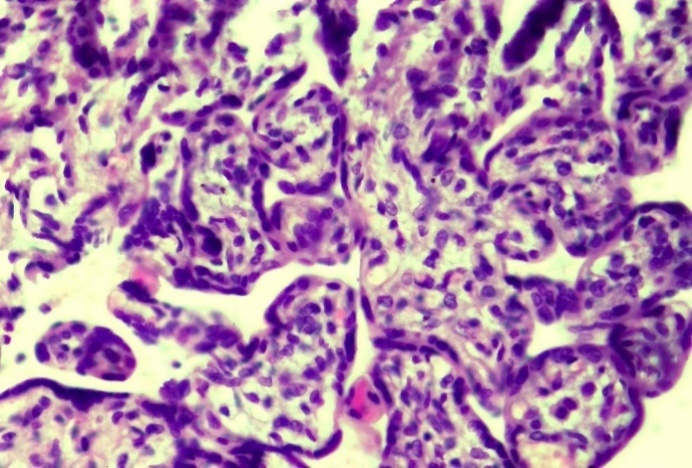
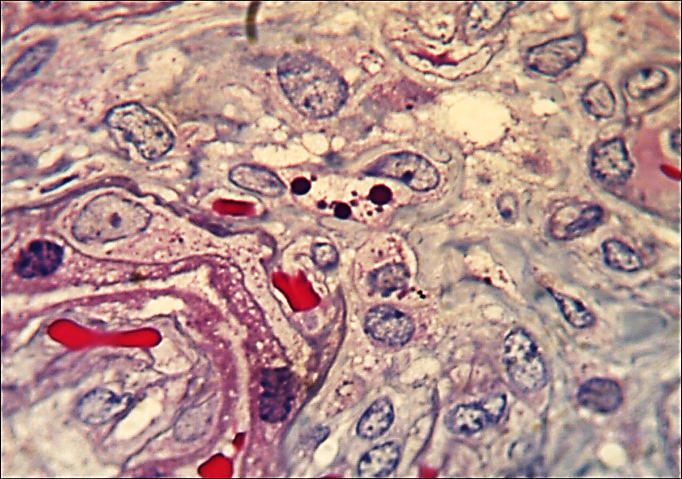
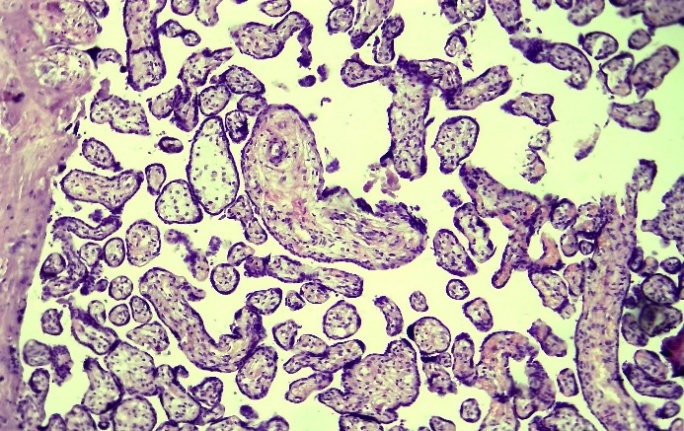
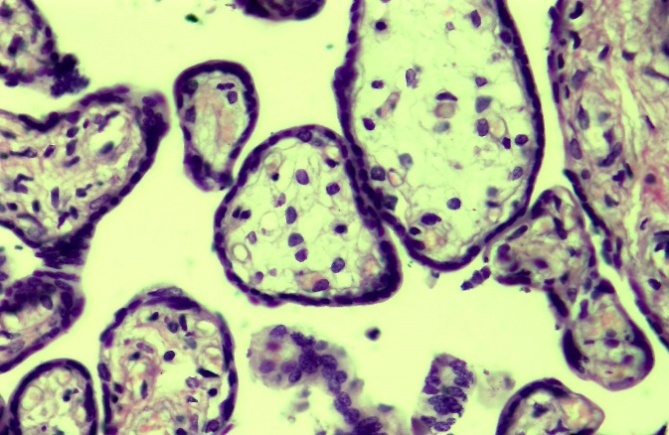
- The results of morphological examination showed that the pathologically undifferentiated placenta developed morphologically in several forms: 1) the type of embryonic villis survival, 2) the appearance of incomplete intermediate-shaped villis, 3) sclerosed and chaotically located villis, 4) mixed component, that is, dissociated. The type of embryonic villi survival develops as a result of cessation of placental maturation in the early stages of embryogenesis. In this type of pathologically undifferentiated placenta, morphologically there are structures in the placenta, even in the base villis, that are not fully developed, reminiscent of embryonic tissue. In this case, the base villis are relatively thin, the blood vessels are wide, the connective tissue stroma around them is undeveloped, that is, there are many blast cells, a small number of fibrous structures. The layers of the vascular wall are not uniformly developed, the endothelium consists of flat cells, the basement membrane is thin, the smooth muscle cell layer is found to be of uneven thickness. The number of secondary villis separated from them is small and undeveloped, less branched, the number of terminal villis is also small, and their size is small compared to the norm.It is observed that the terminal villis contain undifferentiated villis at the embryonic level, which are located close to each other. The stroma of such villis is found to consist of thin, immature, poorly developed connective tissue structures. The blood vessels are of various sizes, mostly located in the middle of the villies, with no hematotrophoblast barriers. The connective tissue stroma also has a chaotic structure, in which young cells are observed to be concentrated in one place and sparse in other places. The trophoblasts on the surface of the villis are also not well developed, that is, they are prismatic in some areas, flattened in other areas, and the nuclei are found to have varying degrees of hyperchromasis. A study of embryonic looking villi under a large magnification of the microscope shows that some of them are large, while others are relatively small, and the stroma consists of a mesenchymal type of non-embryonic connective tissue (Fig. 1). Among the cells in it, the Kashchenko-Gofbauer cells are the most numerous. There are almost no capillaries in the stroma, and all of them are composed of endothelial cells of different sizes, without walls. The trophoblasts on the surface of this type of villi are also composed of immature embryonic cells, i.e., their nuclei are of different sizes, hyperchromics, and different shapes.In addition to the above-mentioned data, the presence of even more profound changes was confirmed when the tissue of the pathologically undifferentiated placenta was examined in a semi-thin section of embryonic mammalian survival appearance. At a glance, it is observed that one of the villis is not similar to the other, that is, it differs in size and composition. Their immaturity at the embryonic level is mainly determined by the composition and structure of the stroma. It was established that the stroma of the connective tissue consists of mesenchymal tissue, that is, the cells are composed of polyblasts, histioblasts and fibroblasts, among which preserved endocrine cells, Kashchenko-Hoffbauer cells were found in large numbers and that they are mainly located around blood vessels (Fig. 2). A characteristic feature of this type of embryonic structure of the mammary stroma is the preservation of these endocrine cells and the large number of Kashchenko-Gofbauer cells. In addition, the fact that the villi on the surface are trophoblast-free blast cells, that is, their cytoplasm is wider than normal, has a lot of chromatin in the nuclei, different sizes, and location disorder also confirms the embryonic structure. It was found that the appearance of incomplete intermediate-shaped villis of the pathologically undifferentiated placenta differs morphologically from the above-mentioned form. One of the main morphological features of this was confirmed by the low separation of rod villis from this chorial membrane and their similarity in development to secondary villis. This type of villi confirms that several of them at once separated from one place in the chorial membrane and joined together, which means that the coteledons developed without an anomaly (Fig. 3). The stroma of this type of villi was found to be thin, poorly developed, and swollen. It was found that the fibrous structures in the stroma are disorganized, the cells are sparse and mostly composed of undifferentiated young blast cells. The number of capillaries in the stroma is also small, all of them are located in the central part of the stroma, the diameter is different, the wall is not fully developed. From the base villis of this type, the branching of the secondary and terminal villis is low, the terminal villis are very small, and the size is small compared to the norm. Most of them are underdeveloped round, the trophoblasts on the surface are flat and prismatic. The number of capillaries in the stroma is small, located in the center, hematotrophoblast barriers are not formed. In this type of pathologically undifferentiated placenta, terminal villis are found to be smaller and less complete than normal. Evidence of the immaturity of such villis is their small size, lack of stroma and capillaries in it (Fig. 4), immaturity of the cells in them, and the presence of Kashchenko-Gofbauer cells. Covering trophoblast cells are also observed to be mostly single-layered but chaotic.The appearance of the next, i.e., sclerosed, chaotically located villis of the pathologically undifferentiated placenta develops in the 2nd trimester of pregnancy and differs from other types by specific morphological changes. The morphological peculiarity of this form is the smallness of the villis, the sclerosis of the stroma, the lack of capillaries in it, the almost absence of syncytiotrophoblast buds (Fig. 5), the lack of immature villis. As can be seen in this micro-image, the dimensions of the secondary and terminal villis of the placenta are less than normal, close to each other, and densely packed, all with a proliferation of cell-rich connective tissue in the stroma. The sclerosed stroma contains almost no capillaries, and the veins are very small, narrowed, and spasmodic in appearance. The trophoblasts on the outer surface of the villis are dense, prismatic in shape, the nuclei of some are hyperchromic and elongated, among them there are sparse syncytiotrophoblast buds, all of which are very small, flattened. When seen in a large lens of a microscope in semi-thin sections, the morphological features shown above are even more clearly visible. The stroma of the villis is dense due to sclerosis, there are many fibrous structures and dense, almost no capillaries, the existing capillaries in some villis are round, the cells of the wall are connected with the connective tissue structure (Fig. 6). The trophoblasts on the surface are flattened, and their nuclei are also elongated, rich in chromatin.The fourth appearance of the pathologically undifferentiated placenta, i.e., a mixed dissociated appearance of the component, is a relatively common form that develops in the 2nd and 3rd trimesters of pregnancy. In our material, it was confirmed that he suffered mainly from severe preeclampsia and diabetes. Morphologically specific changes were identified as the chaotic development of coteledons, the presence of immature villis among mature villis, and the presence of single-embryonic and hypovascular villis among them (Fig. 7). In addition to these changes, decidual tissue and placental trophoblasts are characterized by severe dystrophy, excessive bleeding into the interstitial space of the placenta, the presence of white and hemorrhagic infarction foci in the placenta. Immature villis are found to be mainly round and oval in shape, their stroma consists of thin low-fiber connective tissue, and the interstitial material is strongly swollen (Fig. 8). Capillaries are almost non-existent, and their presence is confirmed in the case of very small atresia, which does not form a hematotrophoblastic barrier. The surface trophoblasts are mainly composed of a single row of prismatic epithelium, the nuclei of which are flattened and hyperchromic.
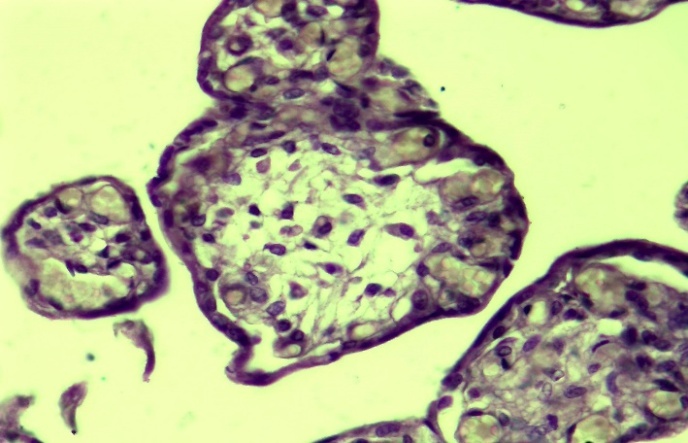 | Figure 1. The structure of immature villis. Paint: G-E. X: 10x40 |
 | Figure 2. Appearance of immature villis in a semi-thin section. Dye: methylene blue. X: 10x100 |
 | Figure 3. Unsupported base villis. Paint: G-E. X: 10x10 |
 | Figure 4. Capillaries are less tiny villis. Paint: G-E. X: 10x40 |
 | Figure 5. Sclerosed villis. Paint: G-E. X: 10x40 |
 | Figure 6. Appearance of sclerosed villis in a semi-thin section. Dye: methylene blue. X: 10x100 |
 | Figure 7. Mixed villis. Paint: G-E. X: 10x10 |
 | Figure 8. Untreated villis. Paint: G-E. X: 10x40 |
4. Conclusions
- Pathologically undifferentiated placenta is one of the main manifestations of primary placental insufficiency, manifested by hypoplasia, dysplasia, pathological formation of placental structural units, disorders of placental structure, location, uterine adhesions, coteledons placental anomalies and vascularization.It was confirmed that the pathological placenta developed morphologically in several forms: 1) the type of survival of embryonic villis, 2) the appearance of incomplete intermediate-shaped villis, 3) sclerosed and chaotically located villis, 4) mixed, ie dissociated appearances.The type of embryonic villis preserved morphologically placental villis, even the base villis are not fully developed, the presence of structures reminiscent of embryonic tissue, the base villis are relatively thin, the blood vessels are wide, the surrounding connective tissue stroma is not visible, ie blast cells are numerous, fibrous structures are small.One of the main morphological features of the incomplete intermediate form of the placenta is the low separation of the villi from the chorial membrane, their stroma is thin, underdeveloped, swollen, disordered fibrous structures, sparse and mostly immature young blast cells, the number of capillaries rarely, the lesions are located in the central part of the stroma, of different diameters, the wall is not fully developed.The appearance of sclerosed and chaotically located villis is morphologically specific, the villis are small, the stroma is sclerotic, there is a lack of capillaries, almost no syncytiotrophoblast buds, there is a lack of immature villis.The dissociated appearance of the mixed composition was relatively common, and morphologically specific changes were identified as the chaotic development of coteledons, the presence of immature villis among mature villis, and single-embryonic and hypovascular villis among them.