Tulyaganov J. Sh. , Akbarov A. N. , Safarov M. T. , Arslanov O. U. , Ziyadullaeva N. S. , Kudratov Sh. Sh.
Tashkent State Dental Institute, Uzbekistan
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Tissue engineering - the creation of new tissues and organs to repair a damaged organ by delivering to the desired area the supporting structures of cells, molecular and mechanical signals for regeneration. The goal of tissue engineering is to restore biological (metabolic) functions, namely: tissue regeneration, as well as morphological and functional integrity, in contrast to the simple mechanical replacement of its osteoplastic material. For this purpose, it is advisable to use bioactive glass bioactive glass from bioactive osteoplastic material. Osteoplastic material in combination with platelet rich plasma (PR P) or hyaluronic acid to prevent inflammation and bone atrophy while optimizing the strength of the bone repair process.
Keywords:
Biotechnology, Tissue engineering, Regeneration, Implantology, Gialuronic acid, Ultrasound osteometry, Bioglass
Cite this paper: Tulyaganov J. Sh. , Akbarov A. N. , Safarov M. T. , Arslanov O. U. , Ziyadullaeva N. S. , Kudratov Sh. Sh. , Tissue Engineering by Guided Bone Regeneration with Application of Bioglass “Bioactive Glass” in Patients with Diabetes for Dental Implantation, American Journal of Medicine and Medical Sciences, Vol. 10 No. 9, 2020, pp. 646-651. doi: 10.5923/j.ajmms.20201009.04.
Article Outline
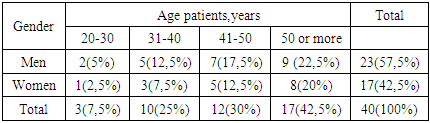
In modern medicine and biotechnology, tissue engineering occupies a special place (tissue engineering) - the creation of new tissues and organs for the reconstruction of the damaged organ by means of delivery to the desired region of the supporting structures of cells, molecular and mechanical signals for regeneration. Alloplastic inert materials can eliminate only physical and mechanical defects of damaged or atrophied tissues. The goal of tissue engineering is to restore the biological (metabolic) functions, ie: the regeneration of tissue, and the morphological and functional integrity, as opposed to simple mechanical replacement of its osteoplastic material. [2,3,4].For the first time in Sweden for more than 20 years of the development in the treatment of periodontitis are happening In modern medicine and biotechnology, tissue engineering occupies a special place (tissue engineering) - the creation of new tissues and organs for the reconstruction of the damaged organ by means of delivery to the desired region of the supporting structures of cells, molecular and mechanical signals for regeneration. Alloplastic inert materials can eliminate only physical and mechanical defects of damaged or atrophied tissues. The goal of tissue engineering is to restore the biological (metabolic) functions, ie: the regeneration of tissue, and the morphological and functional integrity, as opposed to simple mechanical replacement of its osteoplastic material. [1,3].The cell material for tissue engineering can be represented by regenerable cells or tissue stem cells. The types of molecular signals for regeneration in tissue engineering among biologically active substances of natural origin include macromolecule - hyaluronic acid, which is a scientific and practical interest in the field of dental implantology with bone grafting. As the polyanion, hyaluronic acid has a high water-holding capacity - one molecule of hyaluronic acid connects 200-300 water molecules. Together with other proteoglycans, hyaluronic acid is a member of the extracellular matrix. Due to its physical and chemical properties such as high viscosity (specific ability to bind water and protein to form proteoglycan aggregates) hyaluronic acid contributes to the manifestation of numerous connective tissue functions. [2,10].For the purpose from bioactive osteoplastic material reasonable use of bioglass “Bioactive Glass”. Osteoplastic material in aggregate with rich platelet rich plasma (PR P) or gialuronic acid to prevent inflammation and atrophy of the bone on the strength optimization conditions process of reparative in the bone.Bioactive glass “Bioactive glass” apply (to) group of surface-active bio material, on surface witch of descend row specific reactions, bring to formation amorphous calcium phosphate or crystalline hydroxyapatite, what favorable for formation bone [osseous] tissue. As well this material have ability to release critical concentration ion of Si, Ca, P and Na which one evoke bone formation/osteogenesis. Regenerate of bone [osseous] tissue it is allowed/ it can be done on unique granule of bioactive glass.Given that diabetic patients have low regenerative potential of bone tissue, which is associated with infringement of microcirculation (angiopathy), atherosclerosis, tissue hypoxia, and increased levels of lipid peroxidation. That leads to the urgency of this problem which lies in the optimization of reparative regeneration conditions, providing cellular material and macromolecules in dental implantation. It is particularly important in case of simultaneous recovery of jaw bone tissue. (AB Shabanovich, EV Aleynikov, 2008). [2,3,4].The ability of diabetic patients, in the surgery with bone augmentation and dental implantation, to differentiate osteogenic cells also depend on the preservation or restoration of blood vessels. In the case of poor circulation in the postsurgical field occurs oxygen deficiency, which in turn stimulates the proliferation of fibrous and chondroid tissue instead of bone mineralization process. [10,11].Maximum accuracy in diagnosing the state of the bone prior to implantation plays a vital role in choosing the optimal implant design and surgical intervention techniques. Most authentically the quality of the bone can be estimated based on the results of X-ray 3D COMPUTER tomography, ultrasound osteometry and the also by surgeon during surgical intervention and visual inspection. However, not always after receiving new information by using this ways, the surgeon is capable of changing the plan of operation. [2,5,6,10].Remote status of the newly formed bone structure around the dental implant determines the degree of osseointegration and design of prosthetics and rehabilitation period. [7,9,11]. The research work of Swedish scientist, the founder of modern implant Branemark, has proven true osseointegration of the implant in the bone tissue using an implant made of pure titanium. [8,9,11].During the intraosseous dental implantation there is also a probability development inflammatory complications associated with infection of incisional wound by oral microflora, especially bone. All operations related to the risk of oral or oral linked are classified as clean-contaminated and require prior and targeted use of antimicrobial drugs, due to the relatively high risk of microbial contamination (V.N.Tsarev P V.Ushakov 2004).Determination of features of microflora in the pathological focus can become a basis for new approaches to planning dental implant with bone grafting and monitoring the results in patients with inflammatory periodontal diseases as well as to the choice of prophylactic agents with selective antibacterial effect, including on the basis of virulent bacteriophages to periodontal.The aim of our research is to study the morphological and functional restructuring of the newly formed bone, osseointegration of dental implant and an objective evaluation of the results of tissue engineering with guided bone regeneration with dental implantation in patients with diabetes with apply osteoplasty material bioglass “Bioactive glass”.We examined 40 patients with diabetes between the ages of 20 and 65 with dentition defects and atrophy of the alveolar process of varying degrees, undergoing surgery dental implant with bone grafting in combination with hyaluronic acid (IMPLA, Germany) and platelet-rich plasma (PRP). From bioactive osteoplastic material used bioglass “Bioactive glass”.The patients and the test results of the clinical bone grafting drawn from the treatment setting in the clinic Surgical Dentistry of the Tashkent State Institute of Dental and from the dental clinic "Zahne na Claar" in Kassel (Germany) and from the Institute of Endocrinology, Ministry of Health of the Republic of Uzbekistan. The research work carried out at the Department of surgical dentistry and dental implantology and in the Department of Normal and Pathological Physiology, Microbiology, Pharmacology, of the Tashkent State Dental Institute in the 2015-2016 years. Table 1. The distribution of patients by age and sex, abs. (%)
 |
| |
|
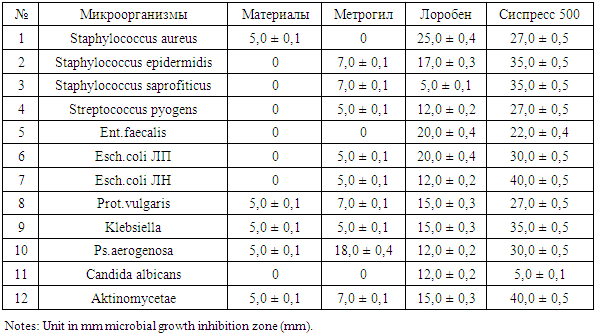
Microbiological examination included selection of microflora from saliva collected via oral rinses with sterile saline. Identification of isolated bacteria, using anaerobic culture techniques. Taking the material was performed eight times: before surgery before and after prescribing. The capture of the material after the operation was carried out in the early stages after 3, 7, 14, 30 days after the dental implantation.It is known, that an infectious-inflammatory processes significantly increases the probability of graft rejection. By this, it is urgent to develop activities aimed at the prevention of these complications arising during this kind of intervention. In recent years, in the global dental practice, when performing dental implant, actively implemented methods of the preoperative prevention based on the use of highly effective antiseptics and antibiotics (VN Tsarev, RV Ushakov VI Chuvilin, 2000).However, for prescribing effective drugs of directed action (antibiotics) it is necessary to have clear evidence of a potential-aggressive microbial flora of the patient and its sensitivity to various antibiotics. Taking into account the above aspects, prior to the microbiological and immunological studies of oral fluid in patients with diabetes to whom recommended dental implantation, we assessed the effectiveness of the use of several drugs, such as: metrolin, metrogil, loroben, sispress 500, in order to preoperative preparation of patients, in conditions in vitro!The data obtained in these studies are shown in Table 2.Table 2. Sensitivity Characteristics of microbes to some drugs in the conditions in vitro!
 |
| |
|
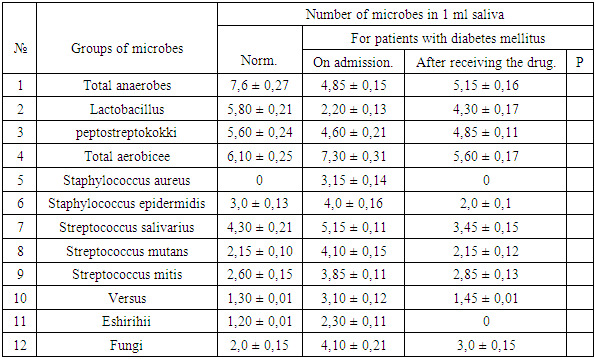
The table shows that the drug metrogil not has antibacterial properties, at the same time drug metrogil had a significant impact on the culture (Pseudomonas aerogenosa) which amounted to 18,0 ± 0,4 mm. Drug loroben has effects on almost all studied groups of microbes, except for culture Staphylococcus saprofiticus. Interestingly, this drug were moderately sensitive both gram-positive and gram-negative microbes including fungi. Among all tested drugs the strongest antibacterial effect had a sispress 500. As can be seen from the table, highly sensitive were eshirihii and actinomycetes, which equaled 40.0 ± 0.5 mm. and the remaining groups tested germs were also highly sensitive from 22,0 ± 0,4 to 35,0 ± 0.5 mm, and only fungi of the genus Candida seemed insensitive.Microbiological studies of quantitative parameters of microbes in the mouth of patients with diabetes mellitus after preparation pre operating using the above drugs are presented in Table 3.Table 3. Indicators of oral fluid flora in patients with diabetes mellitus lg (M ± m) cfu / ml
 |
| |
|
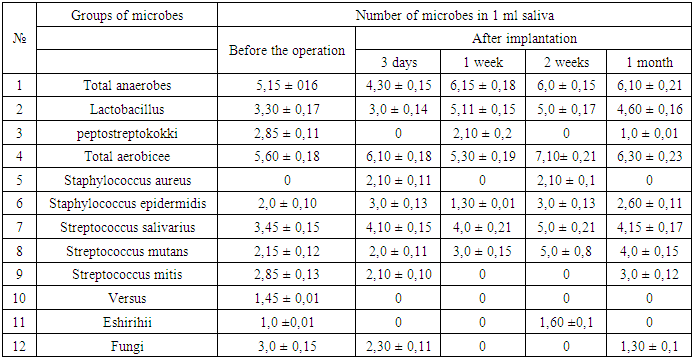
The table shows that all the studied groups of microbes have a positive quantitative shift is actually close to normal and only the number of Candida fungi several high data apparently used drugs do not have antifungal activity.The next group of our study consisted of patients with diabetes who underwent dental implantation. Microbiological examination of these patients after surgery performed in dynamics: 3-7-14-30 on days -that was the early period of observation, these same patients in the study continued and long-term periods of observation - is 3-6 months. Materials of microbiological studies carried out in the early stages of the observation are shown in Table 4.Table 4. Characteristics of oral flora in patients with diabetes, after dental implantation and bone grafting in the early stages. lg (M ± m) CFU / ml
 |
| |
|
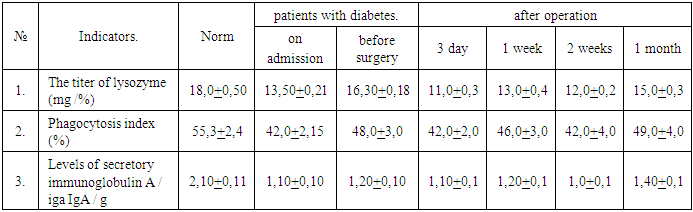
The table shows that on day 3 after surgery microbial picture is somewhat deteriorated in comparison with the picture pre operation. At the same time, these changes have a tendency anaerobic flora decreased slightly, but increased somewhat the facultative. It is particularly alarming, the emergence of oral strains of pathogenic staph (Staphylococcus aureus).Interestingly, in the observations on 7 the day microflora of the oral cavity differ mostly positive changes, so anaerobic flora even increased in comparison with the picture before the operation. Optional flora close to the norm, which is particularly pleasing, that one that some microbes such as pathogenic staphylococci, Streptococcus mitis, against Eshirihii and fungi in general i.e. eliminated the disappeared, and it is these microbes, mostly due to the large set of fragments pathogenicity, and are the cause of inflammation after surgery.On 14th day of the study can be noted that improvements available at 7 days, not only retained, but also further improved because anaerobic flora was slightly higher compared to pre operation. However, the alarming increase in the number of facultative flora, so the total number of the picture was lg 7,10 ± 0,21KOE / ml. Apparently the picture can be explained by the fact that on the 14th day ended compensatory adaptive processes in the oral cavity and the dose of drugs were found sufficient to suppress facultative flora.and observed the emergence of strains of pathogenic staphylococcus. However, the most interesting picture of the oral microflora we observed in the 30 day study, the actual quantitative parameters flora in anaerobic as well, and an optional very close to the normal range, and is particularly pleased with the elimination of such of microbes as pathogenic staphylococci, Proteus and eshirihii. We would like to emphasize that these positive developments occurring in the microflora of the oral cavity in patients with diabetes who underwent dental implants and bone grafting correlate with the picture of the clinical course of these patients. In table №2 figures, at patient’s admission, Staf Aureus in liquid oral flora is present in significant amounts. After receiving the drug prior to surgery, he is eliminated. Further Strep. Mutans fungi, at admission of patient, exceeds the norm by 2 times. Then, after taking the drug figures are normalized.In Table №3 on the 3rd day after the operation the number of Staf. aureus risen again. By the 1st week after surgery it normalizes. By the 2nd week indicator Staf. aureus grows.This is because the medication after the operation is completed at the expiration of 1 week after implantation. The same trend is observed in Strep. mutans. A figure Strep. Salivarius to 2nd week increased slightly, and the first month is normalized.In the table 5, at admission, indicator of the titer of lysozyme reduced.Table 5. Indicators of local oral defense factors in patients with diabetes, after dental implantation, in the early stages
 |
| |
|
Before the operation, after taking the medicines it is close to normal. Further to third day after surgery, the level of its amount reduced due to traumatic shock. In subsequent periods, his figure is closer to the norm.The morphological and functional evaluation of bone tissue reconstruction after guided bone regeneration with the use of hyaluronic acid, we carried out a dynamic study of the structure of the bone tissue before and after dental implantation. Bone density was assessed by Haunsfield scale units - HU on the results of the 3D X-ray multispriral computed tomography «Sirona - Galileos» (Germany), «VOLUX- Triana» (South Korea), «MORITA» (Japan), Philips (Germany), radiovisiography (the unit "AnyRay-ANR2-0210", the sensor "EzSensor-CR1, 5D-09-0020", VatechE-WOOTehnology, South Korea).The program allows you to map gray values on the CT scan linearity of gray on the monitor, which objectively assesses the structure and bone density.We obtained data the average bone density units scale Haunsfield - HU comparatively evaluated the results obtained Misch classification of bone type.1) 1150 and more Haunsfield scale units - HU, consistent with Misch classification type D1 bone (dense homogenous compact bone substance, a little spongy tissue);2) 840-1150 Haunsfield scale units - HU consistent with the classification Misch bone type D2 (dense homogenous compact bone substance, spongy tissue coarse-grained, with a distinct trabecular structure);3) 330-840 Haunsfield scale units - HU consistent with the classification D3 Misch type of bone (a thin layer of cortical bone, close-meshed cancellous bone with a distinct trabecular structure);4) 145-330 Haunsfield scale units - HU consistent with the classification Misch bone type D4 (very thin layer of cortical bone, cancellous bone loose);The data allow us to determine the morphological and functional restructuring during the dental implant with bone grafting and dental implants functioning in patients with diabetes.At the results of the studies defined a proportional change in bone density depending on the time of implantation and functional loading of the implant. Studies show that one year after guided bone regeneration of bone tissue growth is up 95%.To determine the primary stability of the implant and the analysis of remote results of intraosseous dental implant osseointegration used instrument «Osstell ISQ» the production of the company Integration Diagnostics (Sweden) tuned to a resonant frequency analysis of the RFA (Resonance Frequency Analysis) determines the rate of implant stability. All patients during and after surgery was performed measurement ISQ (Implant stability Quotient) / ISQ (implant stability factor) in certain periods. During the operation, before closing the wound and in terms 1-2-4-6-9-12-24 months.  | a) a device for measuring ISQ / CSI b) attach magnetized parts in the implant), b) and measuring the mesiodistal direction vestibulooralnom |
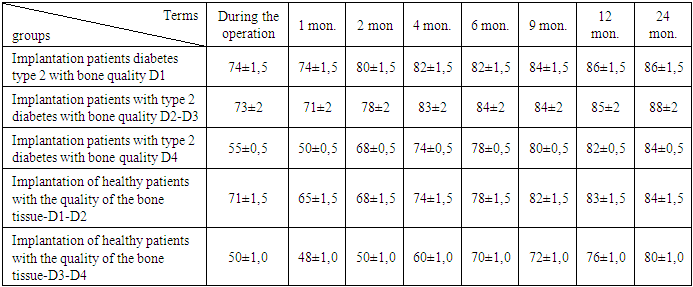
Table 6. Average values ISQ (implant stability factor), ISQ - (implant stability quotient)
 |
| |
|
Integration of bone components, due to the formation of mineralized areas of direct contact with the bony structures of the implant surface. The integration of the implant with bone structure more pronounced than in previous terms in all comparative groups.The best indicator of ISQ / CSI for the secure functional load is higher than 70 units. In assessing osseointegration of implants precision measurement stability, in instrument indication «Osstell» (Sweden) sufficiently rigidly attached components installed repeatability with high accuracy. An objective method for primary stability studies and distant osseointegration of dental intraosseous screw implants to evaluate the primary stabilization of the implant.Conclusions1. The data on assessment of the bone structure indicate the rationality and objectivity of research methods to facilitate a correct assessment of the state of the bone tissue before implantation and the choice of method of implantation and osteoplasty.2. In use of osteoplastic material bioglass “bioactive glass” in aggregate with PRP or gialuronic acid to prevent inflammation and atrophy of the bone under optimization conditions of reparative process in the bone.3. The use of hyaluronic acid activates inhibitors or retarders metalloprotienaz and thus effectively prevents the destruction of tissues. A similar effect is achieved by slowing the cytokines that cause inflammation (eg TNF α). Thus, hyaluronic acid may help preserve tissues.4. This microbiological research suggests a positive impact sound application of antimicrobial and antiseptic agents on wound regeneration after dental implantation.5. Targeted use of antimicrobials help to reduce the concentration of microorganisms in periodontal surgical wound and reduces the number of inflammatory complications. Predict the possible inflammatory complications in the postoperative period in the species composition of microorganisms and to conduct timely medication.6. Dynamic observation of morphological and functional restructuring of the bone tissue can correctly determine the optimal time of prosthesis and prevents complications in patients with diabetes during dental implantation with bone augmentation, followed by a decrease in terms of rehabilitation.7. By the method of resonant frequency implant stability analysis and evaluation of the quality of bone Haunsfield scale units - HU can prevent complications associated unreasonable early loading of the implant.8. Using the device «Osstell ISQ» tuned to a resonant frequency analysis of the RFA (Resonance Frequency Analysis) to assess the primary stability of the implant rate and distant osseointegration, to prevent complications related to unreasonable early loading of the implant, and the choice of optimal period of prosthetics and reducing the time of prosthetic treatment.
References
| [1] | David A. Mitchell Anastasios N. Kanatas, 2015. An introduction to oral and maxillofacial surgery (Second edition). |
| [2] | Misch, Carl E, 2008. Contemporary Implant Dentistry. |
| [3] | Neelima Anil Malik, 2008. Textbook of Oral and Maxillofacial Surgery. |
| [4] | Peterson’s 2004. Principles of Oral and Maxillofacial Surgery. |
| [5] | Albrektsson T., Johansson C., Lundgren A.K., Sul Y.T., Gottlow J. (2000) Experimental studies on oxidized implants. A histomorphometrical and biomechanical analysis // Appl. Osseointegration Res. – 1: 21–24. |
| [6] | Albrektsson T. On long-term maintenance of the osseointegrated response // J. Aust. Prosthodont, 7 [Suppl.]. – 2003. – P. 15–24. |
| [7] | Albrektsson T. Principles of osseointegration. In: Hobkirk J.A., Watson K. (eds) Dental and maxillofacial implantology // Mosby-Wolfe, London. – 2001. – P. 9–19. |
| [8] | Albrektsson T. Principles of osseointegration. In: Hobkirk J.A., Watson К. Dental and maxillofacial implantology // Mosby-Wolfe, London, 2005. – P. 9–19. |
| [9] | Davies J.E. In vitro modeling of the bone/implant interface // Anat. Rec. – 1996; 245: 426–45. |
| [10] | Davies J.E. The cellular cascades of wound healing. In: Bone engineering. Toronto: em squared Inc., 2000: 81–93. |
| [11] | Gruber R., Varga F., Fischer M.B. et al. Platelets stimulate proliferation of bone cells: involvement of platelet-derived growth factor, microparticles and membranes // Clin. Oral Impl. Res. – 2002; 13: 529–35. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML