-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2020; 10(9): 643-645
doi:10.5923/j.ajmms.20201009.03
Received: July 6, 2020; Accepted: August 8, 2020; Published: August 15, 2020

Aspects of Microflora Disturbance in the Implant-gingival Sulcus in Patients Using Fixed Bridges with Support on Dental Implants
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSafarov M. T. , Tashpulatova K. M.
Tashkent State Dental Institute, Uzbekistan
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The main complications in prosthetics of patients using dental implants today are inflammatory processes in the near-implant zone. Analysis of specialized literature reliably indicates the microbial theory of the occurrence of inflammatory complications, known as peri-implantitis. The most common complication of dental implantation is perimplantitis, which develops in various forms (traumatic, resorptive, inflammatory, ulcerative) in the near-implant zone. Microbiological studies have shown that in patients with peri-implantitis, the biocenosis of the oral environment is significantly impaired. The results of clinical and microbiological studies of patients indicate that the degree of disturbances in the biocenosis of the oral cavity is interconnected with the clinical form of perimplantitis. Moreover, it was found that dysbiotic shifts aggravate the clinical picture of the disease.
Keywords: Pereimplantitis, Aerobs, Anaerobs, Microflora, Pneumococcs, Candida, Prevotella intermedia, Disbios
Cite this paper: Safarov M. T. , Tashpulatova K. M. , Aspects of Microflora Disturbance in the Implant-gingival Sulcus in Patients Using Fixed Bridges with Support on Dental Implants, American Journal of Medicine and Medical Sciences, Vol. 10 No. 9, 2020, pp. 643-645. doi: 10.5923/j.ajmms.20201009.03.
Article Outline
- It is well known that in a healthy periodontal condition the microflora of the periodontal fissure and grooves around the implant is almost the same (mainly gram-positive immobilized aerobic bacteria, usually cocci). The pathogenic microflora around the implant is similar to the pathogenic flora in periodontitis (gram-negative motile anaerobic microorganisms). The pathogenic bacteria associated with periodontitis (Prevotella intermedia and Porphyromonas gingivalis) are responsible for the damage to the tissues surrounding the implants. The formation of plaque on implants is identical to plaque on natural teeth and occurs at the same time. The change in the nature of microflora during reimplantitis and periodontitis occurs in a similar way with a shift from coccal forms to rod-shaped and spirochetes. In addition, there is a positive correlation between the increase in plaque and the degree of the inflammatory process, as well as between the increase in plaque and the depth of the pockets around the implant.Microbiological examination of patients using bridges with support on implants revealed a definite correlation of changes in the microflora of the oral cavity and reimplantitis. Thus, the microflora of the oral cavity in mild forms of reimplantitis included all taxonomic groups of microorganisms that are defined in healthy individuals. The frequency of their detection almost did not differ from the norm, minor changes were not of a natural nature (aerobic and anaerobic gram-positive and gram-negative microbes). Close results were also obtained by a quantitative study of the contents of the oral cavity, although in relation to certain groups of bacteria, a difference was revealed that manifested itself in a decrease in CFU / ml for Streptococcus salivarius (from 7.4 to 5.4), Peptococcus c (7, 0 to 5.5) and, conversely, increasing the concentration of fusobacteria from 2.8 to 5.7 and “odontogenic” bacteroids from 3 to 4.8 (p <0.05).With moderate severity of reimplantitis, the number of most species and groups that make up the normal flora of the oral cavity was reduced: green streptococci from 100.0 to 68.5% (p <0.01), staphylococci from 90.0 to 45.7% (p <0.01), diphtheroids from 55.0 to 5.7% (p <0.01), neysseries c90.0 to 37.1% (p <0.01). The number of pneumococci (25.0 to 14.3%), lactobacilli (from 90.0 to 68.5%) decreased less significantly (p> 0.05).With a slight decrease in the total number of bacteroids to 83.3%, their species composition noticeably changed: if Pr and Pr. Prevailed in healthy and in patients with mild CGP. melaninogenicus and other bacteroids, then, with moderate severity, the frequency of their release sharply decreased, and the number of odontogenic anaerobes increased from 10.0 to 83.3% (p <0.05). There was also an increase in the frequency of sowing fungi of the genus Candida from 25.0 to 50.0% (p> 0.05). Protozoa, like spirochetes, in native preparations were found in isolated cases (2.8% each). In patients with severe form of reimplantitis with inflammatory secretions, hemophils, pneumococci, and other cocci were absent; many times lower was the sowing rate of non-growing streptococci, staphylococci, diphtheroids, neysseries, and waillonell (p <0.05 and p <0.01). At the same time, the frequency of detection of Candida mushrooms (from 15 to 50.0%) and odontogenic bacteroids (from 10.0 to 83.3%) increased. The number of green streptococci was 2.3 times less than that of healthy ones, staphylococci - 4.3 times, neysserii - 3.6 times, lactobacilli - 2.6 times, vellonellus - 2 times. At the same time, the concentration of fusobacteria increased by 2 times, and actinomycetes by 3.2 times. The total number of bacteroids increased 1.6 times, of which odontogenic ones - 1.7 times. In 5 (16.6%) patients, the study revealed trichomonads, spirochetes and spirills (the latter - only 6.6%).When the depth of the implant-gingival sulcus is not more than 4 mm, in most cases there was a slightly lower frequency of sowing of the aerobic-microaerophilic flora than in healthy individuals (p> 0.05). No species such as pneumococci, diphtheroids were found. In the anaerobic part of the microflora, only mutut group of streptococci (90 and 64%, p <0.05) and peptostreptococci (95 and 60%, p <0.05) affected significant changes. The concentration of detected microorganisms also remained almost unchanged, although CFU / ml of peptostreptococcus in patients of this group decreased from 6.2 normal to 4.4. The change in the spectrum of microorganisms isolated from periodontal pockets with a depth of more than 6 mm was even more pronounced and had a reliable character (90.0 and 40.0%, p <0.01 and 95 and 28.5%, p <0.01). With severe bleeding of the gums, most representatives of normal microflora were sown less frequently: streptococci “Salivarius” in 80.0 and 22.8% (p <0.01), staphylococci - 50.0 and 17.0% (p <0.05), lactobacilli - in 25.0 and 5.7% (p <0.05). The number of these microorganisms decreased by 1, -1.8 times, the difference in CFU / ml was especially significant for peptostreptococci -6.2 normal and 3.4 in patients.The detection rate of bacteroids slightly decreased (from 90.0 to 82.8%), however, the proportion of “odontogenic” bacteroids sharply increased from 2.8 to 61.8% (p <0.05). Also noteworthy is a more than twofold increase in the inoculation of fungi of the genus Candida (from 15.0 to 31.0%, p >0.05). The frequency of detection of actinomycetes increased in the presence of serous-purulent exudate (from 10.0 to 14.3%), the quantitative indicator of this microorganism increased 3.2 times - from 1.7 to 5.5 CFU / ml with suppuration.The results of our studies indicate that, as the inflammatory and destructive process intensifies and its clinical manifestations increase in the microbiological status of patients using implants based dentures, significant changes occur. They relate to the biocenosis of the implant-gingival sulcus: some bacterial groups characteristic of healthy individuals (neysseries, pneumococci, other cocci) disappear, the detectability of the majority of obligate and facultative anaerobes characteristic of this biotope (waillonella, peptostreptococcus, lactobacillus, green and green disappears). The leading role is played by "odontogenic" bacteroids, fungi of the genus Candida, to a lesser extent (due to a higher concentration) - actinomycetes and fusobacteria. In severe forms of reimplantitis, rarely identified A. actinomycetemcomitans, conditionally pathogenic aerobic species - P. aeruginosa and S. aureus also appear in the implant-gingival sulcus.Apparently, the simplest ones also play a significant role in the development of a more severe course of the disease, since their detection in native smears, as they move from mild forms of the disease to more severe ones, becomes more frequent. When analyzing the total number of associates in the oral cavity (both representatives of “normoflora” and opportunistic microorganisms), it turned out that in the control group and in patients with the initial stage of reimplantitis, 10-9 species and groups of microorganisms were mainly sown. In the control group, such results were obtained in 90% of the examined, in the initial stage of reimplantitis - in 96%. With moderate and severe course of the disease, there was a shift towards a decrease in the number of associates. In the first case, in 82.7% of patients, 8–6 species were sown from the oral cavity; in the second case, the number of associates in all patients did not exceed 7 (23.3%), but the majority were patients who had 6 (30.0% ) and 5 (46.6%) species. Carrying out a similar analysis, where the material for the study was the contents of the implant-gingival groove, showed that the total number of associates is significantly less. In the microbiocenosis of this biotope, the number of associates was: in healthy individuals, 7–6 (80.0%); in patients with an initial stage of reimplantitis - 6-3 (80.0%); moderate and severe degrees - respectively 5-3 (74.3%) and 4 -2 (93.4%).In addition, a clear pattern was observed in the implant-gingival sulcus more than 6 mm deep and in the severe course of the disease: the "odontogenic" bacteria, found in 80.0% of patients of the second group and 86.0% of patients of the third group, occupied the leading position. It should be emphasized that Acinobacillus actinomicetemcomitans were detected only when abscessing and the presence of purulent exudate were detected in 13.3% of cases, they were the only representatives of periodontopathogenic flora in high titers and in 2 cases stood out in association with Por. gingivalis. The study of samples of the oral cavity and implant-gingival sulcus showed that in the oral cavity of healthy individuals and in patients of the first group, the microflora is quite plentiful and consists of 9-10 or more associates. With the development of reimplantitis, the number of participants in the biocenosis decreases to 8-6 with an average degree and up to 7-8 with a severe degree of reimplantitis. An even greater “unification” occurs in the gingival pockets: if 7-6 species (groups) of bacteria are sown in healthy ones, then in patients with an average degree of 5-3, and in severe cases, no more than 4-2 types.In the oral cavity and in the implant-gingival sulcus of patients with moderate and severe severity, one or two representatives of this group dominated. This tendency is especially pronounced in the implant-gingival sulcus. According to some researchers (Ushakov R.V., 1998; Rabinovich I.M., 2002), a violation of the ratio of the number and composition of microorganisms can eventually acquire nosological independence and serve as an additional factor in the pathogenesis of chronic inflammatory diseases of the oral cavity. As the results of our studies have shown, in patients with peri-implantitis, the severity of the revealed violations of the biocenosis can be different. The distribution of patients according to the severity of dysbiotic disorders was carried out by us based on the calculation of the dysbiosis index (ID). Digital values were obtained by dividing the quantitative indicators of microorganisms according to the following formula:
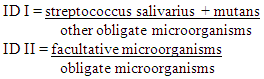 So, in individuals of the control group, the normal state of microflora was noted (ID 0.8-0.7). A dysbiotic shift (ID 0.7-0.6) was observed in patients with a mild degree of reimplantitis. Dysbiosis of the first degree (ID 0.6-0.4), diagnosed with moderate reimplantitis. Dysbiosis of the II degree (ID 0.06 or less) corresponded to a severe degree of reimplantitis. Such systematization is conditional and does not take into account all possible quantitative fluctuations. However, it allows a more differentiated approach to the diagnosis and complex treatment of the disease.Thus, microbiological studies have shown that in patients with periimplantitis, the biocenosis of the oral environment is significantly impaired. The most pronounced disorders of microflora, which are dysbiotic, are observed in patients with a severe degree of disease. The results of clinical and microbiological studies of patients indicate that the degree of disturbances in the biocenosis of the oral cavity is interconnected with the severity of the course of reimplantitis. Moreover, it was found that dysbiotic shifts aggravate the clinical picture of the disease.
So, in individuals of the control group, the normal state of microflora was noted (ID 0.8-0.7). A dysbiotic shift (ID 0.7-0.6) was observed in patients with a mild degree of reimplantitis. Dysbiosis of the first degree (ID 0.6-0.4), diagnosed with moderate reimplantitis. Dysbiosis of the II degree (ID 0.06 or less) corresponded to a severe degree of reimplantitis. Such systematization is conditional and does not take into account all possible quantitative fluctuations. However, it allows a more differentiated approach to the diagnosis and complex treatment of the disease.Thus, microbiological studies have shown that in patients with periimplantitis, the biocenosis of the oral environment is significantly impaired. The most pronounced disorders of microflora, which are dysbiotic, are observed in patients with a severe degree of disease. The results of clinical and microbiological studies of patients indicate that the degree of disturbances in the biocenosis of the oral cavity is interconnected with the severity of the course of reimplantitis. Moreover, it was found that dysbiotic shifts aggravate the clinical picture of the disease.