-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2020; 10(8): 614-619
doi:10.5923/j.ajmms.20201008.16
Received: July 1, 2020; Accepted: July 24, 2020; Published: August 15, 2020

Urethroplasty at Traumatic Strictures in Children: The Experience of One Institution
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKh. A. Akilov 1, S. S. Kariev 2, Sh. A. Nizomov 1
1Department of Surgery and Pediatric Surgery, Institute of Postgraduate Medical Education, Tashkent, Uzbekistan
2Department of Urology and Andrology, Institute of Postgraduate Medical Education, Tashkent, Uzbekistan
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Introduction The mechanism of urethral injury is similar in both boys and adult men. The difference is that more often in childhood there is an injury in the prostatic urethra and the neck of the bladder in 4-19% due to pelvic fractures as a result of motor vehicle incidents. The anterior urethra is affected by penetrating wounds of the penis. The complexity of the treatment is due to lifelong urinary complications such as recurrent strictures, urinary incontinence, and erectile dysfunction. Aim of study is to improve the treatment results of strictures and obliterations of the traumatic origin of the posterior urethra in children by improving (modifying) the surgical technique and using a two-diameter drainage catheter. Material and methods There were 50 boys at age of 3-15 years. 17 (34%) had strictures and 33 (66%) obliterations. By localization: in 23 (46%) patients in the membranous department, in the prostatic department - in 12 (24%) or both urethral sections - in 14 (28%). One patient (2%) had a complete separation of the urethra from the bladder neck with the subsequent development of stricture of the posterior urethra. The causes were injuries of the pelvic bones in 36 children (72%) and a fall from a height in 14 (28%). In terms of age, 5 children were from 3 to 7 years old, 28 at the age of 7 to 12 years and 17 were aged from 12 to 15 years. Results According to urethrograms data, the length of strictures and obliterations averaged 1.9 ± 0.2 cm. After excision, the diastasis between the proximal and distal parts averaged 3.8 ± 0.2 cm. In 98.0% of 50 operated children we received good results due to the use of a two-diameter drainage catheter. Only one patient had a relapse and was re-operated with good long-term results. Conclusion Careful preoperative preparation, accurate, gentle and economical resection of well-mobilized anastomosed ends of the urethra within healthy tissues and the use of a two-diameter drainage catheter, makes it possible to reduce the degree of tension of the anastomotic line both intraoperatively and in the early postoperative period.
Keywords: Trauma, Urethra, Stricture, Urethroplasty
Cite this paper: Kh. A. Akilov , S. S. Kariev , Sh. A. Nizomov , Urethroplasty at Traumatic Strictures in Children: The Experience of One Institution, American Journal of Medicine and Medical Sciences, Vol. 10 No. 8, 2020, pp. 614-619. doi: 10.5923/j.ajmms.20201008.16.
Article Outline
1. Introduction
- The mechanism of urethral injury is similar in both boys and adult men. The difference is that more often in childhood there is an injury in the prostatic urethra and the neck of the bladder in 4-19% due to pelvic fractures as a result of motor vehicle incidents. The anterior urethra is affected by penetrating wounds of the penis. The complexity of the treatment is due to lifelong urinary complications such as recurrent strictures, urinary incontinence, and erectile dysfunction [1-2].A comparative analysis of the Clinical Recommendations for urogenital system trauma of the European Association of Urology (EAU), American Association of Urology (AUA) and Société Internationale d'Urologie (SIU) showed that multicenter studies are still relevant today. This is necessary for optimization, improvement the quality and increasing the level of these documents evidence both for the diagnostics and treatment of urethral injuries [3]. Despite the successes achieved in the surgical removal of strictures and obliterations of traumatic origin (SOTO) of the membranous and prostatic sections of the urethra, the percentage of unsuccessful outcomes is still very large and they range from 25 to 50% [4-10]. And the spectrum of unsuccessful outcomes causes is very diverse, ranging from violations in primary care and diagnostics, ending with the imperfection and inaccuracies of surgical technique and postoperative management [11-13]. In this regard, the issue of preventing the formation of post-traumatic strictures and their relapse remains an urgent problem of pediatric surgery.Aim of study is to improve the treatment results of strictures and obliterations of the traumatic origin of the posterior urethra in children by modifying the surgical technique and using a two-diameter drainage catheter.
2. Material and Methods
- There were 50 boys at the age of 3-15 years. 17 (34%) had strictures and 33 (66%) had obliterations. By lo-calization: in 23 (46%) patients in the membranous department, in the prostatic department - in 12 (24%) or both urethral sections - in 14 (28%). One patient (2%) had a complete separation of the urethra from the bladder neck with the subsequent development of stricture of the posterior urethra. The causes were injuries of the pelvic bones in 36 children (72%) and a fall from a height in 14 (28%). In terms of age, 5 children were from 3 to 7 years old, 28 at the age of 7 to 12 years and 17 were aged from 12 to 15 years. Earlier, 31 (62%) patients were operated on in the clinics at the place of residence. Strictures and obliterations when they contacted us were recurrent. 17 of them were operated according to the Marion-Holtsov method, 14 patients - according to Kreiss-Fronstein. After these operations, 17 patients underwent prolonged unsuccessful urethral bougienages. The remaining 19 (38%) patients were not operated on before the admission to our hospital. All patients were performed ascending and descending urethrography, ultrasound of the urethra and bladder, urethroscopy, and, if possible, mictoscystic urethrography. If necessary, an examination of the bladder neck the internal opening of the urethra and urethral parts proximal to the affected area was made through the cystostomy fistula. After surgery, when catheters and the drains were removed, control uroflowmetry was performed. Erectile function was also evaluated by the presence of a spontaneous morning penile erection in a boy. All 50 patients already had suprapubic cystostomic drainage at admission. After urine sampling for bacteriological examination, drainage replacement and urinary tract sanitation were performed. At "controllability" of urinary tract infection, surgical treatment was performed - a modified Marion-Holtsov surgery with the installation of a two-diameter catheter - IDP patent No. 05277, 11/19/2001 (Fig. 1). A catheter was made during surgery, taking into account the anatomical parameters of the patient.
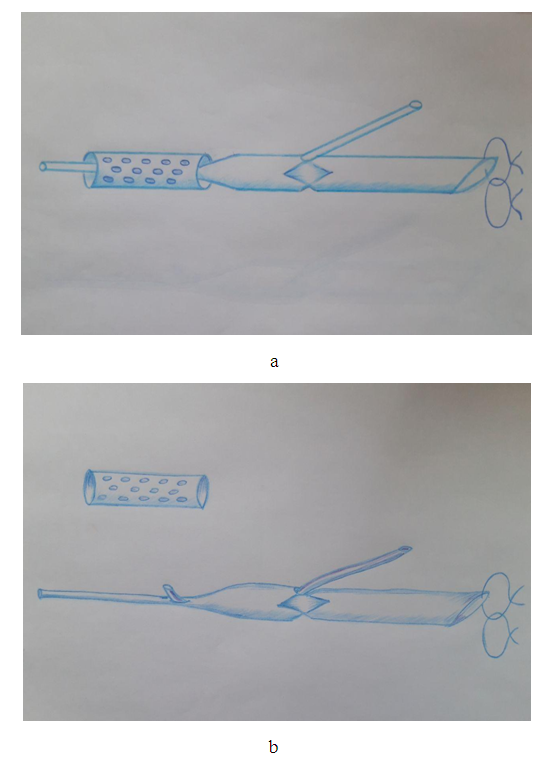 | Figure 1. Two-diameter catheter for drainage of the urethra and bladder: a) the whole element, b) a separate element |
3. The Technique of Modified Marion-Holtsov Urethroplasty
- Unlike V.I. Rusakov (1991), who offers a peak-shaped incision, we used the perineal incision strictly along the midline giving wide access to the posterior urethra. After dissection of the skin, subcutaneous tissue and exposure of the surface of the bulbar-cavernous muscle, it is separated from the spongy tissue of the urethral bulb. Then the muscle is removed on two sides, preserving it from damage as much as possible, since damage of this muscle is fraught by the development of erectile dysfunction. The spongy part together with the urethra is separated from the fixation site, dissecting the ligament that attaches to the lower edge of the pubic bones. The spongy tissue is not separated from the urethra, as L.A. Kudryavtsev (1993) recommends, as the wall of the children's urethra is very thin and delicate. The release of the urethra bulb is continued into the depths together with the membranous part to the prostate gland. After that, we cut off the urethra from the scar-changed part (at strictures and obliterations of the membranous section) or as close as possible to the scar-changed part of the urethra (when the stricture or obliteration is in the prostatic section, or in cases of separation of the urethra from the bladder neck). It must be remembered that every millimeter of non-scar-changed tissue of the urethral wall is very valuable for protecting the anastomosis line from tension. In the cases of repeated surgery, due to the numerous adhesions and scars of the surrounding tissues, as well as due to the complete obliteration of the membranous, prostatic, or both of these sections of the urethra, it is not possible to strictly observe the principle of topographic anatomical operations. Therefore, at this stage of the sugery, the main attention should be paid to the careful release of urethra distal part and its excision from the obliterated or stricture changed part. The removal of scars in the proximal section should be begun from the side of the inner surface of the pubic joint to avoid the prostate injury. After cutting off the scar tissue and finding the blunt end of the urethra proximal part, the wall of the urethra is carefully dissected and their ends are freed from the surrounding tissue. After thorough preparation of both ends of the urethra for the end-to-end anastomosis, the bladder was drained with two diameter cystic urethral tubes. The proximal end of the urethra (diameter 0.5-0.6 cm) is displayed on the suprapubic region, at the level of the Leto triangle. From the initial part of the neck of the bladder, the wall of this tube becomes thinner (diameter 0.15-0.18 cm) and another catheter with an external diameter of 0.4-0.5 cm is put on it, on the wall of which there are small multiple drainage holes. The end of both catheters is discharged through the external opening of the urethra by 5-6 cm (Fig. 2).
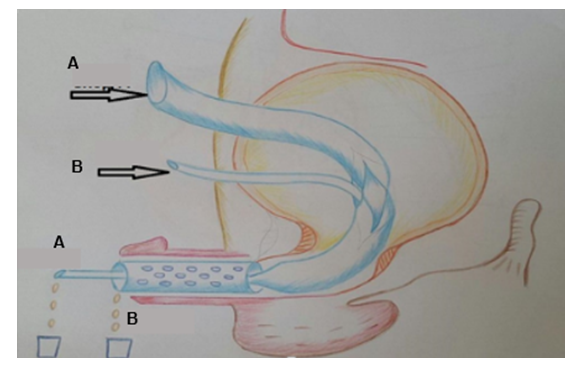 | Figure 2. The principal scheme of catheter functioning |
4. Results
- According to urethrograms, the length of strictures and obliterations averaged 1.9 ± 0.2 cm. The changed sections of the urethra were released intraoperatively, with great care. Amputation of the urethra scar-changed part was performed as close as possible to the pathological areas. After excision, the diastasis between the proximal and distal parts averaged 3.8 ± 0.2 cm. Therefore, the maximum mobilization of the distal part of the urethra was performed to reduce the tension of the anastomosis line. In one case mobilization of the bladder neck was performed in a patient with a separation of the urethra from the bladder neck. The next step was the installation of a polyvinyl chloride two-diameter catheter, the sizes of which were selected individually in each case. Then anastomosis was applied - monofilament sutures were arranged evenly around the circumference, as it was mentioned above. Early postoperative treatment did not differ from generally accepted principles. But at the same time, special attention was paid to 3 factors. The first factor is the selection of a parenteral antibiotic, when the basis was not only the result of a bacteriological study, but also the features of the microbial landscape of the entire cohort of patients. Nosocomial flora predominates in our patients, when a protected antibiotic with bactericidal ability against nosocomial strains with sufficient evidence should be chosen.The second factor is the continuous irrigation of the bladder offered by us with sterile solutions having an antiseptic component. Chlorhexidine bigluconate or dioxidine was used for it.The third factor is a regular irrigation of the urethral anastomosis site, followed by the introduction of antibiotics through the microcatheter we have proposed. By other words, we carried out a systematic local sanitation of the wound and local treatment of the infection. A microbiological investigation of urine with determination of the pathogen and sensitivity to antibacterial drugs was performed in 47 (94%) patients. Microflora growth was not detected at urine examination in 9 (18%) children and in 38 (76%) patients urine culture was positive. In 22 (57.9%) children the growth of microorganisms of the Enterobacteriaceae family was found, in 11 (28.9%) patients - the growth of microbes of the Proteus family, in 3 (7.9%) - St. saprophiticus and in 2 (5.3%) - Candida. We explain this variant of uropathogens seeding by the fact that 9 (18%) children received antibacterial treatment immediately before admission to the hospital. The sensitivity analysis of the isolated microorganisms was carried out only to antibacterial drugs approved for use in pediatric practice. Representatives of the Enterobacteriaceae family showed a high sensitivity to cefoperazone (86.4%), amikacin (81.8%), ceftriaxone (77.3%) and gentamicin (72.7%). These microorganisms are less sensitive to protected ampicillin (ampicillin clavulonic acid - 63.6%), cefuroxime and cefoxime (54.5%). Resistance was detected to doxycycline (86.4%), carbenicillin (90.9%), benzylpenicillin (95.5%), ampicillin (90.9%), cefazolin (81.8%) and cephalexin (72.7%). Microbes of the Proteus family were sensitive to cefoperazone (81.8%) and ceftriaxone (72.7%), gentamicin (63.6%), amikacin (54.5%). And a particularly high sensitivity in 86.4% of cases to protected third generation cephalosporins, and especially protected antipsevdomonas cephalosporins (cefoperazone + sulbactam - 90.9%). These microorganisms were insensitive to ampicillin, penicillin, doxycycline and polymyxin in 100% of cases. As it can be seen from the presented data, both microorganisms of the Enterobacteriaceae and Proteus family are highly sensitive to cephalosporins of the third generation. So, cephalosporin antibiotics of the third generation were chosen for parenteral administration, in particular, it was ceftriaxone and ceftriaxone sulbactam. If antibacterial therapy was not effective enough, an increase in body temperature and uncontrolled infection according to a step-by-step analysis of urine were replaced by cefoperazone sulbactam. Aminoglycosides (gentamicin) were used for the local application. In cases of Candida presence, flucanazole of 50 mg / day was included. Irrigation of the anastomotic area was carried out with sterile saline solution (0.9% sodium chloride solution) with an antiseptic. Chlorhexidine bigluconate (in all age groups) or Dioxidin (only in the older age group) was used as an antiseptic component. Chlorhexidine bigluconate in the form of a 0.5% sterile aqueous solution in glycerol gives both bacteriostatic and bactericidal effects. The bactericidal effect is manifested in a concentration of more than 0.01% at a temperature of at least 22°C and exposure for 1 min. Fungicidal action - and at a concentration of 0.05%, at a temperature of 22°C and exposure for 10 minutes. The drug is effective against gram-positive and gram-negative bacteria. It is stable and retains activity (although somewhat reduced) in the presence of blood, pus, various secrets and organic substances. It very rarely causes allergic reactions, irritation of the skin and tissues, does not have a damaging effect on objects made of glass, plastic and metals. For antiseptic treatment of the urethral wound site (anastomosis), a 0.5% sterile solution was prepared by diluting the drug in a ratio of 1:40 in 0.9% saline solution (sodium chloride) with sterile glycerin. A feature of this solution is its ability to increase the sensitivity of bacteria to chloramphenicol, kanamycin, neomycin, cephalosporins. For irrigation, 5-10 ml of the solution was injected through the drainage into the area of the anastomosis, usually 2-3 times a day. The treatment course is 7-9 days, daily, until the catheter is removed. Release form - Concentrate for the preparation of solutions for local and external use of 20% of 500 ml per bottle of colored polypropylene with a cap. Dioxidin (hydroxymethyl quinoxalindioxide) - a broad-spectrum antibacterial drug from the group of quinoxaline derivatives, has chemotherapeutic activity in infections caused by a vulgar protein, dysentery stick, Klebsiella, Pseudomonas aeruginosa, Salmonella, Staphylococcus aureus, Streptococcus ga. gangrene), acts on strains of bacteria that are resistant to other chemotherapy drugs, including antibiotics. The release form is a ready-to-use sterile solution in ampoules of 5 ml and 10 ml, with a dioxidine content of 5 mg (0.5%) or 10 mg (1%). Irrigation of the anastomosis area was carried out with a 0.5% solution through the drainage tube of the catheter from 10 to 50 ml, depending on the transparency and purity of the wash water 2 times a day. The treatment course is 7-9 days, daily, until the catheter is removed. Thanks to the use of a special drainage catheter in no case we observed local complications of infectious origin. It made possible to prevent relapse, as noted by other surgeons. In only one case, a stricture recurrence was observed. This was a re-operation, when during the intervention a large extent of diastasis was found between the healthy ends of the urethra. It turned out to be more than 6 cm, and in this patient we had to use a scrotal skin flap on a vascular pedicle for technical reasons to restore the urethra. The conducted local manipulations and the technique of the surgery led to a smooth flow of the early postoperative period. No general or local complications were observed. The wounds healed primarily. It allowed the removal of a special drainage catheter from the urethra no later than 8-9 days. The maximum volume of the bladder, its wall thickness, the volume of residual urine and the time of urination were monitored after the surgery. Deviations from the age criteria of the norm were not found in the results of these studies. No significant differences with the data of the long-term examination were also observed. 49 children had no complaints, the urine stream was normal, the data of the simplified uroflow metric index (Goldberg BB, 1974) were within normal limits (14.3 + 3.3 ml / s after the catheter removal on the 10th day after surgery; 23.6 + 4 , 9 ml / s 3-6 months after surgery; 24.9 + 5.8 ml / s 12 months after surgery, P> 0.05). Taking into account all the objective data, a stricture recurrence at the site of the anastomosis was excluded. The results of the surgery after 3-6 months (n = 44) and 1 year (n = 36) were checked by means of a survey, direct examination and investigation.
5. Discussion
- The problem of urethral strictures treatment in children is a very difficult task. Today, there are various methods of treatment, ranging from endoscopic procedures, ending with open surgical interventions. Urethral strictures in children have a huge impact on their future lives if they are not treated properly. The problem has not only a material side, but the psychological aspect, both for the child and for the whole family, is no less important. Therefore, the main goal of the surgeon is to search for a minimally invasive procedure with short healing times. In the works of R. Novak (1983) good results were obtained only in 71% of cases from 99 operated patients; repeated intervention was required in 14 patients (28.6%). H. Zincke, L. Furlow (1985) performed 44 surgeries in children, good results were obtained in 22 patients, and 10 needed constant bougieunage. V.N. Tkachuk, B.K. Komyakov (1990) noted relapses in 56% of the operated patients due to the post-traumatic urethral strictures. During Marion-Holtsov surgery there was a relapse of the urethra posterior parts in 3 patients from 7 cases (Kudryavtsev L.A., 1993).A. Ahmed, G. S. Kalayi (1997) noted relapse in 20.9% of cases after an anastomosis of the urethra "end to end", which were then reoperated. G. Gibson (1970) observed impotence in 42% of cases after surgical removal of the stricture of urethra membranous part, G.S. Webster et al (1983) - in 45% of cases. After the Marion-Holtsov surgery in the Frakman-Rusakov modification, similar complications were registered in 3/4 of the patients (L. Kudryavtsev, 1993). As it is known, at this type of surgery, the bulb-cavernous muscle is separated from the attachment site together with the urethra, i.e. as a single unit (Rusakov V.I., 1991). We prepared a questionnaire for a retrospective analysis of the unsuccessful treatment reasons of 31 patients with recurrent strictures. Possible reasons in it were divided into groups: technical, local and general. Technical reasons included intraoperative errors - incomplete removal of scarred tissue (67.7%), unsuccessful suturing of the anastomosis (61.3%), poor-quality suture material (61.3%), strong anastomosis line tension (64.5%) and inefficient drainage of the bladder (87.1%). Local reasons included stasis in the area of the anastomosis, local urinary infection.Common reasons include the lack of a systematic approach at the prehospital stage, when iatrogenic damage or aggravation of damage is often observed as a result of multiple and sometimes violent attempts to catheterize the urethra at the initial stages of emergency care (87.1% of cases). This is the result of non-compliance with emergency care standards, which indicate that retrograde urethrography is the primary diagnostic procedure for choosing a specific assessment of possible damage to the urethra and determining subsequent actions by specialists [14].Another factor leading to the ineffectiveness of surgical treatment of urethral strictures should be considered the occurrence of spontaneous erections in the early postoperative period (80.6%). Common causes of unsuccessful outcomes of surgical treatment of SOTO in the posterior urethra are incomplete removal of scarred tissue, unsuccessful suturing of the anastomosis, strong tension of the anastomosis line in the immediate postoperative period, as well as inefficient drainage of the bladder, catheter-associated urinary tract infection (UTI). The successful and complete elimination of the above-mentioned complications causes is the key to the successful treatment of SOTO of membranous and prostatic urethra. A modification of the Marion-Holtsov surgery has been proposed to solve technical problems. Attention was focused on the accuracy and sequence of each stage which were framed in the form of an algorithm. At each stage, the surgeon is focused on preventing possible complications, the frequency of occurrence of which was determined above. Further, in the immediate postoperative period, effective drainage of the bladder and catheter-associated UTI plays an important role. In our observations, the most common pathogens of infectious and inflammatory diseases of the urinary system are microorganisms of the Enterobacteriaceae and Proteus families, less often St. saprophiticus. A similar spectrum of microorganisms in the microbiological examination of urine was obtained by most authors [13,16-18]. The data of bacteriological studies allowed us to determine that bacteria from the group Enterobacteriaceae and Proteus were most sensitive to third-generation cephalosporins, especially ceftriaxone and cefoperazone, as well as aminglicosides. The empirical selection of antibacterial drugs of the second generation of cephalosporins and synthetic penicillins for the prevention and treatment of microbial inflammatory diseases of the urinary system, which is most often practiced in pediatric clinical practice, is not justified. These data are consistent with those of scientific publications [13,16-17].The correct selection of antimicrobial therapy components in the preoperative and postoperative period, achieving UTI controllability, effective drainage in the early postoperative period and flushing of the anastomosis zone prevents infection and has a beneficial effect on healing processes and is the main feature of relapse prevention. In this connection, we believe that protected cephalosporins such as ceftriaxone or cefaperazone should be preferred for parenteral administration in our region and aminoglycosides (amikacin, gentamicin) - for the local application (for irrigation of wounds). The next main task is adequate drainage and irrigation of the bladder cavity, and most importantly - the anastomotic zone and the lumen between the drainage and the urethral wall. Proposed catheter solves these problems. Both drainage and sanitation are carried out with its help by irrigation of the cavity of the bladder, anastomosis zone and the lumen between the drainage and the urethral wall. In addition, intraoperative preparation of a polyvinyl chloride catheter, as well as taking into account the anatomical features of each patient, can prevent local irritation and spontaneous erections in the early postoperative period.Another important criterion for assessing the quality of performed surgical treatment is preservation of erectile function. It was estimated by the presence of spontaneous morning penile erections. So, from 31 patients who had already been operated on before admitting to our hospital, erectile dysfunction was detected in 18 (58.1%) patients. Erectile dysfunction was observed only in 2 (10.5%) of 19 patients who underwent a primary Marion-Holtsov operation using a two-diameter catheter. Erectile dysfunction was no longer observed in both of these patients at re-examination after 3 months.In our observations, in 19 patients who did not have catheterization when going to the hospital, the results of the primary surgical treatment of strictures and obliterations were highly effective in compare to those patients who had repeated attempts to catheterize the bladder before performing urethrography. The similarity was only in the fact that in both groups they paid attention to the treatment of UTI in the preoperative period. It is important that in most cases, during long-term catheterization, microorganisms populate only a catheter. It is confirmed by the results of bacteriological studies of urine taken by suprapubic puncture [13].98.0% of 50 operated children had good results due to the use of a two-diameter drainage catheter. Only one patient had a relapse that was reoperated with good long-term results. The other significant complications associated with the underlying disease were not observed.
6. Conclusions
- Careful preoperative preparation, accurate, gentle and economical resection of well-mobilized anastomosed ends of the urethra within healthy tissues and the use of a two-diameter drainage catheter provides an opportunity to reduce the degree of tension of the anastomotic line both intraoperatively and in the early postoperative period (by preventing spontaneous erections), it also prevents local complications of UTI, and allows to prevent the recurrence of posterior urethra SOTO in children. Due to this, good results were received in 98.0% of children. Only one patient had a relapse that was reoperated with good long-term results.Thus, the full and correct implementation of the provisions of the first aid algorithms for urethral injuries, the thorough preparation and the correct execution of the stages of surgical manipulation of the urethral anastomosis using a two-diameter drainage catheter, with the correct selection of antimicrobial agents for parenteral and local use, allowed to achieve good results in 98, 0% of cases, including cases of repeated correction in case of recurrent strictures and urethral obliteration. An integrated protocol approach is the main tool for preventing complications and relapses the posterior urethra SOTO in children. The proposed two-diameter drainage catheter offers promising results for widespread use.