-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2020; 10(8): 563-566
doi:10.5923/j.ajmms.20201008.05

Justification of Simultaneous Operations on the Organs of the Abdominal Cavity and Abdominal Wall in Patients with Ventral Hernia
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKurbaniyazov Zafar Babajanovich, Mardanov Bobosher Amirovich, Davlatov Salim Sulaymonovich, Rakhmanov Kosim Erdanovich
Samarkand State Medical Institute, Republic of Uzbekistan, Samarkand
Correspondence to: Davlatov Salim Sulaymonovich, Samarkand State Medical Institute, Republic of Uzbekistan, Samarkand.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Relevance. According to domestic and foreign literature, 15-20% of patients who underwent hernia repair, in the coming years after surgery undergo repeated surgical interventions for other surgical diseases. The aim of the study is to improve the quality of treatment of patients with ventral hernia by reducing the frequency and severity of complications after simultaneous and reconstructive surgery on the abdominal organs and abdominal wall. Materials and research methods. The study included the results of treatment of 197 patients with simultaneous pathology of the abdominal cavity and abdominal wall, admitted to the surgical department of the 1st clinic of Samarkand State Medical Institute. The results of the study. On average, one patient in the comparison group had 2-3 complications in the form of a combination of bronchopulmonary and / or cardiovascular complications with wound complications. In general, in the comparison group there were 17 (18.3% of 93) patients with various complications. Findings. Improving the tactical and technical aspects allowed: in 47.1% of cases in the main group to perform a simultaneous operation from separate two accesses and thereby reduce the frequency of performing simultaneous operations through one access to 52.9%, and the duration of the operation from 98.5 ± 4,9 to 72.5 ± 2.9 minutes (t-test = 4.23; p <0.001).
Keywords: Ventral hernia, Simultaneous operations, Abdominal cavity, Postoperative complication
Cite this paper: Kurbaniyazov Zafar Babajanovich, Mardanov Bobosher Amirovich, Davlatov Salim Sulaymonovich, Rakhmanov Kosim Erdanovich, Justification of Simultaneous Operations on the Organs of the Abdominal Cavity and Abdominal Wall in Patients with Ventral Hernia, American Journal of Medicine and Medical Sciences, Vol. 10 No. 8, 2020, pp. 563-566. doi: 10.5923/j.ajmms.20201008.05.
1. Relevance
- According to domestic and foreign literature, 15-20% of patients who underwent hernia repair, in the coming years after surgery are subjected to repeated surgical interventions for other surgical diseases [2,5].This determines the urgency of the problem of simultaneous operations. Attention should be paid to the irrationality of performing only hernia repair in case of hepatitis A if the patient has a combined disease of the abdominal organs. If only hernia repair is performed, repeated surgery for abdominal pathology often negates the results of hernioplasty [1,4,7].The analysis of the literature indicates that current trends in the treatment of patients with hepatitis B and simultaneous surgical diseases of the abdominal cavity and the prevention of complications in the early and long-term postoperative periods are based on the restoration of the abdominal wall function, physical rehabilitation after surgery and the achievement of a cosmetic effect. A significant percentage of unsatisfactory outcomes, the lack of a choice of the optimal treatment method, prompt further research in this area [3,6]. In connection with the foregoing, it seems relevant to develop effective methods and principles of surgical treatment of patients with large and giant umbilical and postoperative ventral hernias in combination with another pathology of the abdominal organs. The development of simultaneous and reconstructive surgery on the organs of the abdominal cavity and abdominal wall in patients with ventral hernias requires an integrated approach consisting of many component tasks within the framework of one problem.The aim of the study is to improve the quality of treatment of patients with ventral hernia by reducing the frequency and severity of complications after simultaneous and reconstructive surgery on the abdominal organs and abdominal wall.
2. Materials and Research Methods
- The study included the results of treatment of 197 patients with simultaneous pathology of the abdominal cavity and abdominal wall, admitted to the surgical department of the 1st clinic of Samarkand State Medical Institute.Depending on the tactics of preoperative preparation and the choice of surgical intervention, patients are conditionally divided into two groups: In 2012-2015. operated on 93 (47.2%) patients who made up the comparison group. From 2016 to 2019 under our supervision there were 104 (52.8%) patients who entered the main group.Preoperative preparation of patients of both groups was carried out according to standard methods. The physical status of patients in the comparison group was evaluated by the ASA classification. All patients took into account the presence of concomitant somatic diseases. In the preoperative preparation algorithm, we included those items that directly affect the identified and correctable risk factors.191 patients had one concomitant surgical pathology of the abdominal organs, and 6 patients had two. All patients in the study groups underwent simultaneous operations.After a thorough preoperative preparation in the preoperative period, the surgeon must solve at least two questions: 1. Operation access, simultaneous operation to be performed through one access or two separate accesses; 2. If it is necessary to perform through separate accesses, which stage should be performed first, the main stage or the simultaneous stage.Since in all the patients examined by us, the main pathology was a ventral hernia, and the simultaneous pathology was a surgical disease of an organ of the abdominal cavity when choosing a surgical approach, first of all, the location of the hernia gate, then the location of the organ with simultaneous pathology in the areas of the abdominal cavity was taken into account (fig. 1).
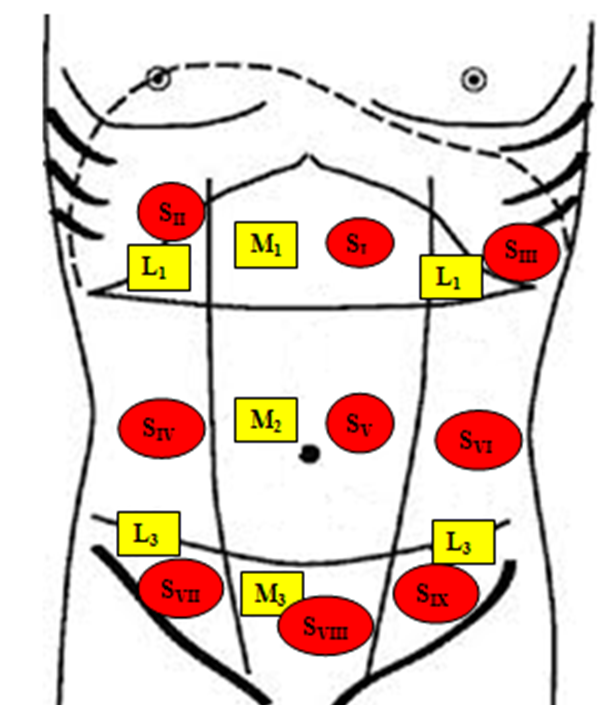 | Figure 1. A schematic arrangement of a hernia in the anterior abdominal wall and of simultaneous abdominal pathology (L, M - localization of the hernia Chervel J. P and. Rath A. M (1999),. S - localization of simultaneous disease in different areas of the abdominal cavity) |
|
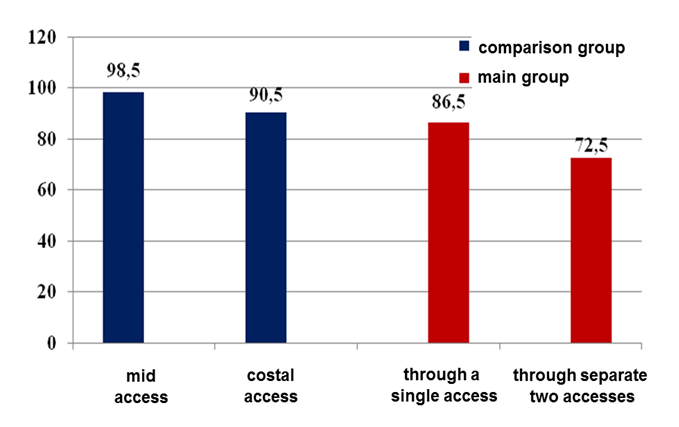 | Figure 2. Comparative indicators of the duration of the operation (min) depending on the access undertaken |
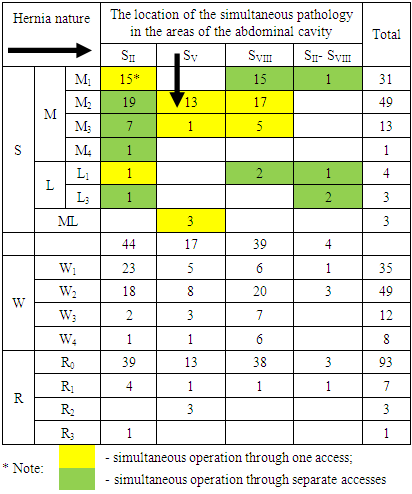
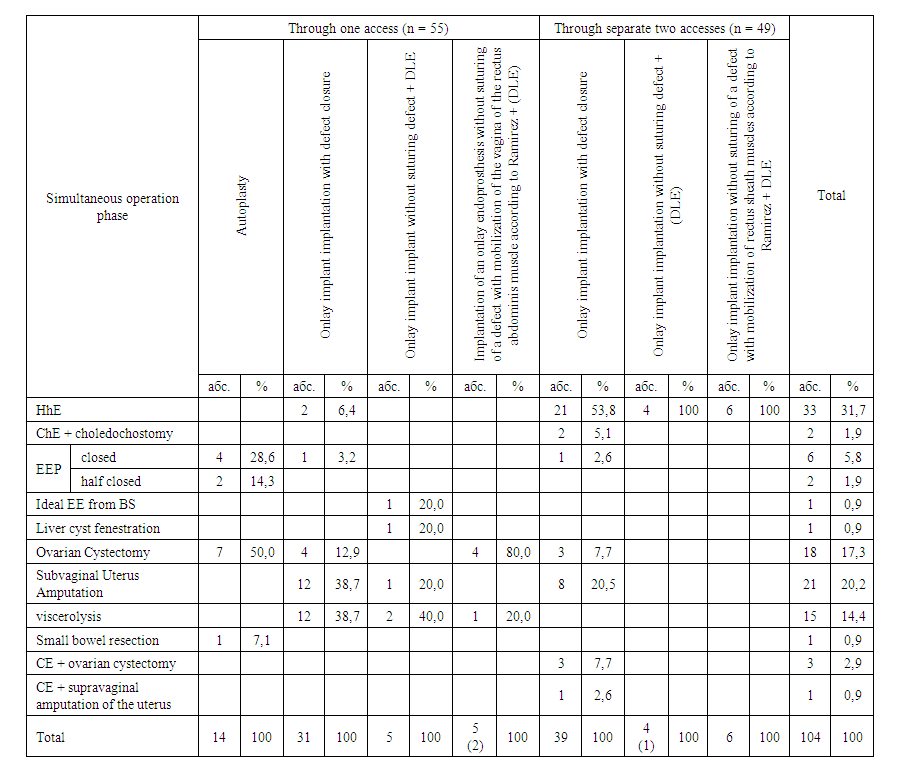 | Table 2. The nature of the performed simultaneous operations in patients of the main group |
3. The Results of the Study
- On average, one patient in the comparison group had 2-3 complications in the form of a combination of bronchopulmonary and / or cardiovascular complications with wound complications. In general, in the comparison group there were 17 (18.3% of 93) patients with various complications. In the main group there were 9 (8.6% of 104) patients with various complications. Relative improvement in the number of complications showed a significant improvement in the main group (Criterion χ 2 = 4.043; Df = 1; p = 0.045) (fig. 3).
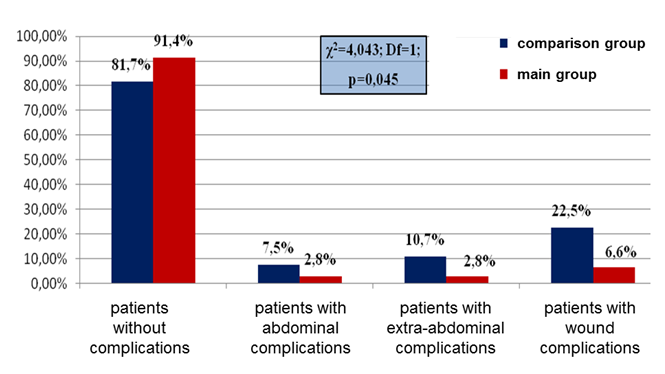 | Figure 3. The distribution of patients according to the frequency of complications after simultaneous surgery |
4. Findings
- Improving the tactical and technical aspects allowed: in 47.1% of cases in the main group to perform a simultaneous operation from separate two accesses and thereby reduce the frequency of performing simultaneous operations through one access to 52.9%, and the duration of the operation from 98.5 ± 4,9 to 72.5 ± 2.9 minutes (t-test = 4.23; p< 0.001). The application of the proposed algorithm, taking into account the improved tactical and technical aspects of surgical treatment of hypertension with simultaneous surgical pathology of the abdominal organs, reduced the overall frequency of postoperative complications from 18.3% to 8.6% (p = 0.045), including wound from 22.5% to 6.6% and extra-abdominal from 10.7% to 2.8%, as well as significantly reduce the duration of surgical treatment and rehabilitation periods after various options for hernioplasty.