D. I. Akhmedova1, 2, N. N. Ergasheva2
1Republican Specialized Scientific and Practical Medical Center of Pediatrics, Tashkent, Uzbekistan
2Tashkent Pediatric Medical Institute, Tashkent, Uzbekistan
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Urgency of problem. Congenital intestinal obstruction in newborns causes insufficient digestion and elimination of enterotoxins, makes a significant contribution to the development of endogenous intoxication, dramatically worsening the adaptive capabilities of the child's body. The presence of endotoxemia at newborns with congenital intestinal obstruction due to increased permeability of the intestinal wall, the catabolic orientation of metabolism, exacerbated by water-electrolyte disturbances can affects the intensity of reparative processes after surgical correction of the defect. The aim of the research was to determine the type and grade of endogenous intoxication in newborns with various clinical and anatomical forms of congenital intestinal obstruction before and after surgical treatment. Material and methods. The parameters of endogenous intoxication (middle-weight molecular peptides, malondialdehyde, lactate, bilirubin, creatinine levels) were measured in the blood serum of 208 newborns with various clinical and anatomical forms of congenital intestinal obstruction. Results. It was proved that endogenous intoxication (EI) in newborns with congenital intestinal obstruction is multiplex and composed of metabolic and resorption components. Metabolic component of EI includes middle-weight molecular peptides (MMP), malondialdehyde (MDA). Concentration of middle-weight molecular peptides was statistically significant (p <0.05) increase versus control in all cases of congenital intestinal obstruction in newborns, furthermore MMP level increase was more expressed at newborns with low congenital intestinal obstruction. The resorption component of endogenous intoxication at congenital intestinal obstruction was increased due to bilirubin, it was significantly higher at newborns with low congenital intestinal obstruction versus patients with high congenital intestinal obstruction. The lactate level was within the reference interval for all newborns, regardless of the level of congenital intestinal obstruction. Before surgery the metabolic component of the endogenous intoxication - malondialdehyde, as well as protein-energy, water-electrolyte disorders and weight loss were more evident at newborns with high congenital intestinal obstruction. In spite of this, regression of endogenous intoxication after surgery was faster in this patients with high intestinal obstruction versus newborns with low intestinal obstruction. Conclusion. Congenital intestinal obstruction in newborns is accompanied by EI of mixed genesis with a predominance of metabolic and resorption components. Before surgery high level of MDA, as a result of hypoxia, membrane destruction and tissue necrosis is a distinctive feature of high congenital intestinal obstruction and malrotation. After surgery regression of MDA level was faster in patients with high intestinal obstruction versus newborns with low intestinal obstruction, that had significantly high level of MMP.
Keywords:
Newborns, Congenital intestinal obstruction, Endogenous intoxication
Cite this paper: D. I. Akhmedova, N. N. Ergasheva, Intensity of Endogenous Intoxication in Newborns with Congenital Intestinal Obstruction and Its Grade after Surgical Treatment of the Disease, American Journal of Medicine and Medical Sciences, Vol. 10 No. 6, 2020, pp. 410-415. doi: 10.5923/j.ajmms.20201006.13.
1. Introduction
Congenital intestinal obstruction (CIO) in newborns is one of the most common reasons for hospitalization in a surgical hospital and surgical intervention [1]. Due to the peculiarities of the clinical and radiological manifestations, the differences in the nature of the complications, CIO is divided into high, low and malrotation of the intestine [2-3]. In recent years, the detection of CIO has been increasing, which is associated with an improvement in ante- and postnatal diagnostics [4]. With the introduction of effective surgical methods, anesthetic management and optimal methods of parenteral nutritionin to practice of neonatology, survival increases annually and at isolated defects it makes up 95% [3]. At the same time, the severity of the pathology itself against the background of more than 80% of cases of concomitant conditions (aspiration-atelectatic pneumonia, birth injury, intrauterine infection, necrotic enterocolitis) is exacerbated, that causes many complications and a high frequency of deaths [5-7]. CIO in newborns, which causes insufficient digestion and elimination of enterotoxins, makes a significant contribution to the development of endogenous intoxication (EI), dramatically worsening the adaptive capabilities of the child's body [8]. The genesis of EI at CIO is presumably mixed, since retention, exchange, and resorption components are not excluded. EI is developed as a result of a combination of several types of disorders: disorders of the central, micro- and lymphocirculation, hypoxia, immunity disorders and anti-infection protection at the failure of the control of these processesintegration [9]. In this case, metabolic disorders depend on the nature of the damaging factor and the response to it of the macro- and microcirculation system in accordance with the violation of transport and tissue extraction of oxygen, activation of the sympathetic-adrenal system [10]. This leads to a syndrome of hypermetabolism typical for a critical state - tissue needs for various substrates providing compensatory-adaptive mechanisms for energy conservation, preventing protein breakdown, reducing the utilization of fatty acids, increasing of gluconeogenesis and glucose tolerance, and intensifying of endothelial permeability [10-11,2]. The effectiveness of surgical treatment of CIO in newborns and the prognosis of the disease depend on the severity of the defect, concomitant diseases, the degree of tension of adaptive capabilities and the general reactivity of the newborn's body. The presence of endotoxemia at CIO due to increased permeability of the intestinal wall, the catabolic orientation of metabolism, exacerbated by water-electrolyte disturbances affects the intensity of reparative processes after surgical correction of the defect.Aim of the research was to determine the type and grade of endogenous intoxication in newborns with various clinical and anatomical forms of congenital intestinal obstruction before and after surgical treatment.
2. Material and Methods
There were observed 208 newborns with CIO in the department of Neonatal surgery of the Republican Perinatal Center in the period from 2009 - 2019: congenital high intestinal obstruction (CHIO) - 68 (33%), congenital low intestinal obstruction (CLIO) - 93 (45%), intestinal malrotation (IM) - 47 (22%). X-ray and ultrasound data were taken into accountin the differential diagnostics of various forms of the CIO course. A clinical examination of the newborn, estimation of the condition severity were carried out in accordance with the recommendations of N.N. Volodin [8,12]. The clinical and radiological manifestations of CIO, the influence of ante-and intrapartum factors, obstetric history and the nature of the comorbidity, aggravating the somatic status of the newborn were studied. (pic.1). 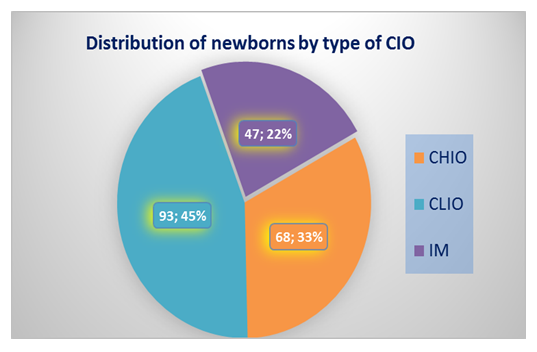 | Picture 1. Distribution of newborns by type of CIO |
The type and grade of EI were evaluated according to following markers: middle-weight molecular peptides (MMP), malondialdehyde (MDA) as a metabolic component of EI, creatinine as retention component; lactate, bilirubin as resorption components of EI [13]. Serum creatinine, bilirubin, and lactate were measured on biochemical analyzer “Mindray BS-120” (China) using standard reagent kits manufactured by “VITAL” OJSC (Russia). The concentration of malondialdehyde was determined by the thiobarbituric acid (TBA) test according to the method of N. Ohkawa et all. [14].The level of MMP in blood plasma was evaluated on N.I. Gabrielian et all. [15] manner; the absorption spectra of the supernatant were recorded using a “F 96” double-beam spectrophotometer (China) at wavelengths from 220 to 310 nm with the construction of a spectrogram. MMP content was measured at wavelengths of 220, 254, 260, 280 nm. The maximum absorption, as a rule, occurred at some one of the wavelengths. Based on the results of photometric measurements of the supernatant, the prefered component of the total MMP fraction was revealed. Evaluation of EI was done before surgery and 10 days after surgery. The comparison group (control) was consisted of 20 newborns without somatic and surgical pathology. Biochemical tests were available at 74 newborns and in 20 controls.
3. Results and Discussion
The main clinical signs of high intestinal obstruction were abdominal distention in the epigastric region (ADER) at 68 (100%), vomiting (V) at 66 (97%), growing symptoms of exsicosis with electrolyte imbalance (EEI) at 67 (98,5%) newborns. The type of vomiting (with or without bile impurity), the volume of vomit (in abundant or moderate amounts) and meconium discharge depended on the degree (full or partial) and the location of the obstruction (above or below) the duodenal papilla.At low intestinal obstruction, which often manifests itself as complete obstruction, the clinical picture was dominated by a sharp bloating and ADER at 47 (50,5%), total lack of stool and gas discharge (TLS) at 93 (100%), later vomiting – at 52(55,9%) and peritonitis at 35 (37,6%) of newborns. The degree of compression or inversion in individual parts of the small intestine or throughout the middle intestine had a decisive importance in the clinical course of intestinal malrotation. Vomiting with an admixture of bile, streaks of blood, secretion of blood from the rectum clearly indicated an inversion. During malrotations with inversion, the condition of the neonates progressively worsened: intoxication, dehydration, and electrolyte disturbances increased. Anxiety was replaced by lethargy, adynamia, a decrease in physiological reflexes; gray in color and marbling skin (MS) observed in 93,6% patients with IM. Clinical signs varied according to type of CIO (pic.2).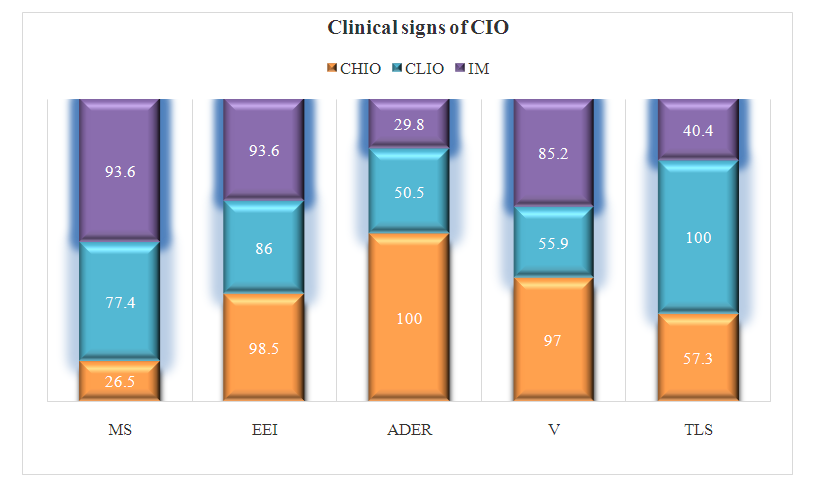 | Picture 2. Clinical signs of CIO in newborns, % |
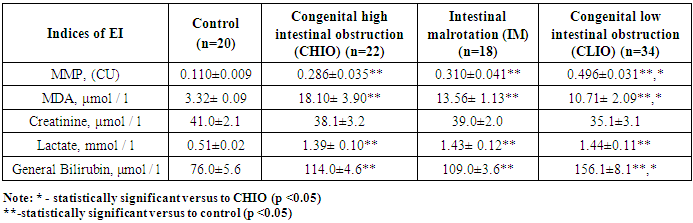
In 104 (50.2%) newborns intestinal obstruction developed on the background of intrauterine infection, trauma in childbirth, perinatal damage to the central nervous system, asphyxiation.It was found that the average MMP level in all newborns with CIO was higher relative to the control, with the highest increase being found in the group of neonates with CLIO. Their MMP was significantly higher relative to those ones with CHIO; in the group of neonates with malrotation the concentration of MMP was comparable to that one at CHIO. The MDA level was significantly higher versus the control in all newborns with CIO, however, there were no statistically significant differences depending on the level of intestinal obstruction. At the same time, higher average MDA values were observed in newborns with CHIO and intestinal malrotation relative to CLIO, although differences regarding CLIO were not significant. At CIO due to malrotation, when partial CHIO occurs and signs of intestinal obstruction prevail, causing circulatory-ischemic disorders, the MDA level was comparable to that in CHIO, i.e. higher than at CLIO. This may be due to the fact that the intensity of lipid peroxidation increases with hypoxia, which inevitably accompanies strangulation (Tab.1).Table 1. Markers of endogenous intoxication in newborns with various forms of CIO
 |
| |
|
We believe that the sharp increase in MMP during CLIO is due to massive degradation of proteins in the intestine and the active absorption of products of incomplete catabolism in conditions of stagnation of intestinal contents, as well as the absorption of some low molecular weight microbial toxins, degradation products of intestinal tissue proteins. As it is known, the MMP fraction in the blood is 80% represented by substances of protein and peptide nature with a molecular weight of 10-500 Da. These protein toxins have a high content of dicarboxylic and low content of aromatic amino acids. MMPs include products of hydrolysis of fibrinogen, globulins, glycoprotein catabolism, oligosugar (often of microbial origin), as well as fragments of certain hormones (adrenocorticotropic hormone, angiotensin, endorphins, encephalin) [15-16]. MMP also includes a number of biologically active substances, such as parathyroid hormone, neurotoxins X, inhibitors of phagocytosis, hematopoiesis, glucose utilization and amino acid transport; factors of separation of respiration and phosphorylation. This determines the toxicity of MMP and their negative effect on erythropoiesis, inhibition of the reaction of rosette formation and inhibition of mitochondrial respiration; DNA synthesis disorders in hepatocytes and lymphocytes; impaired synthesis and utilization of glucose, enzyme activity, creatinine excretion [17-18]. A high level of MMP at CIO can make a significant contribution to the violation of the adaptive reactions formation in the newborn. A specific feature of the toxic effect of MMP is that they have a direct membrane-toxic effect and initiate lipoperoxidation, the end product of which is MDA [13]. We believe that an increase of MDA which characterizes the intensity of lipid peroxidation, indicates the presence of evident membrane-destructive processes at CIO in newborns and there is a pronounced metabolic component of EI, which disrupts the adaptation process. It is important to note that in neonates with CIO there was a wide range of fluctuations in the values of MDA and MMP, which was reflected in standard deviation. So, the level of MDA at CHIO was in the range of 3.8-49.5 μmol / l, at CLIO - 5.3 - 14.7 μmol / l; MMP concentration varied between 0.170-0.390 CU and 0.197-0.510 CU at CHIO and CLIO, respectively.A study of the level of the EI retention component revealed the absence of significant differences in the creatinine index both from the control and between the groups with high and low CIO. The calculation of glomerular filtration rate (GFR) also did not reveal significant differences from the control, although 3 out of 83 neonates with low CIO had a decrease in GFR to 52-45 ml / min due to toxic nephropathy. The obtained results of an average level of creatinine and GFR as a whole indicate satisfactory renal function in newborns with CIO and the absence of the retention component of EI associated with renal filtration.Determination of the resorption component of EI (lactate, bilirubin) revealed its moderate contribution to EI. So, the level of lactate in the venous blood was 2.8-2.9 times higher relative to the control in children with CIO, while the changes in its concentration were within the reference interval (0.56-1.39 mmol / l), and there were no reliable differences between the CHIO, CLIO and malrotation groups. In 5 cases (3 with CLIO and 2 with CHIO), the lactate level was more than 2.4 mmol / l, that indicates risk of adverse outcome. There were shifts in the acid-base environment characteristic of metabolic acidosis with respiratory alkalosis in these neonates, they needed intensive therapy to normalize their state. The concentration of bilirubin in neonates with CLIO was significantly higher than in neonates with CHIO. It is known, that bilirubin has a wide spectrum of toxic effects, mainly being a membranotoxic agent: bilirubin may integrate into membranes and penetrating into the cell, it damages mitochondrial membrane lipids and causes energy metabolism abnormalities. In case of albumin concentration decrease in blood, bilirubin can diffusing through cell membranes into the cerebrospinal fluid, into the tissue and cause disturbances. Both it can be as a result of displacement bilirubin from the complex with albumin. Bilirubin inhibits blood coagulation, utilization of glucose by cells, disrupts enzyme activity and ionic cell impermeability [19]. Thus, CIO in newborns is accompanied by EI of mixed genesis with a predominance of metabolic and resorption components. High level of MDA, as a result of hypoxia, membrane destruction and tissue necrosis proved as a distinctive feature of CHIO and malrotation. High level of MMP, bilirubin, as a result of resorption of endogenous and exogenous toxins, dysbiosis was proved as a feature of CLIO in newborns.Analysis of EI after surgical treatment of CIO showed that the dynamics of MMP and MDA were multidirectional and depended on the type of CIO (Tab.2).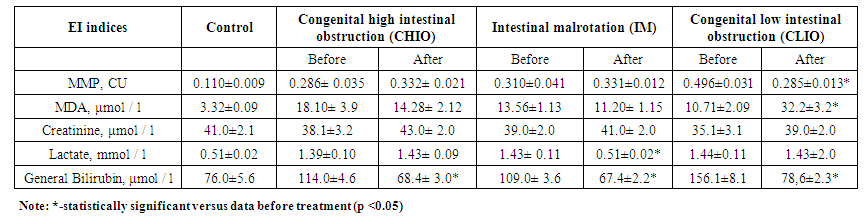 | Table 2. Indices of EI in newborns with CIO at the stages of surgical treatment |
As it can be seen from the table, the MMP level on the 10th day after the surgery in newborns with CHIO and IM did not statistically significant (p>0,05) change versus level before treatment. We suppose, that it may be due to massive surgical trauma and reduced adaptive capabilities in newborns with CIO. Only in newborns with CLIO MMP level decrease 1,7 times versus level before treatment (p<0,05). We can explain it fact by version about significant role of large intestine and its microbiota in MMP production at low CIO, which dramatically increased at CLIO and decreased progressively after surgery and microbita correction. Nevertheless it needs in future investigations. The MDA level had a trend to decrease in children with malrotation and high CIO after surgery (p>0,05). We suppose, that it may be caused by some elimination of strangulation, the restoration of microcirculation and tissue hypoxia, which was accompanied by a decrease in the generation of the reactive oxygen species and lipid peroxidation. At the same time, at low CIO, the MDA level significantly increased versus level before surgery. Probably, it was associated both with the phenomenon of hypermetabolism due to EI, the accumulation of toxins and MDA in tissues before surgery and some aspects of surgical trauma and wound healing in newborns with CLIO. Massive emission of the end products of catabolism from intestinal tissue and lumen can be a consequence of the intestinal obstruction elimination and blood perfusion restoration in large intestine after surgery. There was a general edematous syndrome with fluid retention in the tissues in children with CLIO before surgery. That was the reason for the pathological weight gain in 12 neonates in this group, that causes “imaginary lack of weight” in 19 neonates with CLIO. Let's note, that water and electrolytes metabolism are crucial for the intestine functioning in newborns with CIO [20].Before surgery the metabolic component of the endogenous intoxication - malondialdehyde, as well as protein-energy, water-electrolyte disorders and weight loss were more evident at newborns with high congenital intestinal obstruction. In spite of this, regression of endogenous intoxication after surgery was faster in this patients with high intestinal obstruction versus newborns with low intestinal obstruction. Probably, low CIO, accompanied by a high level of endogenous and bacterial toxins, bilirubin contributes to more evident impaired adaptation of newborns, which affects the postoperative recovery. The decrease of bilirubin (total fraction) on the tenth day after the surgery may be explained by neonatal jaundice reduction, which was slow and disappears by the end of the first month of life. Jaundice was prolonged in newborns with CIO, because the level of total bilirubin was higher versus to the control (p<0,05) measured at 10 day after birth.Thus, EI in newborns wit CIO is developed as a result of unbalancing the links between production and detoxification of endogenous and exogenous toxic products. EI has both common and distinctive features, depending on the level of intestinal obstruction - high or low CIO. EI is an integral part of a critical state of organism of newborn with CIO, it is developed due to the failure of the main components of detoxification systems of the organism, that causes disturbances of ability to utilize and eliminate both the products of normal and impaired metabolism, and also microorganism toxins. Identified disturbances require appropriate corrective therapy at the stages of preoperative preparation and postoperative management of newborns with CIO.
4. Conclusions
Congenital intestinal obstruction in newborns is accompanied by endogenous intoxication, which is reliably confirmed by high levels of MMP. CIO in newborns is accompanied by EI of mixed genesis with a predominance of metabolic and resorption components. High level of MDA, as a result of hypoxia, membrane destruction and tissue necrosis is a distinctive feature of CHIO and malrotation. High level of MMP, bilirubin, as a result of resorption of endogenous and exogenous toxins is a feature of CLIO in newborns.The retention component of endogenous intoxication at CIO is weakly expressed because creatinine levels did not change statistically significantly from the control.MMP level increase was more expressed at newborns with low congenital intestinal obstruction. The resorption component of endogenous intoxication at congenital intestinal obstruction was increased due to bilirubin, it was significantly higher at newborns with low congenital intestinal obstruction versus patients with high congenital intestinal obstruction. Before surgery the metabolic component of the endogenous intoxication - malondialdehyde, as well as protein-energy, water-electrolyte disorders and weight loss were more evident at newborns with high congenital intestinal obstruction. In spite of this, regression of endogenous intoxication after surgery was faster in this patients with high intestinal obstruction versus newborns with low intestinal obstruction. After surgery regression of MDA level was faster in patients with high intestinal obstruction versus newborns with low intestinal obstruction, that had significantly high level of MMP.
References
| [1] | Isakov Yu. F., Razumovsky A. Yu. In the book: Surgery of the newborn. Children's surgery. - Moscow: “GEOTAR-Media”, 2014. - P. 369-391. |
| [2] | Nemilova T.K., Karavaeva S.A., Mokrushina O.G. Congenital intestinal obstruction. In the book:. Pediatric Surgery: National Guide / Ed. Yu.F. Isakova, A.F. Dronova. - M: “GEOTAR - Media”, 2009, - P. 325-334. |
| [3] | Samuel D. Smith Malrotation // Ashcraft’s pediatric surgery. sixth edition. George W. Holcomb, J. Patrick Murphy, Daniel J. Ostlie, London New York Oxford Philadelphia St Louis Sydney Toronto 2014. – P. 430-438. |
| [4] | Ergashev N.Sh., Sattarov Zh.B. Diagnosis and treatment of congenital intestinal obstruction in newborns // "Modern Medicine: Topical Issues": a collection of articles based on the materials of the XXV International Scientific and Practical Conference, Novosibirsk:, SibAK - 2013. –№11 (25). - P.58-65. |
| [5] | Derunova V. I., Galkina Ya. A., Mokrushina O. G., Geraskin A. B. Long-term results of surgical treatment of duodenal obstruction in newborns // Pediatric Surgery. - Moscow, 2011. –№5. - P. 25-28. |
| [6] | Ergashev N. Sh., Sattarov J.B. The сlinical-anatomic characteristic of intestinal rotation and fixation anomalies in children // «European Applied Sciences» – Germany, 2013. – №9. Volume 1. – P. 34-38. |
| [7] | Touloukian R. J. Atresia and stenosis of the intestine. In: Pediatric Surgery, ed. Ashcraft K.U., Holder T.M. - St. Petersburg, Harford, 1996. -- Volume 1. - P. 341-356. |
| [8] | Volodin N.N. Neonatology: National leadership: “GEOTAR - Media”, 2017. - P. 845. |
| [9] | Groff D. Malrotation. In: Pediatric Surgery / Ed. C.W. Ashcraft and T.M. Holder. Translation from English T.K. Nemilova. - St. Petersburg: "Pete-Tal", 1997. - Volume 1. - P. 357-365. |
| [10] | Akhmedova D.I., Akramova H.A., Khaibullina Z.R. Anemia and oxidative stress in the blood as disadaptation factors in low birth weight infants on the first day of life // Pediatrics, Tashkent 2016. -№1. - P. 110-114. |
| [11] | Erkenova M.N., Murzakhmetova M.K., Aralbaeva A.N. The study of antimicrobial and antioxidant properties of plant extracts // Student: electron. scientific journal 2017. No. 1 (1). URL: https://sibac.info journal student 1/70626. |
| [12] | Methodological problems of the rehabilitation of premature babies: scientific publication / L. L. Pankratieva, N. N. Volodin // Pediatrics. G.N. Speransky Journal: Scientific and Practical Medical Journal / Union of Pediatricians of Russia. - Moscow: LLC "Pediatrics". - 2019. -- Volume 98 N 2. - P. 14-18. |
| [13] | Khaibullina Z.R. Oxidative stress and the possibilities of antioxidant therapy (review) // Infection, immunity, pharmacology, 2014. -№1. - P. 82-92. |
| [14] | Ohkawa H, Ohishi N, Tagi K. Assay for lipid peroxides in animal tissues by thiobarbituric acid reaction // Anal Biochem. 1979; 95: 351-358. |
| [15] | Gabrielyan N.I., Levitsky E.R., Dmitriev A.A. Screening method for determination of medium molecules in biological fluids //Methodical recommendations, M.: BI, 1985. - P. 3-6, 9-18. |
| [16] | Morrison V.V., Chesnokova N.P., Bizenkova M.N. Acid-base condition. Typical violations of the acid-base state (lecture 2) // International Journal of Applied and Basic Research. - 2015. - No. 3-2. - P. 273-278; |
| [17] | Shabalov N.P. Neonatology: Textbook. allowance: T. I. 3rd ed., - M.: MEDprssss-nnform, 2004. - P.154-221. |
| [18] | Vinocur D. N., Lee E. Y., Eisenberg R. L. Neonatal Intestinal Obstruction // AJR (Boston). – 2012. – Vol.198. – P. 1-10. |
| [19] | Pablo Aguayo, Daniel J. Ostlie Duodenal and Intestinal Atresia and Stenosis// Ashcraft’s pediatric surgery. sixth edition. George W. Holcomb, J. Patrick Murphy, Daniel J. Ostlie, London New York Oxford Philadelphia St Louis Sydney Toronto 2014. – P.414-429. |
| [20] | Ergashev N. Sh., Sattarov J.B. Surgical tactics for intestinal malrotation in children // European Medical, Health and Pharmaceutical Journal. – Czech Republic, 2015. – Volume 8. Issue. 1. – P.1-4. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML