-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2020; 10(6): 378-383
doi:10.5923/j.ajmms.20201006.06

Comparative Evaluation of the Nearest Results of Treatment of Sigmoid Volvulus in Elderly
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLD. M. Khakimov, M. M. Nosirov
Andijan State Medical Institute, Andijan, Uzbekistan
Correspondence to: M. M. Nosirov, Andijan State Medical Institute, Andijan, Uzbekistan.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

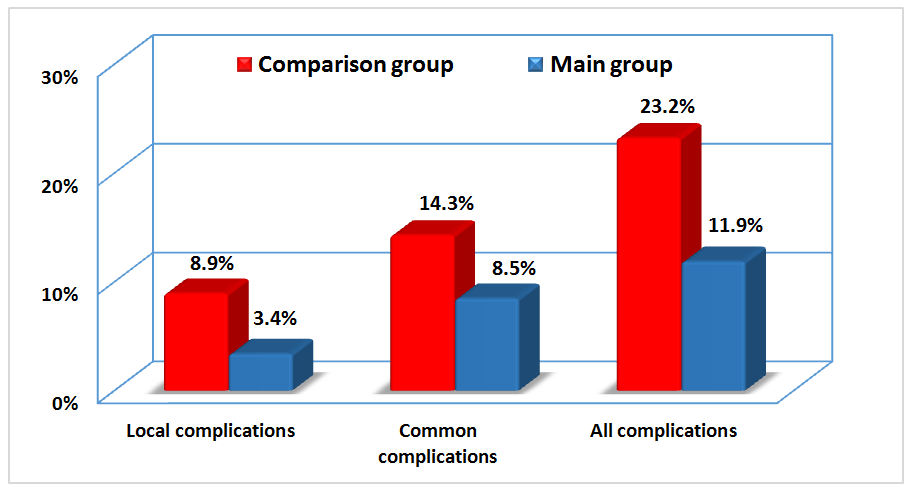
The aim of the research work is - in a comparative aspect, to study the nearest results of treatment of sigmoid volvulus in elderly. Materials. The authors studied nearest results of treatment of sigmoid volvulus in 122 elderly patients. Methods. Comparative analysis of coming results of the non-operative and surgical treatment. Conclusion. Improving the tactical aspects of choosing the optimal type of treatment for SV in the elderly has reduced the risk of ineffective conservative therapy from 10.3% to 3.1%, reduced the share of reassessment of indications for resection interventions from 8.6% to 6.3%, and reduced the frequency of palliative interventions with the possibility of radical surgery from 22.4% to 3.1%, which generally led to an increase in the rate of the right tactics from 58.6% to 87.5%, reduce the incidence of specific complications from 35.7% to 15.3%, general complications from 19.6% to 10.2% and mortality from 22.4% to 10.9%.
Keywords: Sigmoid volvulus, Surgical treatment, Nearest results
Cite this paper: D. M. Khakimov, M. M. Nosirov, Comparative Evaluation of the Nearest Results of Treatment of Sigmoid Volvulus in Elderly, American Journal of Medicine and Medical Sciences, Vol. 10 No. 6, 2020, pp. 378-383. doi: 10.5923/j.ajmms.20201006.06.
1. Introduction
- The sigmoid volvulus (SV) in urgent surgery is still one of the most serious diseases of the abdominal organs [1-3]. To date, aspects of surgical epidemiology and clinical features in various regions of the world with large intestine inversions are well covered in the literature, according to which, for example, SV is often found in people of mature and old age (average age - 65 years), and blind inversion gut develops at a younger age. The average age of occurrence is 50 years. In some regions, for example, in India, the average age of the onset of the disease is 33 years. In different age groups and different regions, the sex ratio is different. According to averaged estimates, men predominate, but cecum inversion is much more common in women [2-7].Today, cases of such patients being admitted to clinics are not uncommon, clinicians have sufficient experience, however, mortality in this disease reaches 11.5–40% or more [4-8], the number of complications of the early postoperative period, in general, is 8-32% and do not tend to reduce their frequency [9-12].In our region, the occurrence of SV and the features of its clinical course with verification of risk factors for an adverse outcome have not yet been studied.Aim of study is - in a comparative aspect, to study the nearest results of treatment of sigmoid volvulus in elderly.
2. Materials and Methods
- In order to objectively evaluate the results of optimization of the tactics of surgical treatment of patients with advanced cardiovascular diseases, we performed a comparative analysis between the groups, conditionally divided into the main group, which included 64 patients who were admitted to the surgical hospital from 2009 to 2018 (treatment was carried out in the aspect of tactical optimization approaches) and a comparison group, which included 58 patients admitted with SV in the period 2000 to 2008 (the treatment of which was carried out in accordance with the surgical tactics adopted at that time).The evaluation of the results of treatment of patients in the compared groups was carried out after the distribution of patients according to the final type of treatment, which is presented in the diagram Figure 1.
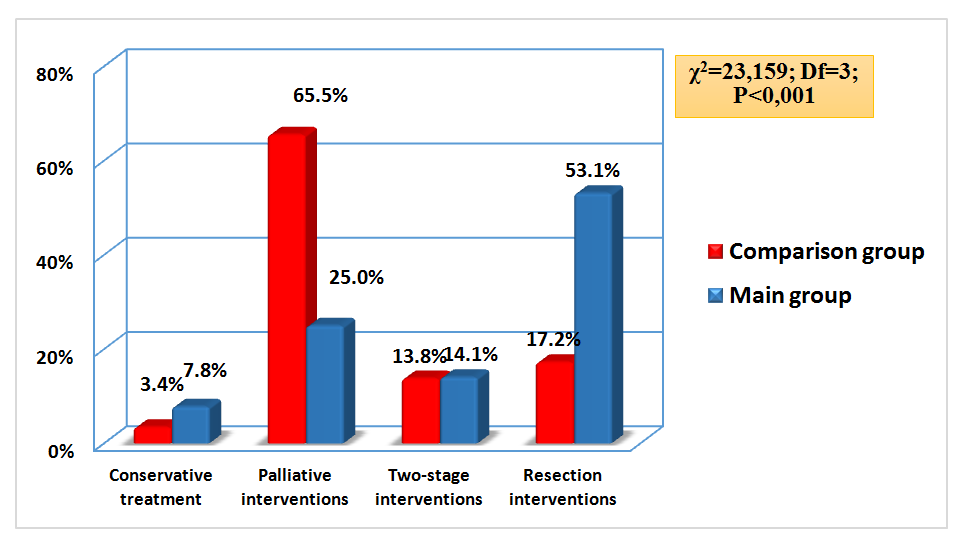 | Figure 1. The distribution of patients by the final type of treatment |
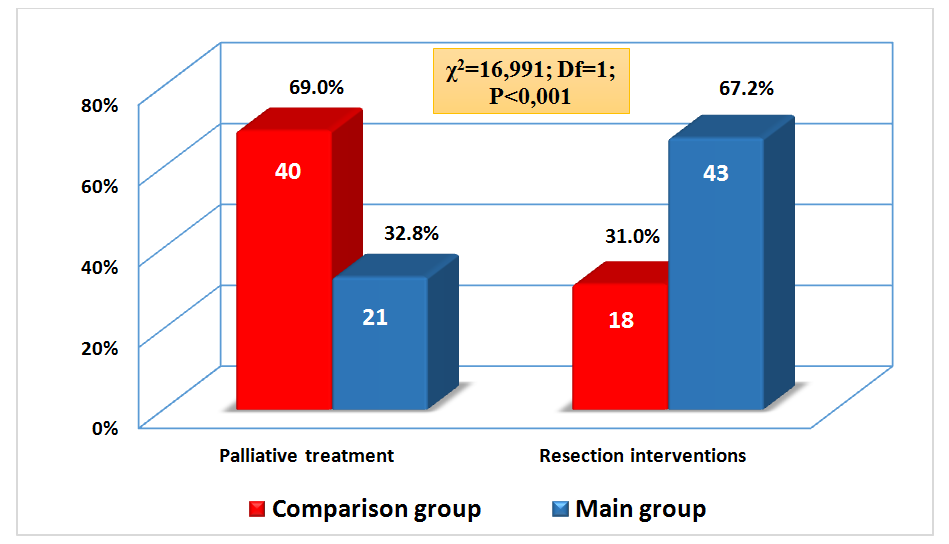 | Figure 2. The distribution of patients by the final type of treatment |
3. Results
- A detailed study of adverse outcomes and factors contributing to them in the near postoperative period allowed us to identify the main tactical shortcomings in the choice of treatment for SV, which are presented in the diagram Figure 3. Thus, ineffective conservative therapy occurred in 6 (10.3%) patients from the comparison group and in 2 (3.1%) patients from the main group. Reassessment of indications for sigmoid colon resection (SCR) was almost identical in both groups: in 5 (8.6%) patients from the comparison group and in 4 (6.3%) from the main group. The possibility of performing one-stage surgical treatment was noted in 13 (22.4%) patients from the comparison group and only 2 (3.1%) patients from the main group. The correct tactics were evaluated by us in 34 (58.6%) patients in the comparison group and in 56 (87.5%) patients in the main group (χ2 = 15.297; Df = 3; P = 0.002).
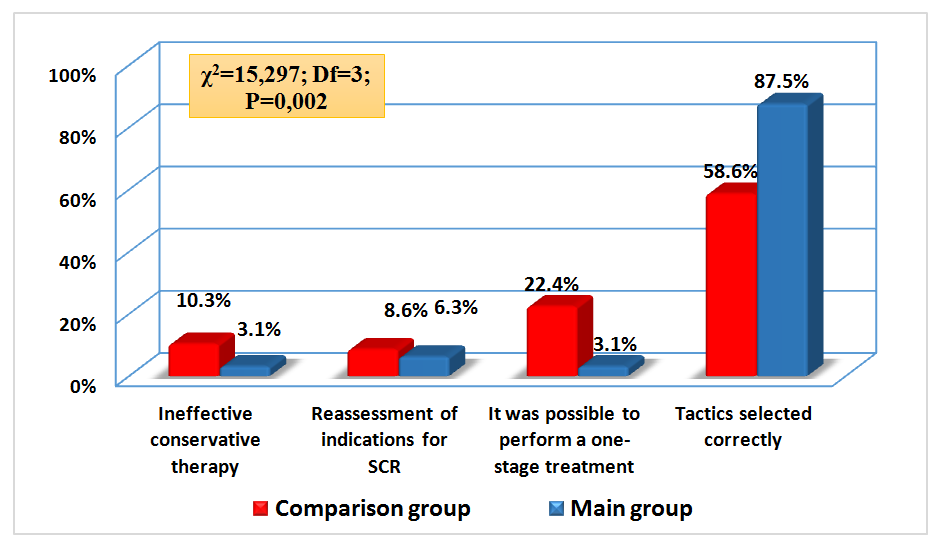 | Figure 3. Tactical flaws in choosing a method for the treatment of SV |
 | Figure 4. Tactical flaws in choosing a method for the treatment of sigmoid volvulus |
|
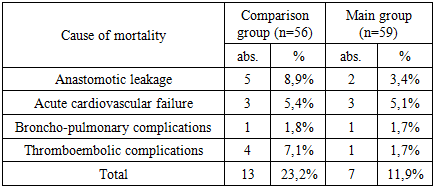
 | Figure 5. Mortality rate depending on the nature of postoperative complications |
|
4. Discussion
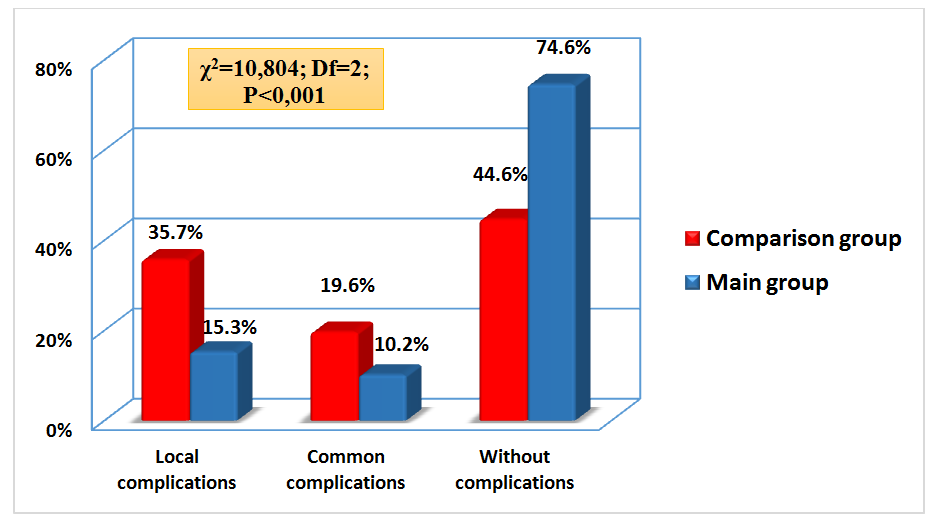
- The summary immediate results of the selected treatment tactics in the compared groups are presented in the diagram Figure 6. So, the total number of patients discharged without complication was 27 (46.6%) from the comparison group and 49 (76.6%) from the main group. Discharged after correction of complications: 18 (31.0%) from the comparison group and 8 (12.5%) from the main group.
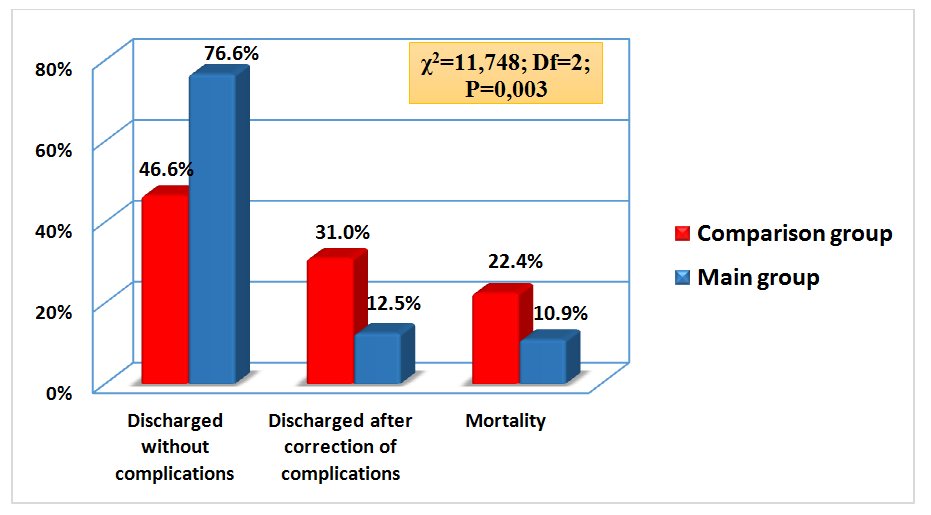 | Figure 6. Consolidated immediate results of conservative and surgical treatment of sigmoid volvulus in the elderly |
5. Conclusions
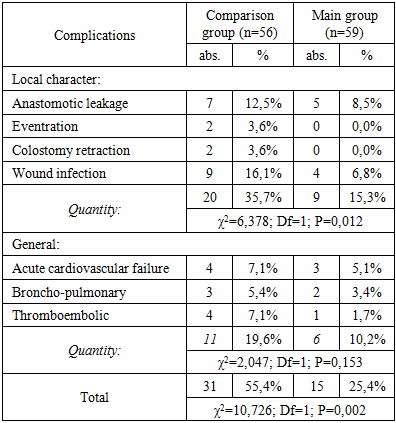
- The studies conducted allowed us to draw the following conclusions: Improving the tactical aspects of choosing the optimal type of treatment for SV in the elderly made it possible to reduce the risk of ineffective conservative therapy, reduce the share of reassessment of indications for resection interventions, and reduce the frequency of palliative interventions when radical surgery is possible (resection of the sigmoid colon), which generally led to an increase in the rate of the right tactic.The developed algorithm for choosing the optimal tactics for the management of elderly patients with SV, as well as improving the technical aspects of performing resection interventions, reduced the frequency of complications in the coming period from 53.4% (in 31 of 58 patients in the comparison group) to 23.4% (in 15 of 64 patients in the main group) (χ2 = 11.667; Df = 1; P <0.001).