Kadirov Rustam Nadirovich1, Khadjibaev Farhod Abdukhakimovich2, Akhmedov Yusuf Makhmudovich1
1Samarkand State Medical Institute, Samarkand, Uzbekistan
2Rebulican Research Centre of Emergency Medicine, Tashkent, Uzbekistan
Correspondence to: Kadirov Rustam Nadirovich, Samarkand State Medical Institute, Samarkand, Uzbekistan.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Introduction. The most common and formidable complications of portal hypertension are bleeding from varicose veins of the esophagus and stomach, a radical method of treatment and prevention of which at present can only be considered liver transplantation. All other technologies (conservative, endoscopic, endovascular, surgical) are palliative measures, the most important task of which is to ensure for the patient the highest possible quality of life in the inter-relapse period. The purpose of this study: a comparative assessment of the quality of life of patients in the early period after emergency treatment of active bleeding from ARVI using endoscopic hemostasis technologies and through the operation of azigo-portal separation according to M.D. Patients. The research method was a survey of 338 patients and 146 healthy people using the non-specific MOS SF-36 questionnaire, to quantify such aspects of quality of life as physical, role and social functioning, the impact on the quality of life of pain, the state of physical and mental health. Results. In the early period after the relief of active bleeding from varicose veins of the esophagus and gastric veins by means of endoscopic ligation and / or sclerotherapy, a higher level of QOL was recorded compared to that after surgical treatment according to M.D. Patients. Conclusion. When stopping gastroesophageal bleeding associated with portal hypertension and varicose veins of the esophagus and stomach, one of the advantages of endoscopic hemostasis over surgical treatment by the method of M.D. Patients is a better quality of life for patients in the early period after the intervention.
Keywords:
Quality of life, Questionnaire SF-36, Bleeding from varicose veins of the esophagus and stomach portal hypertension
Cite this paper: Kadirov Rustam Nadirovich, Khadjibaev Farhod Abdukhakimovich, Akhmedov Yusuf Makhmudovich, Quality of Life of Patients in the Coming Period after Purposing of Gastroesophageal Bleeding, Depending on the Applied Hemostasis Methods, American Journal of Medicine and Medical Sciences, Vol. 10 No. 5, 2020, pp. 344-350. doi: 10.5923/j.ajmms.20201005.14.
1. Introduction
Gastroesophageal bleeding (GEC) from varicose veins of the esophagus and stomach (VVES) are the most dangerous and most frequent complications of portal hypertension (PG), registered, according to many authors, no less than in ⅓ patients with PG and the presence of varicose veins of the esophagus and stomach, and becoming a cause of death for these individuals in 14.5-90% of cases [2,6]. The incidence of HEC from varicose esophageal and gastric veins in all countries of the world increases year by year in proportion to the increase in the incidence of liver cirrhosis [5], associated with an avalanche of increasing alcohol abuse, with an increase in uncontrolled and unsystematic use of drugs, with an increase in the incidence of viral hepatitis [4,7]. It should also be noted that at present, for a number of regions, including those in Central Asia, there is a very persistent trend towards the emergence and development of CP, PG, and HEC in young people-no older than 20-25 years [1,8].Unfortunately, in the Arsenal of modern medicine, there is only one technology for radical treatment of the entire complex of disorders in the chain "cirrhosis of the liver → portal hypertension → gastroesophageal bleeding" - liver transplantation. All other methods (conservative, endoscopic, endovascular, more than 200 surgical techniques) are essentially in the category of palliative measures [2]. Typical for the present time problematic issues of liver transplantation - acute shortage of donor organs (including by reducing injuries and mortality) [7], features of the formation of the waiting list (priority of providing transplant care to individuals with end-stage functional liver disorders) [5], "... absence or stage of introduction of radical treatment in many countries of the world ...» [5] and others-dictate the dominance of palliative treatment of patients with cirrhosis of the liver and PG, complicated by bleeding from varicose esophageal and gastric veins. One of the most important criteria for the effectiveness of palliative treatment is the quality of life (QL) [6]. The purpose of these studies was to compare the quality of life of patients in the early period after emergency treatment of active bleeding from the varicose veins of the esophagus using endoscopic hemostasis technologies and through the operation of azigo-portal separation by the method of MD Patients.
2. Research Materials and Methods
The work was performed on the bases of surgical and intensive care units of the Samarkand branch of the Republican scientific center of emergency medical aid and the Republican scientific center of emergency medicine in the period from January 2014 to November 2018 participated In the study voluntary participation 338 (265 men and 73 women) aged from 20 to 50 years, for the first time after bleeding from varicose veins of the esophagus and stomach, resulting in conditions of syndrome of portal hypertension and liver cirrhosis. Depending on the nature of treatment measures, all participants were divided into the main group №1 (n=162) and the comparison group №2 (n=176). Each of the patients was diagnosed with EGDS within 60-90 minutes after admission, standard medical treatment was performed, including infusion and blood transfusion therapy, as well as the use of drugs with hemostatic and hepatoprotective type of action. In addition, endoscopic ligation (EL) and/or endoscopic sclerotherapy (ES) of problematic veins were performed to stop bleeding in group 1.patients from group 2 underwent azigo-portal dissociation surgery using the method of M.D. Paziora after preliminary relief of bleeding by installing a Sengastaken-Blackmore obturator probe.The quality of life was evaluated before the start of treatment and on the third day after it, taking into account the gender and age of patients, i.e., separately for men and women in the age categories 20-25, 26-30, 31-40, 41-45 and 46-50 years. The obtained data were compared with each other, and also correlated with the results of similar measurements in practically healthy people (n=146) who voluntarily agreed to answer the questionnaire questions and joined the control group No. 3.A non-specific questionnaire MOS SF – 36 (Medical Outcomes Study-Short Form-36), i.e. a short form MOS (General health questionnaire) consisting of 36 questions, was used to analyze QL. When filling out the questionnaire, the respondents chose one of several suggested answers that was most appropriate for them. Interviewing allowed us to quantify the following indicators of the participants ' overall health: 1) physical functioning (PF, the ability to tolerate both normal and increased physical activity); 2) role-based functioning due to physical condition (RP, reflects the influence of physical condition on the performance of their duties at home and at work); 3) the intensity of pain (BP); 4) General health (GH, personal opinion of the Respondent); 5) vital activity (VT, self-awareness of cheerfulness/fatigue, energy/exhaustion); 6) social functioning (SF, level of interest and productivity when communicating with family, colleagues, friends, etc.); 7) role-based functioning due to emotional state (RE); 8) self-assessment of one's own psychological health (MN, severity of feelings of happiness/sadness, calmness/nervousness). Calculation of PF, RP, BP, GH, VT, SF, RE, and MN indicators was performed according to the author's guide to the use of SF-36®V. 2, compiled by J. E. Ware et al. (2000) - the developers of SF-36: 1) within each of the scales summed up the "raw questionnaire scores" [CIT. by J. E. Ware et al.. 2000], i.e., the points that were used to evaluate a particular response option selected by the Respondent; 2) for each of the scales, the sum of the unprocessed questionnaire points was transformed into the sum of QA points using a special author's formula: where,
where,  is the sum of the raw scale points; Min is the minimum possible scale value; Max is the maximum possible scale value [Ware J. E. et al., 2000]. When interpreting the calculated transformed quality of life indicators for each of the scales, we were guided by the following instructions of the author's guide to the use of SF-36®V. 2: "... in the complete absence of restrictions or health disorders, the maximum value is 100, the higher the indicator for each scale, the better the quality of life for this parameter ... " [CIT. by J. E. Ware et al.. 2000].
is the sum of the raw scale points; Min is the minimum possible scale value; Max is the maximum possible scale value [Ware J. E. et al., 2000]. When interpreting the calculated transformed quality of life indicators for each of the scales, we were guided by the following instructions of the author's guide to the use of SF-36®V. 2: "... in the complete absence of restrictions or health disorders, the maximum value is 100, the higher the indicator for each scale, the better the quality of life for this parameter ... " [CIT. by J. E. Ware et al.. 2000].
3. Results and Discussion
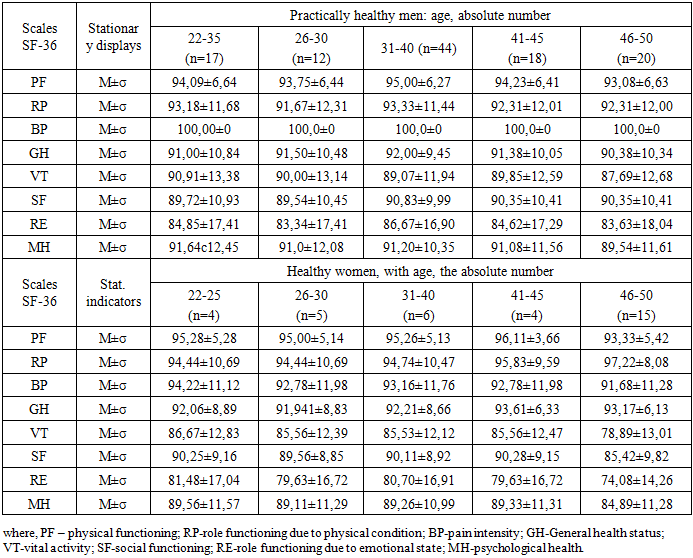
During the survey, all practically healthy respondents in control group 3 rated their health as "Very good" or "Excellent", and noted that there were no problems associated with physical and psycho-emotional state, when performing household and official duties, and communicating with other people. Each of the participants in the control group chose such answers that indicated a positive emotional mood, complete absence of any pain and anxiety about the state of their health in the future. As can be seen from table 1, in practically healthy people of different ages, each of the calculated indicators of QL always aspired to 100, which confirmed the complete satisfaction of the respondents of control group 3 in various spheres of life, the harmony of their physical, psychological, emotional and social functioning.Table 1. Quality of life for practically healthy men and women of different ages
 |
| |
|
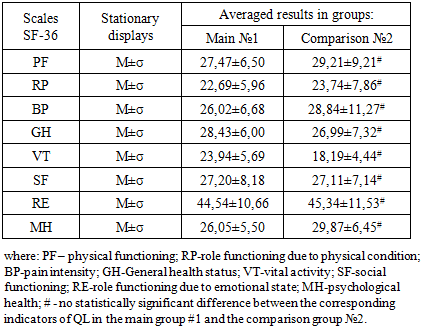
All participants in the study of the main group №1 and the comparison group #2 complained of nausea, vomiting of blood, black stools, and dizziness upon admission to treatment, bothering them within 24-72 hours before seeking medical care or within 4-8 days before hospitalization (85% and 15% of cases, respectively). The General condition was assessed as severe in 75% of patients, moderate and extremely severe in 21% and 4% of patients, respectively. Almost half of the patients had signs of hemorrhagic shock of I-II degree, the rest-the volume of blood loss varied from 250 ml to 800 ml, all without exception had severe post-hemorrhagic anemia, in 68% of cases ascites of various severity were observed.Taking into account on the one hand the impossibility of conducting a questionnaire at the time of hospitalization, and on the other - the need to obtain data on the level of QL before treatment, we asked patients of groups 1 and 2, already treated and preparing for discharge, to retrospectively give a self-assessment of their condition when entering treatment, answering questions SF-36. When processing completed questionnaires, it was found that there were no statistically significant differences between the indicators of QOL (PF, RP, BP, GH, VT, SF, RE, MH) in people of different gender and age. Below, in table 2, we present the average results of calculating PF, RP, BP, GH, VT, SF, RE, MH for all participants in groups 1 and 2, regardless of age and gender.Table 2. Calculated values of QL before the start of treatment of bleeding from varicose veins of the esophagus and stomach in portal hypertension syndrome before the start of treatment
 |
| |
|
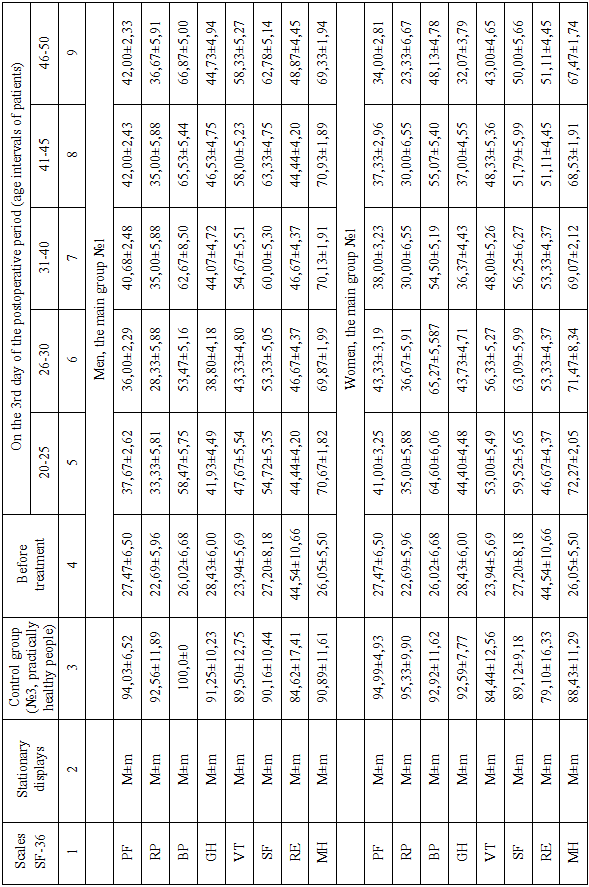
According to the data published in table 2, the period that lasted from the beginning of deterioration to the beginning of treatment measures was characterized by a decrease in all calculated indicators of QL. A more than six-fold decrease in physical functioning capabilities (PF scale) was accompanied by a pronounced depression of the psycho-emotional state and life activity. The patients 'responses to questions on the VT, RE, and MH scales reflected the prevailing feelings of depression, sadness, fatigue, and exhaustion in patients, a decrease in motivation to communicate with other people, and also indicated the patients' confidence in the extremely low quality of their own health ("bad" or "mediocre") and its mandatory deterioration in the future.The results of determining the calculated values of QL in patients after treatment are presented in table 3. In 20-25-year-old men of the main group №1, three days after ES and / or EL, the first signs of a tendency to increase the level of QL appeared. Among them, the most noticeable was a positive change in the psycho-emotional state of patients (MH scale): when answering the question " What feelings most correspond to Your mood now? "respondents often chose versions that indicate the prevailing feelings of peace, tranquility, and happiness. In accordance with this, the calculated MH indicators have increased almost threefold compared to those before the start of treatment measures. There was also a 1.5-2-fold increase in PF, RP, and SF values, which did not exceed 25-30% of the PF, RP, and SF levels in healthy people before admission to the hospital. Self-assessment of pain intensity was 58.47±5.75 versus 26.02±6.68 when seeking medical care. Table 3. Quality of life for voluntary study participants
 |
| |
|
Continuation of the table 3
 |
| |
|
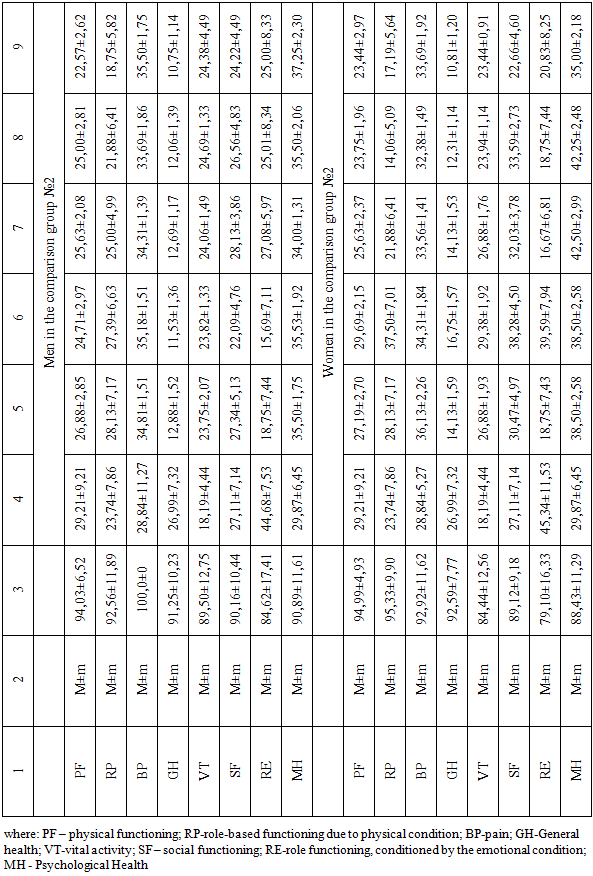
In 20-25-year-old participants from group # 2 three days after the operation, azigo-portal separation by the method of M.D. Patsiora: first, the estimated levels of physical functioning associated with the physical condition and social functioning (PF and SF scales, respectively) remained very low and was not significantly different from those before surgery (p>0.05); second, more than half in relation to the preoperative value decreased values of role functioning, conditioned by emotional state scale (RE) and self-assessment of the General health scale (GH) (p<0.05). Positive dynamics, although less pronounced than in patients from group 1, were observed in relation to QL criteria such as pain intensity (BP), role functioning associated with physical condition (RP), vital activity (VT), and psychological health (MH).In General, the use of endoscopic ligation and/or sclerotherapy technologies for the treatment of first-time HEC from varicose veins of the esophagus and stomach in male patients aged 20-25 years provided a higher quality of life in the early postoperative period than in cases with surgical treatment of the conditions under consideration by the method of MD Patients. Study participants in group 1 felt calmer, more confident, more cheerful, than patients from the comparison group, actively interacted with roommates and separation, family and friends very much interested in various events in his own family, in the surrounding society, the world, etc. in contrast, patients who had undergone surgery were less likely to communicate with other people, often feel fatigue and depression, were more often evaluated their health as "mediocre" or "bad" and its expected deterioration in the future (table. 3). Similar results were obtained for 20-25-year-old women from the main group №1 and from the comparison group #2, as well as for 26-30-year-old male and female patients from groups № 1 and № 2.In 31-40-year-old men of the main group №1, whose treatment regimen included the use of endoscopic hemostasis methods, in the early postoperative period, the calculated values of PF, RP, BP, and SF were 40,68±2,48, 35,00±5,88, 62,67±8,50 and 60.00±5.30, respectively (when hospitalized 27,47±6,50, 22,69±5,96, 26,02±6,68 and 27.20±8.18), which indicated the appearance of a statistically significant trend to reduce the impact of physical condition and pain caused by the disease on physical activity, daily activities (albeit limited at the time of stay in a medical institution), and communication with other people. These respondents as "often began to feel vigorous, full of strength and energy", "never felt depressed or fallen spirit (after treatment)", "my health is now much better than before treatment", "mostly untrue, that my health to deteriorate" confirmed the increase of vitality, a boost in self-esteem your health, both General and mental, hence a statistically significant increase in 2-5 times indicators VT, GH, MH to 54,67±5,51, 44,07±4,72, 70,13±1,91 ( (p<0.05) (table. 3). In men aged 20-25 and 26-30 years from group 1, 3-5 days after endoscopic intervention, there was a similar, but less pronounced dynamics: all indicators of SF-36 exceeded those before treatment by 1.5-2.0 times, however, they were 5-13% lower than the calculated results in 31-40-year-old participants of the main group 1.In comparison group №2, men aged 31-40 years, when interviewed 3-5 days after emergency surgical treatment of bleeding from the ERW, noted that the current physical and emotional state created very significant difficulties when performing even the simplest physical actions, defined in SF-36 as "lifting or carrying a bag of food", "bending over", "washing themselves, dressing themselves", etc. According to the test results, in the early postoperative period, patients rarely felt calm, cheerful and full of energy, extremely low assessment of their level of health and expected it further deterioration. This is probably why the values of PF, GH, and RE were reduced by 12.26-53.24% (p<0.05) compared to those before surgery, while the calculated indicators of vital activity (VT) and daily role activity remained statistically significant at the preoperative level. In men 20-25 and 26-30 years of age from group 1, higher results of SF-36 testing were obtained.When comparing the calculated SF-36 indicators in 20-25-, 26-30 - and 31-40-year-old participants of group 2, it was found that in the early period after asigo-portal separation by the method of MD Patients, firstly, the values of PF, RP, BP, GH, VT and MH, while remaining very low, did not have statistically significant differences among themselves; secondly, men aged 31-40 years, despite the existence of physical and emotional problems in their daily activities, demonstrated a higher level of social activity (table. 3).In women aged 31-40 years, in the early period after emergency treatment of first-time bleeding from varicose veins of the esophagus and stomach, the features of changes in QL indicators were, in General, similar to those observed in 31-40-year-old men. After 3-5 days after EL and / or ES, 41-45-year-old male and female study participants from group 1 increased SF-36 values by 20-60% relative to the data at the time of hospitalization. At the same time, the GH and RE values of men of the considered age group No. 2 were 12.06±1.39 and 25.01±8.34, which was about 2 times less than the results of preoperative measurements, and 3.5 times less than the results of control measurements. PF, RP, and SF also decreased by 14.4%, 7.8%, and 2%, respectively, relative to those before the intervention. BP, VT, and MH values increased to 33.69±1.86, 24.69±1.33, and 35.50±2.06 (when received, 28.84±5.27, 18.19±4.44, and 29.87±6.45, respectively, p<0.05). The same changes in the studied parameters of QL occurred in 41-45-year-old women operated on by the method of MD Patients.At the time of hospitalization, all 46-50-year-old study participants (men and women) had physical, role, and social functioning opportunities due to their physical and emotional state (PF, RP, SF, and RE) reduced by 1.7 – 4.3 times compared to the control values (p<0.05), levels of freedom from the influence of pain on daily activities (BP)-by 3.5 – 3.8 times (p<0.05), life activity (VT)-3.1 – 4.8 times (p<0.05), and self-esteem of their state and prospects of treatment (GH) - 3.2-3.4 times (p<0.05), psychological well-being (mn) - 3.0-3.6 times (p<0.05). In the first 3-5 days after ES and/or EL, 46-50-year-old men from the main group №1 had a statistically significant increase in the numerical characteristics of each of the scales by about 35-60% from the results of preoperative measurements, however, at this stage, all indicators remained below the control values by 30-60% (p<0.05). In group 1 patients (men and women) aged 22-25, 26-30, 31-40, and 40-45, the results of the survey were comparable.In 46-50-year-old men and women who underwent M. D. surgery, positive dynamics was registered only for BP, VT, and MH indicators at 3-5 days after the intervention, the values of which increased by 18.8%, 25.4%, and 19.8% in relation to the results of preoperative measurements (p<00.05). In contrast, the levels of physical, role, and social functioning that depend on physical and emotional state (PF, RP, SF, and RE), as well as self-assessment of their health and treatment effectiveness (GH), decreased by a factor of 1.9-3.9 upon admission to treatment (p<00.05), further decreased to 22.57±2.62. 18,75±5,82, 24,22±4,49, 25,00±8,33 and 10.75±1.14, respectively (p<00.05).
4. Conclusions
The quality of life of patients in the immediate period after stopping the first bleeding from varicose veins of the esophagus and stomach differed depending on the methods used to stop bleeding. In cases using endoscopic ligation and / or sclerotherapy, a higher level of QL was recorded (determined using the SF-36 questionnaire) than after surgical treatment using the M.D. Patient method. In General, the calculated values of all SF-36 indicators in men and women aged 20 to 50 years who underwent surgery were 1.02-4.16 times statistically significantly lower than those in individuals treated with endoscopic techniques. In essence, this means that the use of endoscopic ligation and / or sclerotherapy in the next few days after stopping the bleeding provides significantly greater opportunities to perform physical actions (even the simplest ones, those that are required when staying in a hospital) without the need for additional effort, reducing the time spent on this or that work, reducing its volume. After endoscopic treatment, patients quickly and easily return to life in society, are more optimistic when assessing their health in the future, their psycho-emotional background is more unpleasant and stable compared to that of patients from the comparison group. Also, the analysis of test results SF-36 after endoscopic and surgical stop gastro-esophageal bleeding from Writer was established, first, the lack of statistically significant differences between parameters of SF-36 in men and women of certain age categories within each of the groups; secondly, there is a difference between postoperative QOL in patients aged 20-25, 26-30, 31-40, 41-45 and 46-50 years. In each of the compared groups, we observed better test results in 31-45-year-old men and women, and lower results in those aged 20-30 and 46-50 years.
References
| [1] | Galperin E. I., Dyuzheva T. G. Lectures on hepato-pancreato-biliary surgery. Moscow: Vidar, 2011. - 536 p. |
| [2] | Gadzhiev Ogly K. A. Therapeutic tactics for liver cirrhosis complicated by portal Garbuzenko D. V. Methods for predicting risk and monitoring the effectiveness of therapy for bleeding from esophageal varicose veins in patients with liver cirrhosis // Gastroenterology. Hepatology. - 2010. - No. 6. - Pp. 11-20. |
| [3] | Gauthier S. V. liver Transplantation in Russia: 25-year experience and modern possibilities / S. V. Gauthier / / Bulletin of Transplantology and artificial organs. - 2015. - No. 2. - Pp. 93-95. |
| [4] | Gulyaev V. A. Improving the effectiveness of liver transplantation by improving the technology of removal and preparation of the transplant: Dis. ... d-RA. honey. Sciences: 14.01.24 / Gulyaev, Vladimir Alekseevich. - Moscow, 2015. - 307 p. |
| [5] | Davlatov S.S., Sherbekov U.A., Juraeva F.F., Yusupalieva K.B. Optimization of surgical treatment of varicose disease of lower extremities// Problems of modern science and education - 2017.- 26 (108), - C. 85-88. |
| [6] | Zatevakhin I. I., And Shipov, V. N., Huang H, etc. Implantation of stentgraft – future development transjugular intrahepatic portosystemic shunting (TIPS) / Kremlin medicine // Clin. West. - 2009. - Vol. 2. - Pp. 74-78. |
| [7] | Kamalov Yu. R., Lebezev V. M., Khovrin V. V., and others. Possibilities of three-dimensional reconstruction of computer-tomographic images in preoperative assessment of patients with portal hypertension syndrome / / Med. visualization. - 2013. - No. 3. - Pp. 132-133. |
| [8] | Kotiv B. N., Dzidzava I. I., Kashkin D. P., and others. Treatment and prevention of bleeding from varicose veins of the esophagus in patients with liver cirrhosis with portal hypertension syndrome / / Sovrem. technol. in the honey. - 2010. - No. 1-2. - Pp. 35-36. |
| [9] | Kotiv B. N., Dzidzava I. I., Soldatov S. A. Results of selective and partial portocaval shunting and prognostic factors of long-term survival in patients with liver cirrhosis / / Ann. hir. Hepatol. - 2015. - No. 2. - Pp. 46-58. |
| [10] | Yang L., Yuan L., Dong R. Two surgical procedures for esophagogastric variceal bleeding in patients with portal hypertension // World J. Gastroenterol. - 2013. - Vol. 19 (48). - Р. 9418–9424. |
| [11] | Ware J.Е., Snow К.К., Kosinski М., Gandek В. Sf-36 Health Survey. Manuel and Interpretation Guide, Lincoln,RI'. Quality Metric Incorporated, 2000. - 150 p. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML