-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2020; 10(5): 324-328
doi:10.5923/j.ajmms.20201005.10

Retention of Cardiopulmonary Resuscitation Skills after a Standard Training Programme of Some Nigerian University Students
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAdedamola Olutoyin Onyeaso1, Chukwudi Ochi Onyeaso2
1Senior Lecturer, Department of Human Kinetics and Health Education, Faculty of Education, University of Port Harcourt, Port Harcourt, Nigeria
2Professor of Orthodontics, Department of Child Dental Health, Faculty of Dentistry College of Health Sciences, University of Port Harcourt / University of Port Harcourt Teaching Hospital, Port Harcourt, Nigeria
Correspondence to: Adedamola Olutoyin Onyeaso, Senior Lecturer, Department of Human Kinetics and Health Education, Faculty of Education, University of Port Harcourt, Port Harcourt, Nigeria.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Introduction / Aim: Considering the known decline in CPR skills with time and the importance of adequate CPR skills in the provision of effective bystander CPR for victims of out-of-hospital cardiac arrest, knowledge of retained CPR skills after a period of training in CPR becomes useful for planning. This study aimed at ascertaining the level of retained CPR skills in a group of Nigerian University students 15 months after standard (conventional) CPR training. Materials and Methods: A quasi-experimental design was used with the initial cohort of seventy who had their first exposure to CPR training using the conventional method. Fifteen months later, sixty-five of them -50 (76.92%) females and 15 (23.08%) males with age range of 18 to 29 years and mean of 22.22 ± 2.64 (SD) had their CPR skills re-assessed by the same instructor based on a modified American Heart Association CPR Skills Evaluation Guide. The Statistical Package for Social Sciences (SPSS) was used to analyse the data. Descriptive statistics and student’s t-test were employed in the analysis with P-value set at .05. Results: In all, average of 61.85%of them retained CPR skills of 60% and above, considered good enough for effective bystander CPR provision. There were significant losses in their CPR skills involving the scene safety and call for help, rescue breaths, and cycle/min and placement of victim in correct recovery position domains (P < .001), but not in the chest compression skills (P > .05). Conclusion/Recommendation: Although some of the participants had significant losses in some of the CPR skills domains, they generally had good retained CPR skills for effective bystander CPR provision. More related studies are needed in the country as a way of increasing awareness and producing more potential bystander CPR providers in Nigeria.
Keywords: Standard (Conventional) CPR training, Retention, Nigerian students
Cite this paper: Adedamola Olutoyin Onyeaso, Chukwudi Ochi Onyeaso, Retention of Cardiopulmonary Resuscitation Skills after a Standard Training Programme of Some Nigerian University Students, American Journal of Medicine and Medical Sciences, Vol. 10 No. 5, 2020, pp. 324-328. doi: 10.5923/j.ajmms.20201005.10.
Article Outline
1. Introduction
- The roles of teachers in training school children as potential bystander cardiopulmonary resuscitation (CPR) providers as well as potential CPR providers themselves in schools and the larger societies have been documented [11-14]. For teachers to effectively carry out the Effective bystander cardiopulmonary resuscitation (CPR) can only be guaranteed if the trained potential providers are able to retain their skills for a reasonable period of time before re-training programmes. The public health burden of out-of-hospital cardiac arrest (OHCA) is global involving both the developed and developing nations of the world [1-7]. Awareness of bystander cardiopulmonary resuscitation in our environment is still poor and needs serious improvement [8]. Unlike the advanced and some developing economies around the globe, there are just few reports on the retention of bystander CPR skills in Nigeria [9-11]. In our determined advocacy for inclusion of teaching and training in bystander cardiopulmonary resuscitation in Nigerian schools, there is need for adequate relevant reports on this subject for evidence-based decisions. University students of Human Kinetics and Health Education occupy a very good position in this advocacy both as practitioners in community and public health education and as potential teachers in both primary and secondary schools.A group of such Nigerian University youths were trained in bystander CPR over a year ago using the conventional (standard) method This study aimed at assessing their retained CPR skills fifteen (15) months after their initial training to confirm their potential readiness to provide effective bystander CPR services to possible victims of out-of-hospital cardiac arrest (OHCA). We hypothesized that: (1) most of them would have poor retained CPR skills and as such would not be able to provide effective bystander CPR services for potential victims of OHCA; and (2) their retained CPR skills would have dropped significantly from their earlier immediate post-training CPR skills levels 15 months ago.
2. Materials and Methods
2.1. Study Design
- This report is part of a follow up of a randomised experimental study which was carried out in March 2018 when this cohort were trained on bystander cardiopulmonary resuscitation (CPR) using the conventional method. The participants (University students of the Department of Human Kinetics and Health Education, Faculty of Education, University of Port Harcourt) who were initially seventy (70) in the cohort were re-assessed on their CPR skills fifteen (15) months after the initial training without another training.They were exposed to the same simulated scenarios of a victim of out-of-hospital cardiac arrest (OHCA) using manikins. The same American Heart Association (AHA)-certified Assessor who assessed the same participants in 2018 re-assessed their CPR skills using the same modified AHA Skills Evaluation Guide. The assessment involved four domains for the conventional technique (method) – (1) Scene Safety and call for Help (SS), (2) Chest Compression (CC), (3) Airway / Rescue Breaths (RB) and (4) Cycle / min and Placement of Victim in correct Recovery Position (RP).
2.2. Study Cohort
- It was easy to match the retained skills of each participant with the earlier immediate post-training skills using their matriculation numbers indicated on each scoring sheet. In all, only sixty-five (65) in the earlier cohort of seventy (70) participants were available for the re-assessment of the retained CPR skills in June 2019.The following null hypotheses were generated and tested: Ho1 – most of them would have poor retained CPR skills and as such would not be able to provide effective bystander CPR services for potential victims of OHCA; and Ho2 - their retained CPR skills would have dropped significantly from their earlier immediate post-training skills levels after 15 months of their earlier training.
2.3. Determination of Good and Poor CPR Skills
- As in earlier reports [10-13], for each of the four domains of the CPR skills, retention of at least 50% of the post-training CPR skills is considered as acceptable or good while scores less are deemed poor or unacceptable.
2.4. Data Analysis
- The statistical Package for Social Sciences (SPSS) was used to analyse the data. Besides the descriptive statistics, the paired sample T-test was used to analyse the data collated in 2018 and the present. The significance level was set at P < 0.05.
2.5. Ethical Approval and Participants Consent
- As was explained earlier [12,13], Institutional Consent was not considered necessary because the work was relevant to the training and teaching of ‘Safety Education and First Aid’ that is part of the participants’ course work. Moreover, the study is very non-invasive and the participants were also very much interested in the study as it offered them the opportunity to learn this very important safety skill.
3. Results
- Fifty (50) females and fifteen (15) males participated in this retention phase of this study with age range of 18 to 29 years and mean age of 22.22 + 2.64 (SD). Table 1 shows the comparison of the immediate post training CPR skills of the participants and their retention after 15 months with the best retention found in chest compression having 57 (87.3%) while the worst was in remembering what to do to maintain scene safety and call for help first as only 30 (46.2%) retained this skill. Thirty-five (53.9%) retained good maintenance of airway and rescue breaths skill while the cycle /min and placing the victim in the correct recovery position had 39 (60%) having good retention.
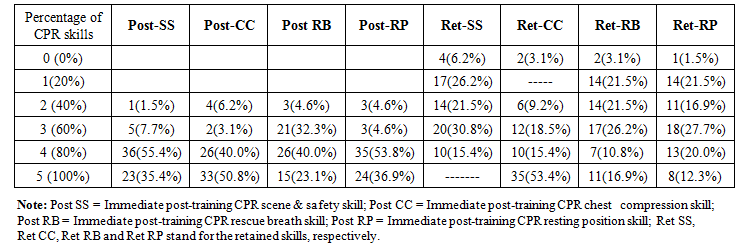 | Table 1. Comparison of the immediate post training CPR skills of the participants and retention after 15 months |
|
4. Discussion
- This Nigerian study on retention of CPR skills 15 months after the initial conventional CPR training has showed that although the participants lost significantly some of their earlier CPR skills, especially in relation to the domains of scene safety and call for help, rescue breaths and placement of victim in correct recovering position, they still generally had acceptably good CPR skills with impressive retained chest compression skills for effective possible bystander CPR provision to potential victims of OHCA. In a much earlier study, Wilson et al [14] reported that the participants had 60-70% average retention compared to their training scores. This is comparable to our present study which recorded 60% and above having good retention of all the CPR skills. According to Wilson et al [14], 16 (40%) of those retested were able to perform effective ventilations and compressions of the manikin while our study gave over 87% able to give effective chest compression and 53.9% capable of providing effective rescue breaths. In a study that aimed at determining the skills and knowledge decay in first aid in those who are paid to respond to emergency situations within a workplace, using a choking victim scenario, Anderson at al [15] reported that compressions following the victim becoming unconscious showed classic signs of skill deterioration after 30 days. Although Nishiyama et al [16] concluded that the shortened compression-only CPR training programme appeared to help the general public retain CPR skills better than the conventional CPR training programme, conventional CPR programme was equally effective in training potential lay rescuers: call for emergency number had 50 (80.6%) for compression-only CPR as against 49 (89.1%) for conventional.In Nigeria, the two previous related reports on retention of CPR skills agreed that conventional CPR training holds promise in our environment for retention of adequate CPR skills for effective bystander CPR provision [9,11]. In a related study in Flanders in 2014, Iserbyt and Mols [17] were able to show that the CPR skill performance and skill decay of Pedagogy students' CPR performance assessed 3 weeks and 12 months following reciprocal learning by an expert teacher versus a non-expert teacher resulted in students taught by theexpert demonstrating significantly higher chest compression rates, although this observation was not clinically relevant.They concluded that instructors with no certification and expertise in BLS can achieve equal learning outcomes,as certified instructors when applying reciprocal learning with task cards. In our present study with very satisfactory outcome even after 15 months a trained and certified American Heart Association (AHA) instructor trained and assessed the participants. Hupfl et al [18] in their meta-analysis showed that from three randomised trials that chest-compression-only CPR was associated with improved chance of survival compared with standard CPR (14% [211/1500] vs 12% [178/1531]; risk ratio 1·22, 95% CI 1·01-1·46). However, in the secondary meta-analysis of seven observational cohort studies in that study [18], no difference was recorded between the two CPR techniques (8% [223/2731] vs 8% [863/11 152]; risk ratio 0·96, 95% CI 0·83-1·11).To compare the effectiveness of different compression-to-ventilation methods during cardiopulmonary resuscitation (CPR) in patients with cardiac arrest, Ashoor et al [19] concluded that for adults, CPR 30:2 is associated with better survival and favourable neurological outcomes when compared to CPR 15:2 while for children, more patients receiving CPR with either 15:2 or 30:2 compression-to ventilation ratio experienced favourable neurological function and survival. It is, therefore, certain that different methods could provide useful means of helping victims of cardiac arrest. Meanwhile, the major challenge to conventional (standard) technique in terms of providing enough potential bystander providers is the time it takes to train laypeople through this means compared to the chest compression-only CPR.Sarac and Ok [20] in their study involving different instructional methods for the training laypersons in CPR, discovered that the students trained using the traditional and case-based instruction methods showed better CPR performance than students in web-based instruction group that used video self-instruction as a learning tool. There is yet to be any study in Nigeria on CPR instructional method involving the video self-instruction method.Considering the period of 15 months before the re-assessment of the retention of skills in this Nigerian study, the outcome is very encouraging. Riggs et al [21] in their systematic review study opined that training sessions should utilise combinations of validated skill-specific training strategies, preferably including popular songs and feedback to help ensure skills retention. They further stated that refresher training, which focuses on skills and self-confidence rather than knowledge, should be undertaken every 3-6 months, although this timeframe needs further validation. The decay or decline in CPR competency has been documented globally necessitating the importance place of re-trainings for effective CPR provision to victims [22].
5. Strengths and Limitation of the Study
- Being one of the few studies in Nigeria on retention of CPR skills involving medically untrained students, as well as having the participants from different parts of Nigeria because the students were admitted based on a quota system policy of the Federal Government of Nigeria on admission into the Federal Universities, this type of study could have a multiplier effect as these potential teachers train their future students. However, the sample is understandably not large for a populous country like Nigeria.
6. Conclusions
- • In all, average of 61.85% of the participants generally had acceptably good retained CPR skills (60% of CPR skills and above) 15 months after their initial training using the conventional CPR training method.• Although the participants lost significantly some of their earlier CPR skills, especially in relation to the domains of scene safety and call for help, rescue breaths and placement of victim in correct recovering position, that was not so in the chest compression skills where they had impressive retained chest compression skills for effective possible bystander CPR provision to potential victims of OHCA.
7. Recommendations
- There is need for more related studies across the country with greater sample sizes involving more schools and work communities in order to increase the awareness of bystander CPR and the number of potential providers for victims of out=of-hospital cardiac arrest (OHCA) in our country.
References
| [1] | Vaillancourt C, Lui A, De Maio VJ, Wells GA, Stiell IG. Socioeconomic status influences bystander CPR and survival rates for out-of-hospital cardiac arrest victims. Resuscitation 2008; 79(3): 417-423. |
| [2] | Ahn KO, Shin SD, Suh GJ, et al. Epidemiology and outcomes from non-traumatic out-of-hospital cardiac arrest in Korea: a nationwide observational study. Resuscitation 2010; 81: 97481. |
| [3] | Mawani M, Kadir MM, Azam I, et al. Epidemiology and outcomes of out-of-hospital cardic arrest ina developing country-a multicenter cohort study. BMC Emerg Med 2016; 16: 28. |
| [4] | Rea TD, Eisenberg MS, Becker LJ, Murray JA, Hearne T. Temporal trends in sudden cardiac arrest; 25-year emergency medical services perspectives. Circulation 2003; 107: 2780-5. |
| [5] | Sasson C, Magid DJ, Chan P, Root ED, McNally BF, Kellermann AL, Haukoos JS. Association of Neighbourhood Characteristics with Bystander-initiated CPR. N EngI J Med. 2012; 367: 1607-1615. |
| [6] | Chiang WC, Ko PCI, Chang AM, Chen WT, Liu SSH, Huang YS et al. Bystander –initiated CPR in an Asian metropolitan: Does the socioeconomic status matter? Resuscitation 2014; 85(1): 53-58. |
| [7] | Sasson C, Rogers MA, Dahl J, Kellermann AL. Predictors of survival from out-of-hospital cardiac arrest: a systematic review and meta-analysis. Circ Cardiovasc Qual Outcomes 2010; 3:63-81. doi: 10.1016/j.resuscitation.2008.07.012. |
| [8] | Onyeaso AO. Awareness of Cardiopulmonary Resuscitation among Secondary School Students in Port Harcourt, Nigeria. Journal of Education in Developing Areas 2014; 22(1): 137-142. |
| [9] | Onyeaso AO. Retention of Cardiopulmonary Resuscitation Skills in Nigerian Secondary School Students. J Educ Pract 2016; 7(15): 162-168. |
| [10] | Onyeaso AO, Onyeaso OO. Cardiopulmonary Resuscitation Skills of some Nigerian Primary and Secondary Schools Teachers. J Adv Med Med Res 2017; 23(2): 1-8. |
| [11] | Onyeaso AO, Onyeaso CO. Retention of Cardiopulmonary Resuscitation Skills in a Group of Nigerian School Teachers. Am J Med Med Sci 2018, 8(6): 112-116. DOI: 10.5923/j.ajmms.20180806.03. |
| [12] | Onyeaso AO, Onyeaso CO. Chest Compression-Only Cardiopulmonary Resuscitation in Nigerian University Students. Am J Med Med Sci 2018; 8(8): 213-218. |
| [13] | Onyeaso AO, Onyeaso CO. Comparison of the Conventional and Hands-Only Cardiopulmonary Resuscitation Skills Performance of Some Nigerian University Students. Am J Med Med Sci 2018; 8(9): 235-240. |
| [14] | Wilson E, Brooks B, Tweed WA. CPR skills retention of lay basic rescuers. Ann Emerg Med 1983; 12(8): 482-4. |
| [15] | Anderson GS, Gaetz M, Masse J. First aid skill retention of first responders within the workplace. Scand J Trauma Resusc Emerg Med 2011, 19:11. |
| [16] | Nishiyama C, Iwami T, Kitamura T, Ando M, Sakamoto T, Marukawa S, Kawamura T. Long-term Retention of Cardiopulmonary Resuscitation Skills After Shortened Chest Compression–only Training and Conventional Training: A Randomized Controlled Trial. Acad Emerg Med 2014; 21: 47-54. |
| [17] | Iserbyt P, Mols L. Retention of CPR skills and the effect of instructor expertise one year following reciprocal learning. Acta Anaesthesiol Belg 2014; 65(1): 23-9. |
| [18] | Hupfl M, Selig HF, Nagele P. Chest-compression-only versus standard cardiopulmonary resuscitation: a meta-analysis. Lancet 2010; 376(9752): 1552-7. doi: 10.1016/S0140-6736(10)61454-7. |
| [19] | Ashoor HM, Lillie E, Zarin W, Pham B, Khan PA, Nincic V, et al ILCOR. Basic Life Support Task Force. Effectiveness of different compression-toventilation methods for cardiopulmonary resuscitation: A systematic review. Resuscitation 2017; 118: 112-125. Doi: 10.1016/j.resuscitation.2017.05.032. |
| [20] | Sarac L, Ok A. The effects of different instructional methods on students' acquisition and retention of cardiopulmonary resuscitation skills. Resuscitation 2010; 81(5): 555-61. doi: 10.1016/j.resuscitation.2009.08.030. |
| [21] | Riggs M, Franklin R, Saylany L. Associations between cardiopulmonary resuscitation (CPR) knowledge, self-efficacy, training history and willingness to perform CPR and CPR psychomotor skills: A systematic review. Resuscitation 2019; 138: 259-272. doi: 10.1016/j.resuscitation.2019.03.019. |
| [22] | Alspach G. CPR-the Vanishing Competency. Crt Care Nurs 2995; 25(6): 8-12. |
| [23] | Donnelly P, Assar D, Lester C. Comparison of manikin CPR performance by lay persons training in three variations of basic life support guidelines. Resuscitation 2000; 45: 195-199. |
| [24] | Wik L, Myklebust H, Auestad BH, Steen PA. Retention of basic life support skills 6 months after training with an automated voice advisory manikin system without instructor involvement. Resuscitation 2002; 52: 273-279. |
| [25] | Su E, Schmidt TA, Mann NC, Zechnich AD. A randomized controlled trial to assess decay in acquired knowledge among paramedics completing a paediatric resuscitation course. Acad Emerg Med 2000; 7: 779-786. |