-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2020; 10(5): 318-323
doi:10.5923/j.ajmms.20201005.09

Retention of Cardiopulmonary Resuscitation Skills after 15 Months of Initial Chest Compression-Only Training of Some University Students in Nigeria
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAdedamola Olutoyin Onyeaso1, Chukwudi Ochi Onyeaso2
1Department of Human Kinetics and Health Education, Faculty of Education, University of Port Harcourt, Port Harcourt, Nigeria
2Department of Child Dental Health, Faculty of Dentistry College of Health Sciences, University of Port Harcourt / University of Port Harcourt Teaching Hospital, Port Harcourt, Nigeria
Correspondence to: Adedamola Olutoyin Onyeaso, Department of Human Kinetics and Health Education, Faculty of Education, University of Port Harcourt, Port Harcourt, Nigeria.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Introduction: There is sufficient information globally on the effectiveness of chest compression-only CPR in providing adequate bystander CPR for victims of out-of-hospital cardiac arrest (OHCA) but there is no single report on the retention of such skills by potential providers of bystander CPR in Nigeria. For potential bystander CPR providers to provide this useful service to victims of OHCA, they must be able to retain the skills for a reasonable period of time before re-training takes place. This study aimed at assessing the retention of CPR skills 15 months after the initial training on chest compression-only CPR in a group of Nigerian students. Materials and Methods: A quasi-experimental study design was used. The initial cohort were seventy but this reduced to sixty-five consisting 50 (76.92%) females and 15(23.08%) with age range of 18-31 years (mean age, 22.11+ 2.80). Their CPR skills were assessed immediately post-training 15 months ago and re-assessed at the retention stage by the same AHA-certified CPR Instructor using the same modified AHA Skills Evaluation guide. Three CPR skills domains were assessed – scene safety and call for help, chest compression and cycle / min and placement of victim in correct recovery position. The data were analysed using descriptive statistics and paired sample t-test with P-value set at P < .05. Results: The participants had impressive CPR skills retention 15 months later. Only the scene safety and call for help CPR skills domain had significant loss (P < .001) while the remaining skills domains did not. Generally, the retained chest compression skills of the participants had marked improvement on their immediate post-training levels but not significant (P > .05). Conclusion: Chest compression-only CPR holds promise as an adequate technique for increasing the number of potential bystander CPR providers for the general public in our environment.
Keywords: Chest compression CPR technique, CPR skills Retention, University students, Nigeria
Cite this paper: Adedamola Olutoyin Onyeaso, Chukwudi Ochi Onyeaso, Retention of Cardiopulmonary Resuscitation Skills after 15 Months of Initial Chest Compression-Only Training of Some University Students in Nigeria, American Journal of Medicine and Medical Sciences, Vol. 10 No. 5, 2020, pp. 318-323. doi: 10.5923/j.ajmms.20201005.09.
Article Outline
1. Introduction
- The usefulness of bystander cardiopulmonary resuscitation (CPR) in the outcome of victims of out-of-hospital cardiac arrest (OHCA) has been widely documented [1-8]. Central to effective bystander CPR provision is the ability of trained bystanders to retain their CPR skills for sometime before re-training programmes. Across the globe, various researchers have reported their findings on retention of cardiopulmonary resuscitation skills by bystander CPR providers with different levels of retained skills [9-13].In Nigeria, few reports have shown that Nigerian school children and teachers could retain reasonable levels of their CPR skills following initial trainings [14,15]. Earlier reports from Nigeria have shown that some Nigerian University students, who are potential teachers in primary and secondary schools, displayed impressive acquisition of CPR skills [16-20], but reports on the CPR skills retention ability of such important target group in the popularization of the bystander CPR among Nigerians is very essential.Although the quality outcomes of Hands-Only CPR trainings for bystander CPR skills are documented [21-29], there is need for more reports on the retained skills of such trainings especially in Nigeria where there is no such report so far.Nigeria is a developing economy and is not spared of the globally increasing public health burden of out-of-hospital cardiac arrest (OHCA). In addition, the role of teachers and students in our advocacy for integration of the teaching and training in bystander into Nigerian schools’ curricula is crucial. Therefore, this study aimed at ascertaining the level of retention of earlier acquired CPR skills through Hands-Only CPR training programme by some University students (potential teachers) in Nigeria. It was hypothesized that: (1) the retention of CPR skills by most of the students in the group would be poor. after over a year of their initial CPR training using the Hands-Only method; and (2) there would be statistically significantly losses in CPR skills in all the three domains assessed.
2. Materials and Methods
2.1. Study Design
- A quasi-experimental design was used.
2.2. Population of the Study
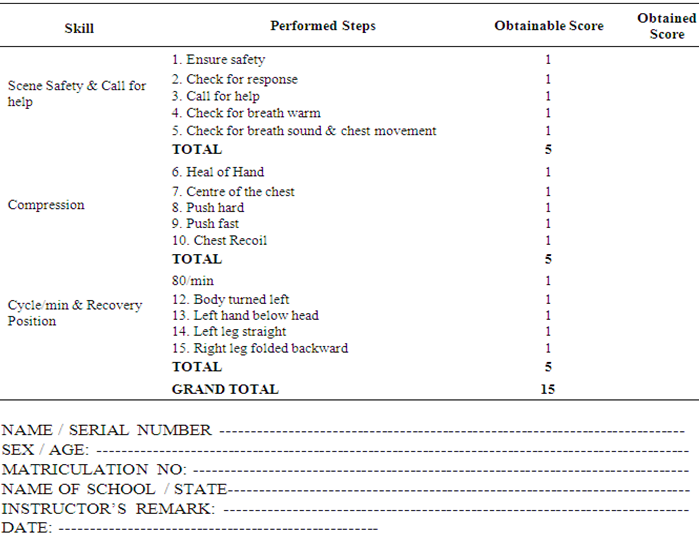
- The initial cohort of seventy (70) participants was 200-Level undergraduate students in the Department of Human Kinetics and Health Education, Faculty of Education, University of Port Harcourt. The participants had CPR training using the hands-only method in March 2018. Their immediate post-training CPR skills were assessed then by the lead researcher who is an American Heart Association (AHA)-certified CPR Instructor using a modified AHA Skills Evaluation Guide as in Onyeaso and Onyeaso [29]. See Appendix below.The same cohort that participated in the earlier study in 2018 were recalled to carry out the hands-only CPR skills in a similar simulated situation using manikins in June, 2019. Without further teaching or training in bystander CPR, they were asked to individually carry out bystander CPR for a simulated victim with out-of-hospital arrest (OHCA). Each of them was assessed by the same lead researcher who did it 15 months ago. The three CPR skills domains assessed were: scene safety and call for help (SS), chest compression (CC) and Cycle / min and correct placement of victim in recovery position (RP). The same modified AHA guideline was used by the same CPR Instructor to assess each participant. The matching of the participants earlier immediate post-training hands-only CPR skills was easy because their matriculation numbers were written on top of each of the assessment form. In all, sixty five (65) of the original cohort of seventy (70) participated at this stage of assessing their retained CPR skills – 50 (76.92%) females and 15(23.08%) with age range of 18-31 years (mean age, 22.11+ 2.80).The following null hypotheses were generated and tested:Ho1: The retention of CPR skills by most of the students in the group would be poor after over a year of their initial CPR training using the Hands-Only method; and Ho2: There would be statistically significantly losses in CPR skills in all the three domains assessed.
2.3. Determination of Poor and good CPR Skills
- Score of 50% was considered acceptable (good) for each of the three domains of chest compression-only (hands-only) CPR skills while less than 50% was considered unacceptable (poor) retained CPR skills.
2.4. Data Analysis
- The Statistical Package for Social Sciences (SPSS) was used to analyze the data. In addition to descriptive statistics, the data collated 15 months ago and the present data on retention were analyzed using the paired samples T-test. The P-value was set at 0.05 level of significance.
2.5. Ethics and Participants Consent
- Institutional review and consent was not necessary as the programme was within the course work of the students and was completely non-invasive. In addition, the students were very enthusiastic to participate in the study because of the obvious benefit they would derive from it. In all, the participants freely gave their consent.
3. Results
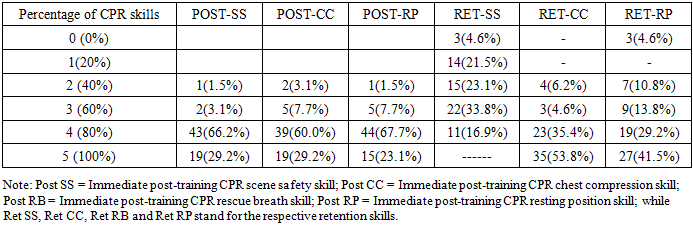
- Comparison of the immediate post-training CPR skills and retention by the participants after 15 months of initial hands-only CPR skills training are shown in Table 1 below. They produced the best retention in their chest compression skills where 61 (93.8%) had 60% and above, followed by Cycle / min and correct placement of victim in recovery position having 55 (84.5%). It is important to note also that hands-only CPR skill involving chest compression domain had more participants (53.8%) scoring 100% than during their immediate post-training assessment (29.1%), although double of participants had 40% which is considered unacceptable.
|
|
|
4. Discussion
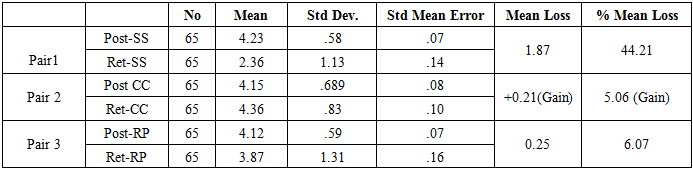
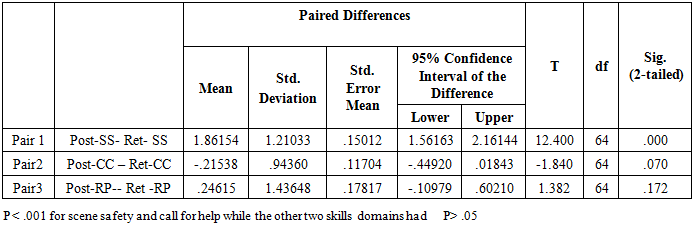
- This first Nigerian study on the retention of CPR skills after the initial chest compression-only (hands-only) CPR training has revealed statistically significant drop in the participants skills in the scene safety and call for help CPR skills domain only while the differences in their retained skills in relation to chest compression and cycle / min and placement of victim in the correct recovery position domains were not statistically significant. However, it must be noted that in all the participants actually gained in the chest compression skill 15 months after and not loss. Bobrow et al [25] reported that victims of out-of-hospital cardiac arrest who received chest compression-only bystander CPR had increased survival rates. They concluded that among patients with out-of-hospital cardiac arrest, layperson compression-only CPR was associated with increased survival compared with conventional CPR and no bystander CPR in this setting with public endorsement of chest compression-only CPR. [25]. According to Lim et al [30], the chest compression-only group produced superior chest compression compared with their conventional counterparts.Although Kim et al [23] reported that chest compression-only CPR did not produce as good chest compression as the conventional CPR in their retention study, it did not mean that chest compression-only CPR was not good. Moreover, their retention assessment was just after 3 months unlike our present study that assessed retention after 15 months. Iwami et al [31] concluded in their study that compression-only CPR is more effective than conventional CPR for patients in whom out-of-hospital cardiac arrest is witnessed and shocked with public-access defibrillation. They further opined that compression-only CPR is the most likely scenario in which lay rescuers can witness a sudden collapse and use public-access AEDs.In their prospective observational study, Iwami et al [32] found ou that bystander-initiated cardiac-only resuscitation and conventional CPR were similarly effective for most adult out-of-hospital cardiac arrests. Roppolo and Pepe [33] had earlier emphasized the importance of retention of CPR skills and its multiplier effect through schools. The very impressive retention of CPR skills observed in this study by potential teachers is an encouraging development because it is expected that some of these students will contribute in the teaching of this vital safety procedure in primary and secondary schools. Therefore, this finding with chest compression-only CPR holds great potential for our community where many would not want to carry out bystander conventional CPR because of the fear of contacting diseases [34].The only related earlier studies in Nigeria on retention of CPR skills were on conventional CPR training [14,15] and all showed satisfactory retention. With the current finding on chest compression-only CPR, it could be said that Nigerian students both at the secondary and University levels have shown satisfactory retention of CPR skills which is a promising development with regard to the future of bystander CPR training and practice in the country. In fact, a meta-analysis on chest compression-only and standard (conventional) CPR training programmes by Hupfl et al [35] led them to conclude that for adults with out-of-hospital cardiac arrest (OHCA), instructions to bystanders from emergency medical services dispatch should focus on chest-compression-only CPR.
4.1. Strengths and Limitations of the Study
- Being a pioneer study on chest compression-only CPR skills retention in Nigeria, this study will serve as a baseline work in this aspect and would stimulate further related studies. However, there is need to improve on the sample size involving a larger cross-section of Nigerian lay persons.
4.2. Conclusions
- • The retention of CPR skills in this study by the participants was generally very satisfactorily good without significant differences in the chest compression and cycle / min and placement of victim in correct recovery position domains except for the scene safety and call for help domain.• Although there was no significant difference in the chest compression skills of the participants, there was gain instead of loss in their chest compression skills 15 months after the initial training.The results suggest that chest compression-only CPR skills training technique is adequate for producing more potential bystander providers for the general public including our Nigerian environment.
4.3. Recommendations
- More related studies in Nigeria involving lay persons in schools (primary, secondary and tertiary institutions) and communities from different parts of the country are encouraged so as to increase the number of potential bystander CPR providers and chest compression-only CPR offers this chance because the fear of contacting diseases is not there.