-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2020; 10(5): 309-313
doi:10.5923/j.ajmms.20201005.07

Evaluation of Risk Factors of Progressing IgA Nephropathy in Children
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKomiljon Khamzaev , Alisher Sharipov
Tashkent Pediatric Medical Institute, Tashkent, Uzbekistan
Correspondence to: Komiljon Khamzaev , Tashkent Pediatric Medical Institute, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Clinical and morphological changes in the IgA nephropathy in children to determine high risk patients for disease progression. Our research included 29 patients at age <17. During framework of the research therapy of the IgA nephropathy included prednisolone, azathioprine and dipyridamole, length of the therapy was 24 months. Kidney biopsy was performed to the all patients which revealed IgA nephropathy in >80% glomeruli with mesangial proliferation. In our research in children with IgA nephropathy 24 hour protein excretion and frequency of glomeruli with crescents were independent risk factors of permanent proteinuria by the end of 2 years combined therapy. Combined therapy of children with severe IgA nephropathy showed good efficiency, but it can be less effective for children with 24 hour urine excretion >1,32g/1,73m2 or crescents in the biopsy in more than 14% glomeruli.
Keywords: IgA nephropathy, Crescents, Mesangial proliferation, Proteinuria
Cite this paper: Komiljon Khamzaev , Alisher Sharipov , Evaluation of Risk Factors of Progressing IgA Nephropathy in Children, American Journal of Medicine and Medical Sciences, Vol. 10 No. 5, 2020, pp. 309-313. doi: 10.5923/j.ajmms.20201005.07.
1. Background
- IgA nephropathy is the most common nephritis in the world. Disease prevalence varies geographically, with biopsy and hemodialysis registries pointing to geographical differences in the burden of disease with higher frequency in Asia and the Pacific. Without a kidney biopsy registry, the burden of disease is underestimated because patients with mild disease may not be biopsied and, in countries where IgA nephropathy screening program and quality kidney biopsy are not available, this disease may not be detected. A systematic review of studies based on kidney biopsy results covering several countries shows that the total incidence of IgA nephropathy (IgAN) is at least 2.5 per 100,000 people [1].Combined cohorts from the European Evaluation Study of the Oxford Classification of IgA nephropathy (VALIGA) and North American cohorts indicate that within 10 years 27% of patients experience terminal stages of chronic renal disease or a 50% reduction in estimated GFR [2]. A study in Japan found that 11% of 241 children with IgAN had terminal stages of chronic renal failure [3]. Factors associated with poor prognosis of the IgA nephropathy are not fully determined. The authors believe that children with IgA nephropathy with diffuse mesangial proliferation on kidney biopsy have a high risk of progressive deterioration of renal function, 17% of these children had impaired renal function (in whom GFR <60 ml/min/1.73m2 including children who started hemodialysis sessions), 0.9% of children who had focal mesangial proliferation in their kidney biopsy [3].In two randomized controlled trials, Yoshikawa N and others for the treatment of IgA-nephropathy with diffuse mesangial proliferation demonstrated the efficacy of 2-year combined treatment with steroids, immunosuppressants, antiaggregant and anticoagulant drugs [4,5]. However, some patients, especially those who had persistent proteinuria at the end of 2-year therapy, developed chronic renal failure. Many authors believe that sustained proteinuria is closely related to the future development of chronic renal failure [6]. The discovery of IgA/IgG deposits in renal biopsy tissue indicates the immunocomplex nature of the disease. In 15-20% of patients, mesangial deposits contain secretory IgA1. Available clinical data revealed a connection between a previous infection of the upper respiratory tract and secretory IgA deposits in kidney tissue. Colocalization of IgA with mannose-binding lectin, L-ficolin, and C4d component of the complement was observed, which indicates IgA-induced activation of complement system along with the lectin (mannose binding) pathway. At present, some issues of IgA-nephropathy pathogenesis remain open and are the subject of numerous studies [7,8,9].The clinical pattern of IgA nephropathy is variable. In 43.3% of cases, the disease is latent and revealed accidently. Besides, hematuria form is found in 38% of cases, and the development of nephrotic syndrome - in 16.1% [10].The main diagnostic method of IgA nephropathy is kidney biopsy, indications for which are repeated episodes of macrohematuria in a patient with microhematuria and proteinuria, especially in combination with arterial hypertension and reduction of GFR [11,12].Following Oxford classification of IgA nephropathy MEST+C 2016 is used for interpretation of the obtained morphological changes: M1 - presence of mesangial hypercellularity in more than 50% of the glomeruli; E1 - presence of endocapillary hypercellularity; S1 - presence of segmental sclerosis; T1 - tubular atrophy and interstitial fibrosis in 25-50%; C1 - crescents in less than 25% of the glomeruli [13,14,15].Objective of the research was to study clinical and morphological changes in IgA-nephropathy in children to identify patients with high risk of disease progression.
2. Materials and Methods
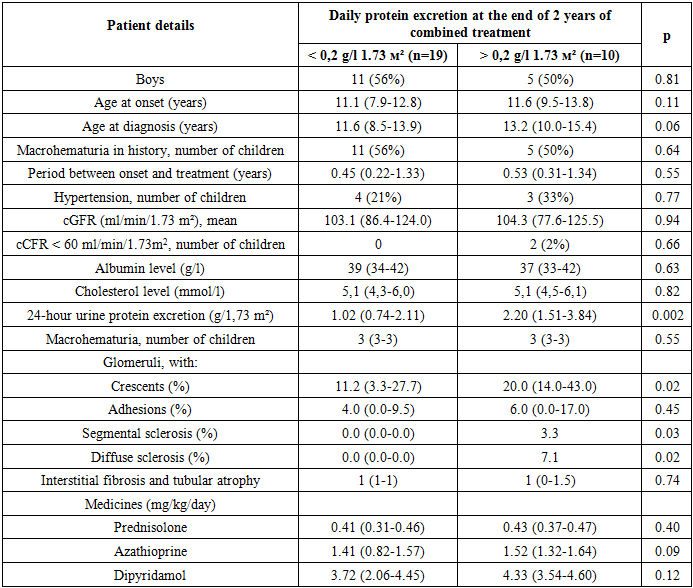
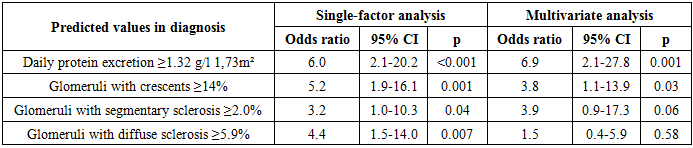
- A total of 29 patients aged <17 years were included to our study. During framework of the research therapy of the IgA nephropathy included prednisolone, azathioprine and dipyridamole, length of the therapy was 24 months. Kidney biopsy was performed to the all patients which revealed IgA nephropathy in >80% glomeruli with mesangial proliferation. All patients included to the study had not been previously treated with corticosteroids or immunosuppressive drugs. Children with chronic liver diseases and systemic diseases such as systemic lupus erythematosus, Henoch-Schonlein purpura were not included in the study. Prednisolone was administered orally at a dose of 2 mg/kg/day (maximum 60 mg/day) in two separate doses in the morning for 4 weeks, then 2 mg/kg/day for 4 weeks, 1.5 mg/kg/day for 4 weeks, and finally 1 mg/kg/day for 21 months. Azathioprine was administered orally at a dose of 2 mg/kg/day in a single morning dose for 24 months. Dipyridamol was administered orally in a dose of 5 mg/kg/day (max 400 mg/day) in three separate doses for 24 months. In this study, the initial protein loss (before treatment - at the time of diagnosis) was compared with proteinuria at the end of 2-year combination therapy. Children after treatment were divided into 2 groups: without proteinuria (<0.2 g/day) and with persistent proteinuria (≥0.2 g/day). The average duration of observation for the period of treatment was 7 years.We also analyzed the risk factors for the development of resistant proteinuria using multivariate analysis. Initial data before kidney biopsy included the following clinical parameters: sex of children, duration of the disease, age at the diagnosis, presence of macrohematuria in the history, interval between the onset of symptoms and start of the treatment, presence of arterial hypertension, renal function (calculated GFR), serum albumin level, serum cholesterol level, daily (24-hour) excretion of protein with urine and the degree of hematuria, as well as morphological features such as crescents, adhesion, segmental and diffuse sclerosis. In the study of kidney biopsy, morphological parameters were estimated as percentage of glomeruli with crescents, adhesion, segmental or diffuse sclerosis, as well as interstitial fibrosis and tubular atrophy on a scale from 0 to 2.Average daily doses of drugs (prednisolone, azathioprine, dipyridamol) per body weight were calculated for each patient during 2-year combination therapy and two groups (children with and without proteinuria) were compared.
3. Results
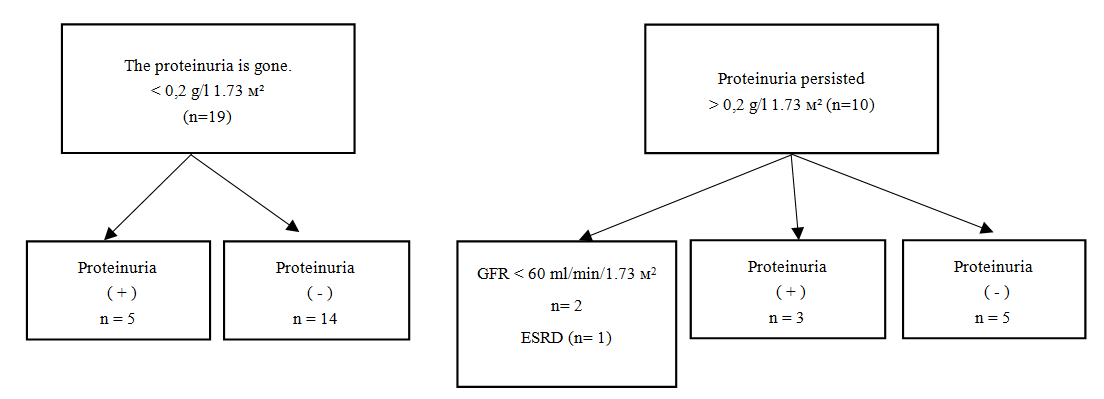
- At the beginning of treatment in 19 children (65%) daily excretion of protein with urine was >1g/1.73m2. At the end of the 2-year combination therapy, proteinuria persisted in 10 (34%) children (Fig.1). At the end of observation (7 years) 2 out of 29 patients developed chronic kidney insufficiency (GFR <60 ml/min/1,73m2), from which 1 developed end stage of renal disease. In those children who did not have proteinuria, chronic renal failure did not develop.
 | Figure 1. Results of follow-up of children with proteinuria at the end of 2 combined treatment and final prognosis |
|
|
|
4. Discussion
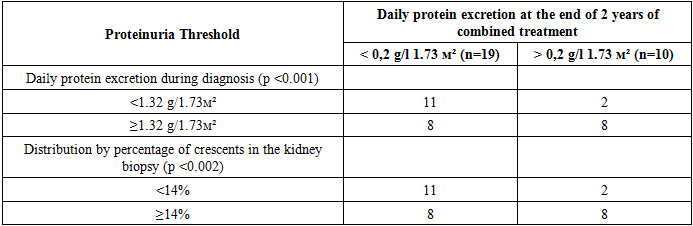
- In some studies, the authors propose certain clinical indicators of poor prognosis in IgA nephropathy including severe proteinuria, hypertension, impaired renal function during diagnosis, as well as morphological criteria such as the presence of crescents, segmental sclerosis, diffuse sclerosis, interstitial fibrosis and tubal atrophy [16,17,18,19]. The majority of studies on IgA nephropathy prognosis have been carried out in adults, while IgA nephropathy prognosis in children has not sufficiently studied. Our study showed that daily urine protein excretion and the frequency of glomeruli with crescents are independent risk factors for the development of persistent proteinuria by the end of 2 years of combined treatment in children with severe IgA nephropathy. Reduced renal function is a known risk factor in adult IgA nephropathy (20), but in our study we cannot prove that it is a significant risk factor due of the small number of children with reduced renal function at the beginning of the combined treatment. Severe proteinuria is a predictor of adverse prognosis in adults, so studies in this area are also being conducted in children with IgA nephropathy [20,21,22,23]. Our results showed that 2 years of combined treatment can lead to a decrease in proteinuria with severe IgA nephropathy, about one-third of children developed remission of proteinuria by the end of treatment. However, in those patients who had severe initial proteinuria, we believe that there is a possibility of persistence of proteinuria by the end of 2 years of combined treatment. It should be noted that in some papers the authors report the presence of crescents in the biopsy and define this fact as a risk factor for poor prognosis [24,25]. This is explained by the fact that in patients with IgA-nephropathy macrophages are infiltrated into the para-mesangial areas of the glomeruli and destroy the glomerular basal membrane. This leads to formation of crescents and adhesion of the capillaries to the Bowman capsule, which eventually causes glomerular sclerosis [26].In IgA nephropathy, small crescents formed by cells may be reversible with appropriate treatment. Although the report on the Oxford Morphological Classification of IgA-nephropathy did not indicate that the formation of crescent cells in children is a risk factor for poor prognosis of IgA-nephropathy [27]. However, our results showed that they are an independent risk factor for this poor prognosis.Thus, in our study in children with IgA nephropathy the daily urine protein excretion and the increase in the frequency of the glomeruli with crescents were independent risk factors for the development of permanent proteinuria at the end of 2 - year combined therapy. Although the combined treatment of children with severe IgA nephropathy shows good efficacy, it may not be effective enough for children in whom urine protein excretion is >1.32 g/1.73 m2/day, or crescents detected in the kidney biopsy in more than 14% of the glomeruli. We believe that additional methods of IgA nephropathy treatment, such as methylprednisolone pulse therapy, may be indicated for such patients with high risk, but further clinical studies are needed to evaluate its efficacy.