-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2020; 10(5): 279-283
doi:10.5923/j.ajmms.20201005.01

Cardiothoracic Ratio of Nigerians in Gas Flaring Communities
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLLoveday Ese Oghenemavwe1, Lydia Olufemi Awoyemi2
1Department of Anatomy Faculty of Basic Medical Sciences, College of Health Sciences University of Port Harcourt, Port Harcourt, Rivers State, Nigeria
2Biomedical Technology, School of Science Laboratory Technology, University of Port Harcourt, Port Harcourt Rivers State, Nigeria
Correspondence to: Loveday Ese Oghenemavwe, Department of Anatomy Faculty of Basic Medical Sciences, College of Health Sciences University of Port Harcourt, Port Harcourt, Rivers State, Nigeria.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The relationship between exposure to gas flaring and cardiothoracic ratio (CTR) have not been well characterized. The study therefore examines whether or not exposure to gas flaring has impact on cardiothoracic ratio. Digitalized postero-anterior chest radiographs of 200 patients from some selected University Teaching Hospitals and Image Diagnostic Centers in Rivers State and Oyo state of Nigeria between the ages of 19 to 70 years were used for the study.100 of them reside permanently in gas flaring communities of Rivers State while the other 100 reside permanently in non-gas flaring communities of Oyo State. Patients in each group had similar socio-economic status. The cardiac diameter (CD) and thoracic diameter (TD) were measured from the chest radiographs and the cardiothoracic ratio was determined by dividing CD by TD. The average CTR for males and females who reside in gas flaring areas of River State was 0.49 while those who reside in non-gas flaring communities of Oyo State was 0.46 and 0.47 for males and females respectively. The CTR differ significantly between both groups at P=0.000. The findings suggest exposure to gas flaring could lead to increase in cardiothoracic ratio an additional indicator that exposure to gas flaring could cause cardiovascular disease.
Keywords: Air Pollution, Cardiac diameter, Cardiothoracic ratio, Cardiomegaly, Gas Flaring, Thoracic diameter
Cite this paper: Loveday Ese Oghenemavwe, Lydia Olufemi Awoyemi, Cardiothoracic Ratio of Nigerians in Gas Flaring Communities, American Journal of Medicine and Medical Sciences, Vol. 10 No. 5, 2020, pp. 279-283. doi: 10.5923/j.ajmms.20201005.01.
Article Outline
1. Introduction
- There is growing concern over the continuous gas flaring in Nigeria which has span over half a century because of its negative effects on individual and public health, ecology, socio-economic and political activities [1,2,3]. Gas flaring involves the practice of burning the natural gas into the atmosphere instead of deploying alternative methods that are environmentally friendly [1]. As at 2017, the Nigeria National Petroleum Corporation (NNPC) reported that the total volume of gas flared by oil and gas companies have increased by 17% year-on-year to 287.59 billion standard cubic feet [4]. A higher percentage of this activity occurs in the Niger Delta Region of Nigeria which has six states namely, Akwa Ibom, Bayelsa, Cross Rivers, Delta, Edo and Rivers States [3,5]. Between 1970 and 1986, a total of 102.3 million cubic metres (mcm) of gas was flared out of 125.5 mcm generated in the Niger Delta [3]. The flared gas especially with incomplete combustion introduces toxic chemical substances such as methane, sulphur dioxide, volatile organic compounds (VOC), polycyclic aromatic carbons (PAHs) and soot (particulate matters) into the environment [6,7]. The result is air pollution, greenhouse effect and general environmental degradation especially around the communities where the gas is flared [1,5,8]. The negative health impacts of gas flaring are well documented [1,9,10]. There is increase mortality rate in Niger Delta States where gas is flared compared to non-gas flaring states and a positive relationship have been established between volume of gas flared and crude death rate. [1] Striking deterioration in haematological parameters, reduced peak expiratory flow rate, respiratory morbidities, increased systolic blood pressure, skin disorders and other related health risks have been reported. [11] It has also been established that there is decreased cardiopulmonary function with longer duration of exposure, reduced renal function with increase in serum concentrations of urea, creatinine, potassium, uric acid and inorganic phosphate [9,10]. Cardiothoracic ratio (CTR) is formed by dividing the transverse cardiac diameter by the transverse chest diameter on a postero-anterior (PA) chest film and it is use in clinical investigation to determine cardiomegaly (enlarged heart) and cardiac function [12,13,14,15,16]. It is a cheap, affordable and easy investigative tool commonly used in resource limited countries for heart evaluation [13,15]. According to Longbak and Co [17] cardiomegaly may not necessary indicate there is an underlying disease just as a normal heart size also does not necessary exclude underlying cardiac disease, however, it often gives first clue of some cardiovascular anomaly. The causes of cardiomegaly are poorly understood in most people, however lifestyle such as the use of tobacco which is an air pollutant has been implicated. Other causes are congenital, pulmonary hypertension, heart valve disease, pericardial effusion, thyroid disorder, chagas disease etc. Although several studies have implicated gas flaring in cardiovascular diseases, studies assessing CTR which is indicative of a cardiac function and heart size of residents of gas flaring communities are very rare. Hence, we set out to assess the cardiothoracic ratio of people exposed to gas flaring.
2. Materials and Methods
- The retrospective study evaluated the CTR of 200 patients from digital PA chest x-ray films taking between January 2017 to September 2018 in selected University Teaching Hospitals and Image Diagnostic Centers in Rivers State and Oyo state of Nigeria. The medical records showed 100 of the patients permanently reside in gas flaring communities of Eleme, Okrika, Omuko and Aluu in Rivers State while the other 100 persons were from communities in Oyo State, where gas is not flared. The patients selected in both groups have similar socio-economy status as shown in the medical records and they are mainly farmers, traders, students, artisans and civil servants. Patients who do not have hypertension or any form of cardiovascular disease and are above 18 years as indicated by medical records were included in the study. Poorly taken chest x-ray of patients with blurred cardiac and thoracic borders, smokers, patients with thoracic or spinal deformity, mediastinal shift and severe rotation were excluded. The parameters measured were cardiac diameter (CD) and thoracic diameter (TD) [See figure 1]. The CTR was determined by dividing CD by TD. CD is the maximal horizontal distance between the most lateral points on the right and left borders of the heart measured from a computerised postero-anterior chest radiograph. TD is the maximal horizontal distance above the costophrenic angle between the lateral points on the border of the ribs.
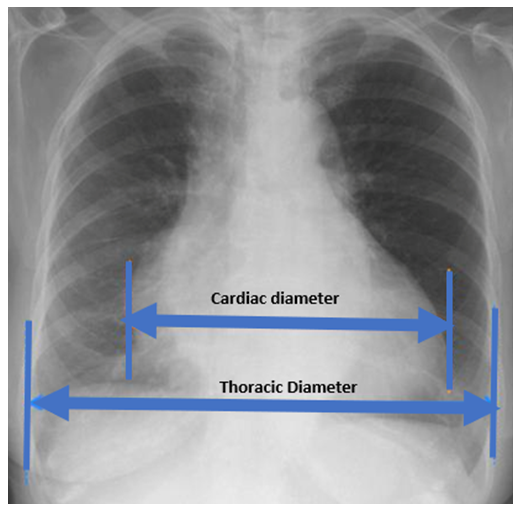 | Figure 1. Posteroanterior Chest radiograph showing cardiac and thoracic diameters |
3. Results
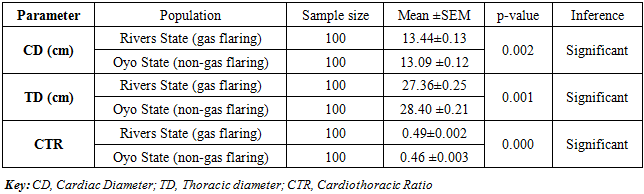
- The results are shown in tables 1-3. Irrespective of sex, the mean CTR for residents in gas flaring area of Port Harcourt was 0.49 while those for non-gas flaring area was 0.45.
|
|
|
4. Discussion
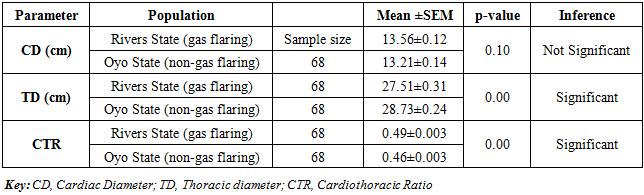
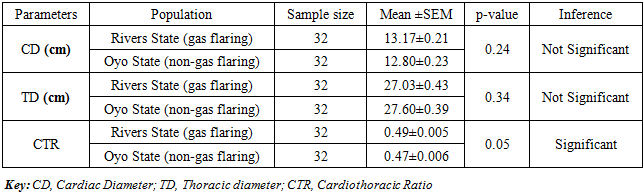
- The study has investigated the CTR of residents of gas flaring and non-gas flaring communities of Rivers and Oyo States of Nigeria. The CTR of residents of gas flaring areas were significantly higher than those in non-gas flaring areas. Several studies have determined the normal CTR of Nigerians. Among non-hypertensive patients at university of Jos Teaching Hospital, the CTR was 0.462 and that there was no significant difference with respect to sex [14]. The CTR of Nigerians residents within Rivers state was 0.457 for males and 0.467 for females and with respect to gender, females had higher statistically significant CTR values [18]. Assessment of fresh graduates of University of Jos showed that the CTR was 0.46 [17]. These findings are in line with our study of residents in non-gas flaring areas where the CTR was 0.46 for males and 0.47 for females, but contrary to residents of gas flaring area which had CTR of 0.49 for males and females respectively. The high CTR of residents of gas flaring communities could be attributed to environmental pollution caused by this activity as several studies have identified flared gas as the major source of air and water contamination [19,20,21,22] Flared gas releases into the environment particulate matter in form of soot, volatile organic compound (VOCs), and Polycyclic aromatic carbon (PAHs) [6,7,23].Epidemiological studies associating long and short-term effects of particulate matters with cardiovascular diseases are well documented [24,25,26,27,28,29,30,31,32]. It was reported by World Health Organization that air pollution was responsible for 3.7 million deaths in 2012 out of which 29% died of heart disease and stroke. In the United States, the risk of death due to cardiovascular disease increased with every increase in particulate matter [24]. But how does polluted air cause heart diseases? The American Heart Foundation (AHA) explained that air pollution affect cardiovascular system directly by altering the central nervous system function and indirectly by effects mediated by pulmonary inflammation and oxidative stress that eventually lead to systemic inflammatory response [31]. The Physicians for Social Responsibility also noted that particulate matters have the ability to block the heart arteries, the finer they are, the more ability they possess to permeate the cardiovascular system and one major effect of arterial blockage is increase in the blood pressure and work over-load on cardiac tissues [33,34,35,36]. Research showed that for every 10.5 µg/ m3 10 in the level of PM2.5, there was a 2.8 mmHg increase in systolic blood pressure and 2.7 increase in diastolic blood pressure disturbances in heart rhythm [37]. Volatile organic compounds (VOCs) are major constituents released from combustion of fossil fuel and the quantity is very high in communities where gas is flared [1]. The composition of VOCs varies with where the petroleum gas is tapped, it includes alkane (paraffin), cycloalkanes (napthenes), aromatics, non-hydrocarbons gases (CO2, H2, S2 SO2, He) etc [38]. These chemicals are regarded as noxious pollutants and can adversely affect pulmonary and cardiovascular functions, heart rate variability and induce oxidative stress. A study has showed that occupational exposure to VOCs increases serum C-reactive protein (CRP) and oxidative DNA adduct 8-hydroxy-2-deoxyguanosine (8-OHdG) levels and decreased heart rate variability indices [39]. CRP is a homopentameric acute-phase inflammatory protein used as a clinical maker of inflammation. Elevated level of these proteins is a strong independent predictor of cardiovascular disease in asymptomatic individuals [40.41]. 8-OHdG is a biomarker of deoxyribonucleic acid (DNA) damage due to oxidative stress. Heart rate variability has been described as a physiologic phenomenon of variation in the time interval between heart beat and it is used to diagnose cardiovascular diseases such as congestive heart failure, myocardiac infarction, coronary heart disease, hypertension etc. Increase in HRV is an indication of healthy autonomic and cardiovascular response while a decrease indicates that the sympathetic and parasympathetic nervous system isn’t properly coordinating to provide appropriate heart response [42].It is important to note the average CTR of residents in gas flaring communities was not above 0.5 because of the inclusion criteria of this study, as patients diagnosed with any form of cardiovascular anomaly, cardiomegaly inclusive were excluded from the study. Increased Cardiac diameter according to several authors reflects a number of pathological processes that affect cardiovascular function and outcome such as left ventricular hypertrophy, dilation and remodelling [43,44]. Since cardiac diameter has been shown to significantly correlate positively with CTR, it therefore implies that an increase in CD will result in increase in CTR and vice-versa [17,15]. It has been observed that individuals with small increases in cardiac size (48–55%) were associated with a 3-fold risk of death, rising to 8-fold when the CTR exceeded 55% in adults after tetralogy of Fallot repair [45].
5. Conclusions
- In conclusion, the borderline CTR of residents in gas flaring communities of in this study suggest a high risk of susceptibility to cardiovascular disease by this group. The exposure to gas flaring could lead to increase in cardiothoracic ratio.
ACKNOWLEDGEMENTS
- We sincerely appreciate Kenny Oyeranmi, University of Port Harcourt Teaching Hospital, University College Hospital (UCH) Ibadan, Orange Diagnostic Medical Center Port Harcourt and Image Diagnostics Port Harcourt, and Two Tees X-ray Center Ibadan for allowing us to use their facilities for this research.