-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2020; 10(4): 269-272
doi:10.5923/j.ajmms.20201004.21

Respiratory Viral Infections in the Formation of Left Atrial Standing and Its Early Diagnostics
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLBaratova M. S.
Bukhara State Medical Institute, Uzbekistan
Correspondence to: Baratova M. S., Bukhara State Medical Institute, Uzbekistan.
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

To study the role of respiratory viral infections in the formation of staning of the left atrium and its early diagnosis. 157 patients were examined, average age - 39.5 ± 4.8 years, men 98 people (63%), women 59 people (37%). All subjects were divided into 3 groups: 1 group — persons who had a mild form of myocarditis (n = 63); Group 2 - people who have had a complicated form of myocarditis (n = 75); Group 3 - persons who had a complicated form of myocarditis (n = 19).
Keywords: Influenza, Respiratory viral infections, Cardiovascular diseases, Myocarditis, Complications
Cite this paper: Baratova M. S., Respiratory Viral Infections in the Formation of Left Atrial Standing and Its Early Diagnostics, American Journal of Medicine and Medical Sciences, Vol. 10 No. 4, 2020, pp. 269-272. doi: 10.5923/j.ajmms.20201004.21.
Article Outline
1. Introduction
- Influenza and ARVI account for 95% of all infectious diseases in the world. Influenza epidemics annually affect from 7% to 15% of the world's population. About 50 million cases of infectious diseases are recorded in the Russian Federation, among which the bulk (90–95%) are influenza and ARD [2,3].In the republics of Central Asia, the incidence of influenza and SARS is about 26.7%. According to the WHO, influenza takes the 1st place among the causes of death from viral infections. So, in 2005, the number of deaths from influenza and pneumonia amounted to 3.87 million cases [WHO, 2005].At the same time, the proportion of deaths from respiratory viral infections caused by myocarditis in 8.73 million cases is growing. Despite the pronounced tendency to a decrease in the overall mortality from influenza and other respiratory viral infections in recent years, especially among people of middle and working age, it remains quite high and has signs of growth. Every year, tens of thousands of people die in different countries, mainly children of the first years of life (up to 2 years old) and elderly people (over 60 years old). Mortality among people 5-19 years old is 0.9, people of average working age 62.0, among people over 65 years old - 103.5 [5,10].For a long time, information on the prevalence of myocarditis was obtained only from autopsy studies. In particular, using the results of 40 thousand autopsies, I. Gore and O. Shaphir demonstrated that myocarditis can cause 3.5% of deaths associated with infectious and toxic diseases [1]. Further pathological studies conducted at the Bellevue Hospital (USA) confirmed that inflammatory myocardial damage in infectious diseases can occur in 3.3–7.8% of cases [2].An analysis of the data of a pathomorphological study of deaths from cardiovascular diseases revealed non-rheumatic myocarditis in 4–9% of cases [7]. Inflammatory myocardial diseases in 8.5% of cases are the cause of sudden death, and in a population under 35 this figure can reach 15% [8,11]. However, autopsy studies do not provide a true picture of the incidence of myocarditis. And only thanks to the introduction of intravital morphological diagnostics, it was possible to prove that recently developed heart failure (HF) in 49.6% of cases has an inflammatory nature [9].A variety of adenovirus serotypes, special biological properties of the pathogen, environmental stability and the ability to persist in the human body determine the wide distribution, polymorphism of clinical manifestations, and a tendency to a long and recurrent course [7]. There is evidence of the involvement of adenoviruses in the development of lower respiratory tract infections - bronchitis, pneumonia, myocarditis and pericarditis [5,6].In the medical literature, hibernating myocardium is understood as the state of the heart, which characterizes the inhibition of pumping function at rest without cardiomyocyte cytolysis, the cause of which is a decrease in the volumetric velocity of blood flow through coronary arteries [8,9].The state of the hibernating myocardium is the result of a protective reaction aimed at reducing the high ratio between the force of contraction of the hypoxic part of the heart muscle and its blood supply. Thus, hibernation delays the cytolysis of heart cells due to hypoergism. Stanning (English stunning - stunning, stunned) of the left atrial myocardium as a condition of those who experienced hypoxia in the segments of the walls of the heart chambers after an infectious and respiratory disease [10,11].Increased migration, physical activity, meteorological conditions, psycho - emotional stress, changes in the nature of food and accommodation affect the premorbid state of people of middle and working age, which can lead to a severe course of diseases [4].The lack of common ideas about clinical and laboratory diagnostics, the relative inefficiency of traditional methods of non-specific prophylaxis, the low effectiveness of modern ARVI treatment regimens for adenoviral etiology and adenoviral diseases and their complications in the cardiovascular system determine the need for additional research and early diagnosis of complications.
2. Aim of the Study
- Analysis of the role of respiratory viral infections in the formation of staning of the left atrium and its early diagnosis.
3. Materials and Methods
- 157 patients were examined, average age - 39.5 ± 4.8 years, men 98 people (63%), women 59 people (37%). All subjects were divided into 3 groups: 1 group — persons who had a mild form of myocarditis (n = 63); Group 2 - people who have had a complicated form of myocarditis (n = 75); Group 3 - persons who had a complicated form of myocarditis (n = 19).A standard examination was conducted to stratify risk: risk factors affecting the prognosis (burdened heredity, dyslipidemia, smoking, obesity, diabetes mellitus, glycemia), echocardiography, 12-lead ECG, ultrasound of the carotid arteries were analyzed. In addition, the following parameters were analyzed by ECG: duration of P wave, P wave height and type of P wave, inside atrial impulse delay, rhythm disturbances - atrial and ventricular extrasystoles, PQ interval, Q wave width, Q wave depth, R wave height, tooth depth S, localization of the transition zone, width of the QRS complex, presence of AV block, SA block, presence of impaired conduction along the legs of the bundle of His, period of internal deviation (QR), signs of sinus node dysfunction, Morganne-Edem-Stokes syndrome, s interval QT, the amplitude of the T wave, localization and its ST segment deviations (depression, shape, early repolarization).A standard echocardiography with a determination of the left ventricular mass index, as well as the relative thickness of the posterior wall of the left ventricle and interventricular septum, allows characterizing the geometry of the left ventricle, diffuse thickening of the myocardial walls due to interstitial edema, size of the left atrium, volume of the left atrium, peak velocity of the early and late diastole streams. When assessing the geometric structure of the left ventricle in B-mode, the thickness of the front, septum, posterior and lateral walls of the left ventricle into the diastole was measured from parasternal access along the short axis at the level of the valves of the MK and papillary muscles. Anterior - posterior size of the papillary muscles was determined from the position of the short axis of the left ventricle in the parasternal projection. In the M-mode, the thickness of the LV and the posterior wall of the LV in diastole, KDR and KSR of the LV, the anterior - posterior size of the LV, in the 4th projection, 2nd projection, was measured.Diagnoses were verified on the basis of modern clinical instrumental and laboratory research methods.Statistical processing of the work material was carried out by traditional methods of variation statistics. When organizing and conducting research, the principles of evidence-based medicine were observed.
4. Results and Discussions
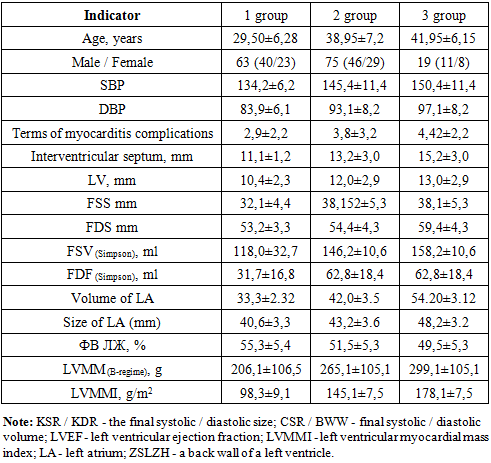
- ECG changes were diagnosed in the first group of 40.1% of cases, in the 2nd group of 47.7% of cases and in the 3rd group of 12.1% of cases, risk distribution: risk 1 - 55 people (35.1%), risk 2 - 46 people (28.6%), risk 3 - in 56 people (33.2%), risk 4 - in 5 people (4.1%). All changes in the analyzed ECG parameters revealed 48.0% of cases. The following were most often identified: displacement of the transitional zone - transitional zone - V4-5 - 13 people (8.2%), V2 - 14 people (8.9%), V5 - 7 people (4.5%), incomplete blockade of the right bundle branch block - 19 people (12.2%), intraventricular conduction disturbance - 25 people (15.9%), ventricular extrasystole - 16 people (10.3%), early repolarization of the ST segment - 48 people (30.5%), atrial fibrillation -12 people (7.6% ), Blinking-Edems-Stokes syndrome - 3 people (1.9%).In the study of echocardiography, myocardial hypertrophy was often observed along the interventricular septum of the middle section at 1.09 to 1.12 cm in 49 people (34.4%), the basal section at 1.12-1.14 cm in 28 people (18.3%), the anterior section from 1.14 -1.21 cm - in 62 people (36.3%), 1.21-1.3 cm in the interventricular septum and posterior wall - in 18 people (11.9%). According to our study, myocardial hypertrophy in patients of the 1st group was observed in 7 people (10%). No changes in the myocardium were observed. In the middle section, 18 people (29%), the basal section, 28 people (45%), and the anterior-apical section, 10 people (16%), respectively. And in patients of the 2nd group, the ratios were distributed as follows: in the median 21 people (28%), basal 30 people (39%), antero-apical 11 people (15%), hypertrophy of the interventricular septum and posterior wall (concentric type) in 13 people. (18%).In patients of group 3, in the middle section of MJP in 5 cases (26%), in the basal in 3 (16%), in the anterior - apical in 4 (21%), and in MJP and the posterior wall in 7 (37%). An increase in heart size was observed in all studied groups. Early diagnosis of the study of temporary "stunned" - Eng. “Stuninig left atrium” included changes in the size of the left atrium in the 2nd and 4th chamber projection and the size determined by the length of the axis of the heart (Table 1). This allows us to conclude that with later reversibility, patients had increased activation of mediators of inflammation, the release of lysosomal enzymes, prostoglandins, kinins, myocardial hypoxia, with the formation of micronecrosis, which aggravate atrial function, resulting in increased pressure in the LP - leading to the initial signs heart failure.
|
5. Conclusions
- In young patients, an electrocardiogram of 39.5% revealed changes associated with left atrial stanning, leading to impaired intraventricular conduction, early repolarization syndrome, and heart rhythm disturbance (tachycardia, extrasystole).It is noted that frequent remodeling leads to hypertrophy of certain parts of the myocardium, and in 31.5% of cases there is a concentric type of hypertrophy, which is considered the most unfavorable in the prognostic plan, which requires more careful observation of this category of patients.The examined patients showed early signs of diastolic dysfunction of the left ventricle, while in patients after an infectious respiratory disease, diastolic dysfunction is predominantly represented by hemodynamic disturbances and early left atrial stunning (67%).