-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2020; 10(4): 201-203
doi:10.5923/j.ajmms.20201004.05

Clinical and Laboratory Characteristic of Crypto-Cock Meningitis in HIV-Infected Patients
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLM. M. Bakhadirkhanov, R. I. Kasimova
Republican Research Centre of Emergency Medicine, Institute of Virusology, Tashkent, Uzbekistan
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

One of the most common forms of invasive mycoses in human immunodeficiency virus (HIV) infection is cryptococcal infection. Cryptococcosis is usually subacute meningitis or meningoencephalitis with fever, malaise and headache in HIV-infected patients. The aim of the study was to assess the clinical course of cryptococcal lesions of the central nervous system. The diagnosis was confirmed by isolation of cryptococcus from cerebrospinal fluid by the method of polymerase chain reaction. 10 patients with cryptococcal meningitis were observed. Analysis of the study results revealed the peculiarities of cryptococcosis course in HIV-infected patients.
Keywords: HIV-infection, Cryptococcus, Meningitis, Clinic, Diagnostics
Cite this paper: M. M. Bakhadirkhanov, R. I. Kasimova, Clinical and Laboratory Characteristic of Crypto-Cock Meningitis in HIV-Infected Patients, American Journal of Medicine and Medical Sciences, Vol. 10 No. 4, 2020, pp. 201-203. doi: 10.5923/j.ajmms.20201004.05.
1. Introduction
- Invasive mycoses have begun to occupy a special place among all infectious diseases for recent decades. Cryptococcal infection is one of the most common forms. HIV infection is the most important risk factor for this disease. According to the AIDS Clinical Research Unit (New York, USA), cryptococcal meningitis is the most common disease worldwide for people with HIV infection [1]. Studies show that almost 1 million cases of cryptococcal meningitis are diagnosed every year worldwide and a mortality rate makes up over 600,000 [2]. The morbidity has significantly decreased with effective anti-retroviral therapy (ART) and most new cases are found in patients with newly diagnosed HIV infection. [3].The incidence of cryptococcal infection among people living with HIV (PLHIV) in the United States is low. Among HIV-infected patients with CD4 ≤100 cells / μl, the prevalence of cryptococcal antigenemia was 2.9% and the prevalence was 4.3% among patients with CD4 ≤50 cells / μl [4]. There are no data about cryptococcosis morbidity in Uzbekistan.Cryptococcosis is usually sub-acute meningitis or meningoencephalitis with fever, malaise and headache in HIV-infected patients. Classical meningeal symptoms and signs occur only from one quarter to one third of patients. Some patients have symptoms of encephalopathy, such as lethargy, altered consciousness, personality changes and memory loss. Cryptococcosis can be diagnosed using a culture method, cerebrospinal fluid microscopy (CSF) or cryptococcal antigen detection (CrAg). PCR has been increasingly used for diagnostic purposes for recent years and its value is in establishing a diagnosis in the shortest time.Aim of the study was to evaluate the clinical course of cryptococcal lesion of the central nervous system in HIV-infected patients.
2. Material and Methods
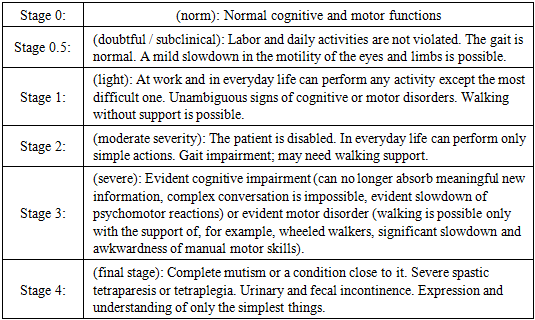
- 10 patients with cryptococcal meningitis admitted to the Republican Research Centre of Emergency Medicine were observed. Patients were sent to the hospital with primary diagnoses: acute cerebrovascular accident, acute meningoencephalitis, HIV-encephalopathy. In 6 (60%) patients HIV infection was first detected during examination. The remaining patients, knowing about their status, did not undergo examination and did not take ART. The average age of the patients was 39.2 years (19-59). There were 2 (20%) women and 6 (60%) men.Cerebrospinal fluid, in which cryptococcus was isolated by PCR served as the study material for confirming the diagnosis of cryptococcal meningitis. The severity of the clinical and functional severity of neurocognitive and motor disorders in patients was evaluated by the Memorial-Sloan-Kettering scale (Price 1988) (Tab.1).
|
3. Results and Discussion
- At admission, the condition of the patients as severe and extremely severe was detected in 7 (70%) patients who corresponded to stages 3 and 4 by the Memorial-Sloan-Kettering scale. Complete mutism or a state close to it, evident spastic paresis and understanding only the simplest things were observed in 5 (50%) patients.At admission, patients or their relatives complained of severe headache, nausea, vomiting, dizziness, unstable gait observed before admission, four patients noted visual disorder (double vision), cough. The severity of the condition was due to evident intoxication and cerebral symptoms. In 9 (90%) patients meningeal symptoms (stiff neck, Kernig, Brudzinsky symptoms) were revealed, in one patient meningeal symptoms were negative. Convultions were observed in 5 (50%) patients, dysfunctions of the pelvic organs were revealed in 7 (70%) cases (Fig. 1).
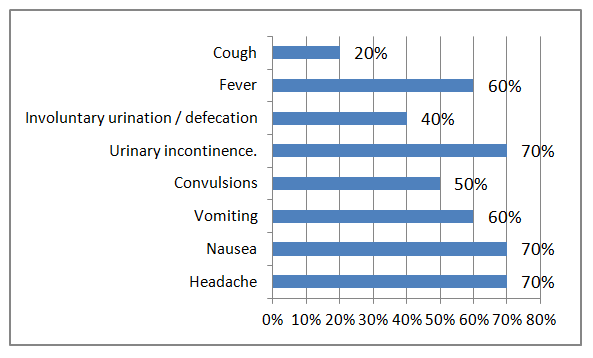 | Figure 1. Complaints of patients with cryptococcal meningoencephalitis |
4. Conclusions
- Cryptococcal meningitis in HIV-infected patients is observed at evident immunodeficiency (a decrease in CD-4 lymphocytes of less than 100 cells / μl) and is characterized by a severe progressive course with high mortality in the first month of therapy. In 40 (40%) patients HIV infection was first detected at the time of the examination - CNS lesion by cryptococcosis was the primary manifestation of HIV. Modern diagnostics of CNS lesions in HIV should include a study on cryptococcosis of patients with CD-4 lymphocytes of less than 100 cells / μl.