-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2020; 10(4): 187-191
doi:10.5923/j.ajmms.20201004.02

The Impact of Electrical Coagulation on the Operation of ECS in Patients with Acute Pathologies in Abdominal Cavity
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLD. A. Alimov, S. N. Salakhitdinov, B. S. Alimkhanov, S. A. Akilova
Republican Scientific Center of Emergency Medical Help
Correspondence to: D. A. Alimov, Republican Scientific Center of Emergency Medical Help.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The objective: In the article we reviewed characteristics and frequency of cardiac rhythm disorders, safety of electrical coagulation performance in mono polar mode during various non-cardiological surgical interventions in patients with earlier implanted electrical cardiac stimulators (ECS). Data and research methods: We studied the factors most often leading to disorders in the operation of ECS during non-cardiological surgical interventions in various terms after implantation of the stimulator in 56 patients in the age from 53 to 84 years old in the units of general surgery, traumatology, and vascular surgery of the RSCEMH. Besides that, measures for the prevention of these disorders were observed. Cardiac activity during surgical interventions was assessed with the help of cardiomonitor. Results: In 8.9% of the patients we registered dysfunction of ECS such as ineffective stimulation, stimulus inhibition, and temporary change in the stimulation mode. Conclusions: The study showed, that application of electric coagulation in mono polar mode was the most often cause of intra operative complications linked with the work of ECS and duration of a single impact of electric coagulator within different surgical operations.
Keywords: Coagulation mono polar mode, Continuous electric cardiac stimulation, Electric coagulation, Cardiac rhythm disorders
Cite this paper: D. A. Alimov, S. N. Salakhitdinov, B. S. Alimkhanov, S. A. Akilova, The Impact of Electrical Coagulation on the Operation of ECS in Patients with Acute Pathologies in Abdominal Cavity, American Journal of Medicine and Medical Sciences, Vol. 10 No. 4, 2020, pp. 187-191. doi: 10.5923/j.ajmms.20201004.02.
- Disorders of rhythm and heart conductibility take the 4th place in the structure of cardiac vascular pathologies. In the modern time the basic method in the therapy of chronic bradyrhythmia is still implantation of a permanent electric cardiac stimulator (ECS). Implementation of ECS implantation into clinical practice significantly increased expectancy and improved quality of life of the patients with symptomic bradycardia. Within the last decade the range of indications to ECS implantation increased, due to which the number of patients with implanted artificial pace maker increased too [1,2].Among the patients applying for emergency and planned operations in abdominal cavity the portion of those with previously implanted ESC is equal to 1-2% [3]. There is data about successful surgical operations in patients with ECS [4-6]. The main reason for surgeons and anesthesiologists worries performing surgical interventions is the risk of ECS dysfunction development. In the foreign literature there is data about disorders in ECS work appearing in cases when during surgical interventions electric coagulation is used. Though the character, prevalence, danger, prevention methods, and treatment of possible complications of these disorders are rarely described in detail [1-7]. The objective of the research was to study the impact of electric coagulation on the function of cardiac stimulator during abdominal surgical operations in patients with acute pathologies in abdominal cavity with previously implanted electric cardiac stimulators (ECS).
1. Data and Research Methods
- In the RSCEMH within the period from 2015 to 2018 fifty-six surgical interventions were performed in the patients with various forms of acute abdominal pathologies with previously implanted artificial pace makers. The age of those patients varies from 53 to 84 years old, average 63.9±14.6 years old. There were 35 (55%) men and 25 (44%) women. Among the concomitant diseases 35.71% (20 patients) were taken by diabetes mellitus, 57.14% (32 patients) by arterial hypertension, 66.07% (37 patients) angina, and 50.0% (28 patients) by cardiac failure. For the assessment of cardiac activity during operations all patients had a record of electrocardiogram (ECG) on cardiomonitor with evaluation of the indicators of ECS operation during mono polar mode electric coagulation (EC). For the analysis of possible damaging effect of EC on cardiac tissue in the endocardial electrode fixation area 13 patients had tests of cardiotropic enzymes amount and assessment of ECG dynamic alterations at the 1st and 3rd days after the surgery. In all the cases during operations mono polar mode EC was used with 100 W capacity.
2. Discussion and Results of the Research
- All (100%) patients had successful emergency surgical operations without intra operation lethal outcome. In spite of the following all the safety rules some patients had registered ECS dysfunctions when electric coagulator was used. In two (3.6%) patients EC impact on ECS work was accompanied by periodic absence of stimuli at the moment of electric coagulation (figure 1).With the help of cardiomonitor with separated channel for the stimulator analysis and Medronic – a device programming cardiac stimulating coagulation in five (8.9%) cases we registered the following interactions of coagulator with cardiac stimulator. During EC two patients (3.6%) had ECS dysfunction, accompanied by temporary asystole (figure 1,2).In the photo №1 there is a part of cardiomonitor record where we can see that at the moment mono polar mode electric coagulation impact, indicated as Mm, there is registered asystolia of ventricles (4000ms-15imp/min) (intervals are indicated by a dotted arrow).
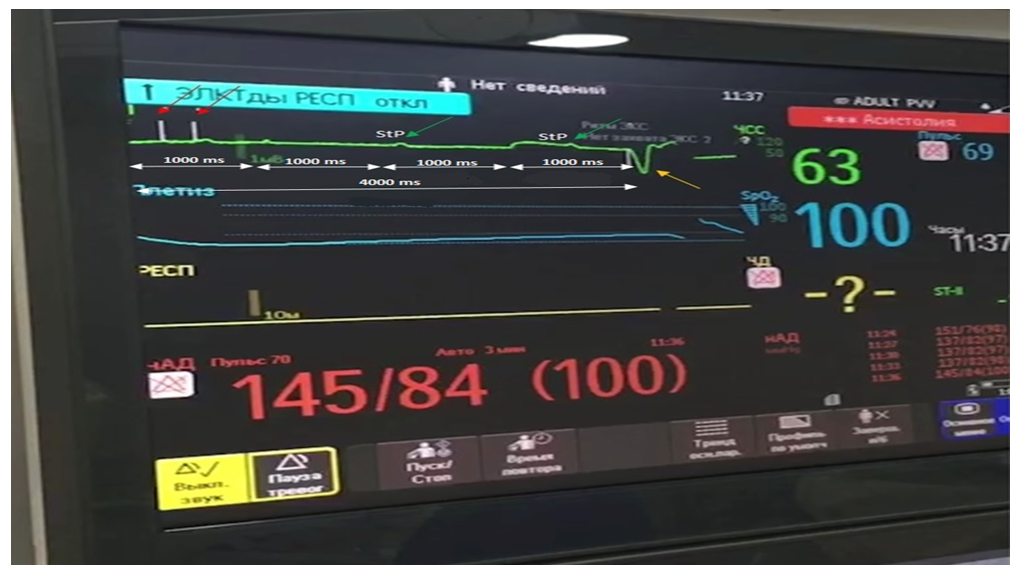 | Photo 1. Intra operation cardiomonitor. Biventricular mode of stimulation (DDD) with basic stimulation frequency equal to 60 imp/min at the moment of EC. Record speed is 50mm/sec, amplification 1mV = 10mm (explanation herein) |
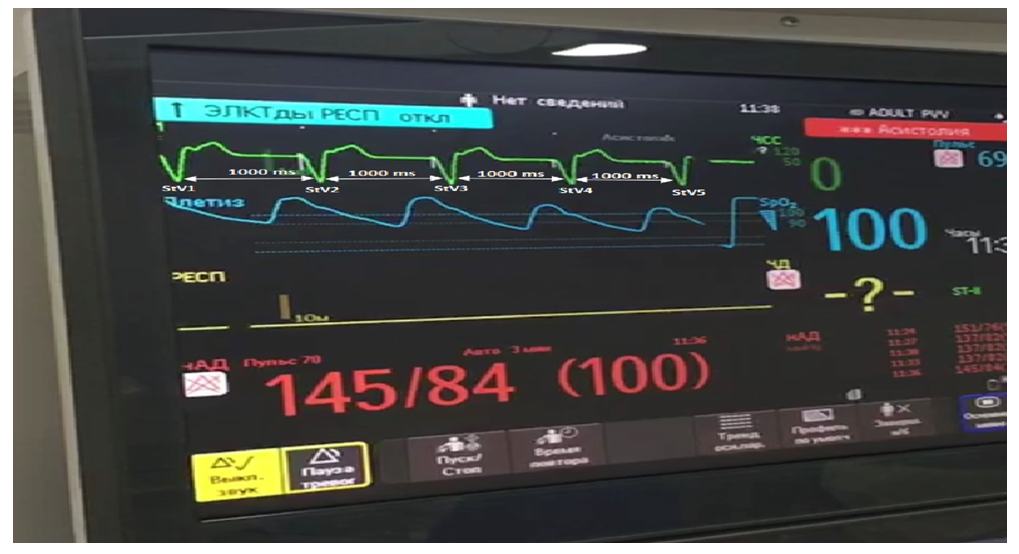 | Photo 2. Intra operation cardiomonitor. Double-chamber mode of stimulation (DDD) with basic stimulation frequency equal to 60 imp/min after EC. Record speed is 50mm/sec, amplification is 1mV = 10 mm (explanation herein) |
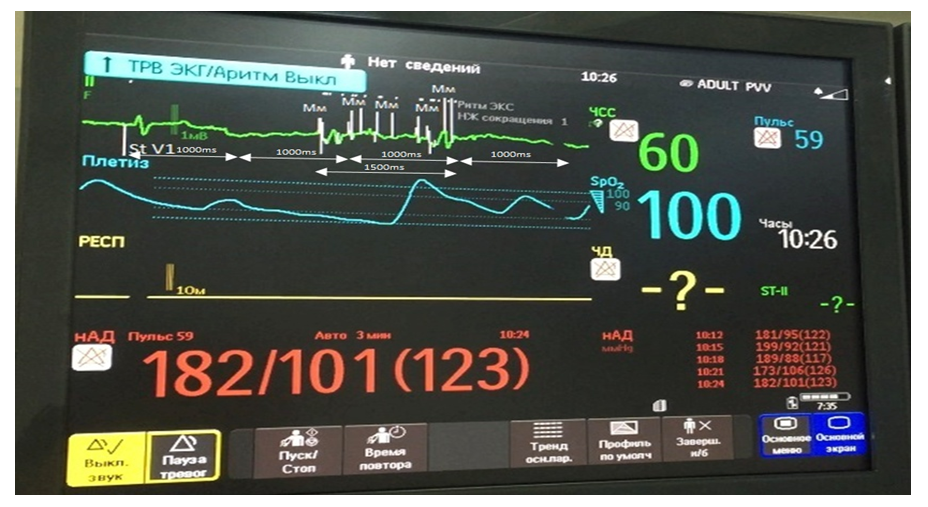 | Photo 3. Intra operation cardiomonitor. Double chamber stimulation mode (DDD) with basic stimulation frequency equal to 60 imp/min at the moment of EC application. Record speed is 50mm/sec, amplification is 1 mV = 10 mm (explanation is hereafter) |
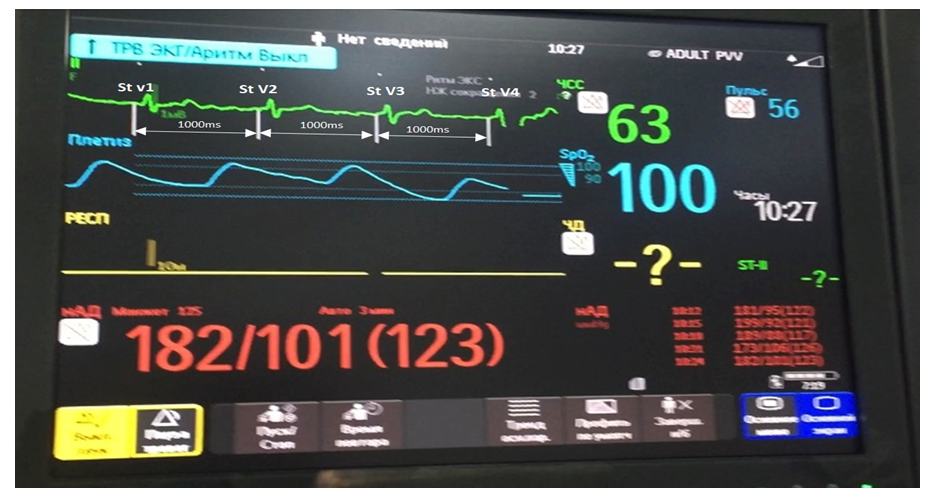 | Photo 4. Intra operative cardiomonitor. Double chamber stimulation mode (DDD) with basic stimulation frequency equal to 60 imp/min after EC application. Record speed is 5-mm/sec, amplification is 1 mV = 10 mm (explanation is hereafter) |
3. Conclusions
- Presence of ECS is not a counter-indication for the performance of surgery using electric coagulation in mono polar mode. Though 8.9% of the patients had development of disorders in ECS system such as stimuli inhibition, ineffective stimulation, and temporary alteration of stimulation mode. Stimulator-dependent patients should be operated with EC in conditions of specialized clinic due to minimal risk of ECS damage. The most often disorder developing under the influence of mono polar electric coagulation was ECS stimulus inhibition, appearance of which depended on the cardiac stimulator’s sensitivity polarity configuration. To diminish the risk of development of the aforesaid disorder it is rational to use bipolar mode sensitivity of electric cardiac stimulator. That disorder is dangerous in the group of stimulator-dependent patients. Short-term episodes of ineffective stimulation at the moment of electric coagulation are not so dangerous as rhythm disorders. In all cases of ECS operation disorders development short-term stop in electric coagulation should be done; in case of ineffective stimuli registration surgeons should quit EC application. The term of single electric coagulation application during operation in any patient with cardiac stimulator should not exceed 3 seconds. ECG characteristics in the work of electric cardiac stimulator can be registered independently of electric coagulation, set basic stimulation frequency, hysteresis function and other settings (including those due to myopotential inhibition). That is why during preoperative examination of a patient control testing of ECS system, and, if necessary, performance of special tests for the detection of these characteristics, should be done.