Nargiza Yarmukhamedova1, Erkin Musabaev2, Khalil Halimzianov3, Vera Vasil'kova4
1Head of Department of Infection disease, Epidemiology and Dermatovenerology Samarkand State Medical Institute, Republic of Uzbekistan
2Head of Scientific Research Institute of Virology Scientific Research Institute of Virology, Republic of Uzbekistan
3State Budgetary Educational Institution of Higher Professional Education «Astrakhan State Medical University» of the Ministry of Healthcare of the Russian Federation, Astrakhan, Russia
4Associate Professor of the Department of Infectious Diseases and Epidemiology, Federal State Budget Educational Institution of Higher Education "Astrakhan State Medical University" of the Ministry of Health of the Russian Federation, Astrakhan, Russia
Correspondence to: Nargiza Yarmukhamedova, Head of Department of Infection disease, Epidemiology and Dermatovenerology Samarkand State Medical Institute, Republic of Uzbekistan.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Rickettsiosis infection is widespread throughout the world. Many areas are natural foci of this infection, especially tick-borne rickettsiosis. To identify the characteristic and leading clinical criteria, the analysis of the most common rickettsioses in the territory of the Republic of Uzbekistan and the southern Federal district of the Russian Federation was carried out. This will allow to form clear indications for laboratory diagnosis, to identify the infection is not only endemic, but also imported for different regions.
Keywords:
Rickettsia, Fever, Tick-borne typhus, Astrakhan rickettsial fever
Cite this paper: Nargiza Yarmukhamedova, Erkin Musabaev, Khalil Halimzianov, Vera Vasil'kova, Clinical Aspects of Rickettsial Infection in the Southern Federal District of Russia and the Republic of Uzbekistan, American Journal of Medicine and Medical Sciences, Vol. 10 No. 3, 2020, pp. 161-165. doi: 10.5923/j.ajmms.20201003.07.
1. Introduction
Rickettsioses include an ever-expanding group of infectious diseases [1,2]. All rickettsioses according to the generally accepted classification are divided into 5 groups. The most significant of them by the number of nosologies is the group of tick-borne spotted fever [3,4,5].Representatives of this group are the etiological agents of a large number of new and emerging infectious diseases spread around the world [6,7,8,9]. These infections are zoonotic and are transmitted by arthropod carriers, mainly ticks, fleas, to hosts such as wild animals. Pets And Humans Are Occasional Hosts [10,11].Recently, there has been a significant increase in rickettsioses, which is characterized by a large-scale change in areas with a noticeable increase in spatial distribution. The restructuring of natural landscapes is observed in connection with the increasing anthropogenic impact, as a result of which the areas of distribution of natural focal diseases expand, covering new territories [12,13]. Locals in endemic areas, as well as travelers to these regions, are at high risk of infection. In addition, the expansion of international relations, population migration also contributes to the importation and spread of infection even in non-endemic territories [14,15].Rickettsioses have common clinical manifestations, such as fever, symptoms of intoxication, exanthema, lymphadenopathy. Some of these manifestations may suggest some types of Rickettsia infection. However, none of these manifestations is pathognomonic, and direct diagnostic methods are always required to confirm the species involved [16,17].This situation is applicable to rickettsioses, where different species can cause similar clinical manifestations.The early diagnosis of an infectious disease is based on the definition of a leading clinical syndrome complex and the sequential comparison of its manifestations. For natural focal infections of rickettsial etiology, the leading syndrome is fever, it is on it that differential diagnosis can be based. In this case, the characteristic of the fever is important - severity, duration, type of temperature curve [18,19]. In addition to the differentiation of fever and intoxication syndrome, organ lesions also play an important role in the diagnosis. For a correct diagnosis, a carefully assembled epidemiological history is also important [20].
2. The Objective of the Study
The foregoing has led us to compare the clinical and epidemiological picture of tick-borne rickettsioses in various natural foci using the example of the Samarkand region (RU) and the Astrakhan region (Southern Federal District of Russia). Identification of the main clinical criteria for the studied infections will allow us to suspect an imported infection due to the geographical and economic spread of rickettsioses.
3. Materials and Methods
On the territory of the Samarkand region, a laboratory examination of acute febrile patients was conducted and a group of 80 people was diagnosed with Tick-borne typhus (Typhoid fever). The diagnosis was verified by serological studies - an enzyme-linked immunosorbent assay was performed to identify specific IgM for a group of tick-borne spotted fevers, namely for tick-borne typhus (R. Sibirica).The territory of the Astrakhan region is a natural focus of rickettsiosis from the group of tick-borne spotted fevers - the Astrakhan rickettsial fever. A total of 145 patients were examined to study clinical symptoms. To verify the diagnosis: Astrakhan rickettsial fever (ARF) used the RNIF serological reaction with a specific antigen of the pathogen - R. conori, as well as PCR diagnostics.Table 1. The distribution of patients by age
 |
| |
|
Table 2. Epidemiological data
 |
| |
|
4. Research Results and Discussion
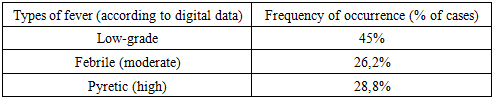
An increase in temperature was the first and one of the main symptoms of CCT. Observation of the nature of the fever made it possible to identify the characteristic temperature curves.Remitting fever was characterized by a daily fluctuation of more than 10°C and was observed in 46 patients (57.7%). In second place in frequency of occurrence was wave-like fever - in 22 patients (27.5%) - with a gradual increase in temperature to high numbers, and then gradually decreased to subfebrile numbers, and sometimes normal, and the formation of 2, 3 waves.The height of the fever is no less significant symptom in this pathology (table 3).Table 3. Characteristic of fever in Typhoid fever
 |
| |
|
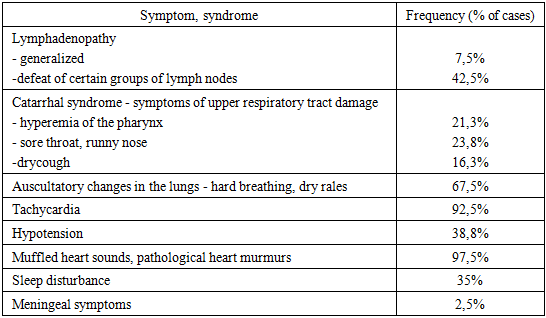
The average duration of fever in the observed patients was 16.05 ± 2.7 days, with fluctuations from 2 to 35 days.Against the background of elevated temperature, the following intoxication symptoms were registered in patients: headache - in 78 cases (97.5%), general weakness - in 40 (50.0%), dizziness - in 10 (12.5%) patients, pain in muscle - in 35 (43.8%), joints - in 21 (26.3%), body aches - in 47 (58.8%) patients and sleep disturbance in the form of insomnia in 28 (35.0%), decreased appetite in 78 (97.5%) patients, nausea and vomiting in 15 (18.8%) patients.The rash is a characteristic sign of Typhoid fever during the height of the disease. In our observations, exanthema was polymorphic in nature. Most often roseolous elements were noted. The rash appeared on the 2nd-5th day of the disease on an unchanged skin background, first on the extremities, and then spread throughout the body. In severe infections, hemorrhagic degeneration of exanthema was observed. On the 6-7th day, the rash passed into the pigmentation stage and regressed.Table 4. Clinical symptoms of Typhoid fever during the height of infection
 |
| |
|
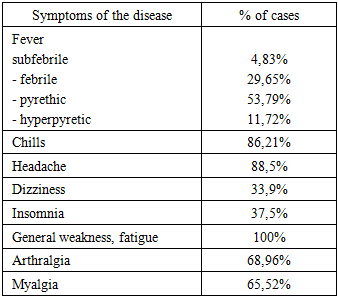
As can be seen from table 4, the peak period in Typhoid fever is characterized by a diverse lesion of organs and systems.Damage to the lymph nodes is characteristic. When analyzing the localization of lymphadenitis, a primary lesion was noted in the submandibular lymph nodes. In severe cases, generalized lymphadenitis was noted with a simultaneous increase in cervical, axillary and inguinal lymph nodes to 1.5-2.0 cm, painless on palpation.In almost all patients, lesions of the respiratory system of varying severity and localization were noted. In 7 (8.8%) patients, changes characteristic of pneumonia were revealed, manifested by respiratory failure syndrome, weakening of breathing with various wet rales, accompanied by cough with sputum.Changes in the cardiovascular system were pronounced, especially at the height of the disease. We have revealed in 78 (97.5%) patients muffling of cardiac sounds, systolic murmur at the apex. At the same time, one patient has infectious - toxic myocarditis, manifested on the ECG by myocardial hypoxia, left ventricular hypertrophy.The leading sign of central nervous system damage in the midst of the disease was headache in 78 patients (97.5%), while in most cases headache was common - in 73 (91.3%), the nature of the pain was different. So in 31 (38.8%) the pain was throbbing, dull in 22 (27.5%) cases, paroxysmal in 11 (13.8%) and constant in 9 (13.8%) patients. And in only some cases, the pain was localized in the temporal 3 (3.8%) and frontal 2 (2.5%) areas. The second most common symptom of central nervous system damage was sleep disturbance, manifested in the form of insomnia in 28 (35%) patients and sometimes in the form of intermittent superficial sleep with nightmare dreams and, in one case, delirium. In addition, 14 (17.5%) patients complained of increased fatigue. In severe cases, retardation, confusion, and also meningeal signs in the form of stiff neck and positive symptoms of Kernig and Brudzinsky were observed in 2.5% of cases. In these patients, serous meningitis was diagnosed in the study of cerebrospinal fluid.Clinical and anamnestic study of symptoms in 145 patients showed that ARL is an acute infectious disease, during which 4 periods can be distinguished - incubation, initial, high and convalescence.The incubation period, fixed by bite or tick detection, ranged widely from 2 days to 1 month, averaging 9.38 days.Table 5. Clinical symptoms of the initial period of ARF
 |
| |
|
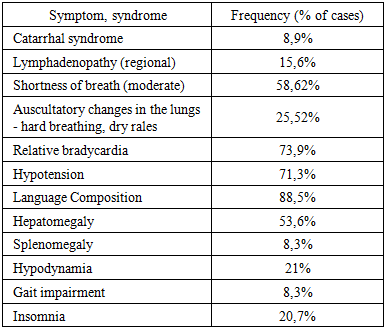
The earliest symptom of ARL, which forms even before the onset of the temperature reaction, is the primary affect at the site of bites by infected tick rickettsia. On examination, affects were found on the skin of 37 patients, mainly on the lower extremities, especially the legs, less often the body, head and upper limbs were affected.The duration of the initial (pre-ekzematous) period ranged from 2 to 6, on average - 4 days. Its development was determined by the appearance of fever with severe chills.From the first days of the disease, body temperature was recorded at high numbers and was mostly - 68% - remitting, rarely constant. The duration of the fever varied depending on the severity - from 5.4 to 15.36 days. In most patients with moderate severity, the average duration of the febrile period was 9.05 days. Along with an increase in temperature, the observed patients had symptoms of intoxication of varying severity.At 2–9 days of fever in all patients - 100% of the cases - there was a simultaneous appearance of an abundant skin rash with widespread distribution. Polymorphic exanthema in the form of spots, roseola and papules was recorded on the trunk - 100%, on the face - 39.1%, limbs - arms 98.9%, legs 100%, palms - 34.9% and soles - 43.2%. The edges of the rash elements were clear, spots in size ranged from 2-3 to 5-7 mm in diameter, papules from 3-5 to 10 mm in diameter, and the elements of the rash could be of different sizes in the same patient. In some patients - 41.7% in the center of the elements of the rash, hemorrhages were noted, most often small-pointed. The rash was kept depending on the duration of the fever (9-12 days, sometimes longer - 15-17 days). The average duration of exanthema was 12.7 days. Almost half of the patients had pigmented spots on the site of the rash. Often, before the appearance of exanthema, patients revealed conjunctival hyperemia and pinpoint rashes on the mucous membrane of the oropharynx.The appearance of a rash in patients with ARF marked the beginning of a period of high disease. At the same time, there was an increase in fever, as well as organ lesions as a result of the direct action of the pathogen ARF or its metabolic products on the human body.Table 6. Clinical Symptoms of ARF during High
 |
| |
|
Analysis of the clinical symptoms of ARF during the height of the infection showed a pronounced toxic effect of rickettsia on the human body.The defeat of the respiratory system in the acute period of ARF in most cases was weakly expressed and, masking itself among the general infectious manifestations of the disease, manifested itself mainly by moderate shortness of breath.From the side of the heart, a moderate expansion of the borders and a muffling of tones in 56.8% were noted. In most patients - 73.9%, relative bradycardia was observed, and in 26% of patients the pulse corresponded to fever during the first and beginning of the second week of illness (92-98-110 beats per minute).Symptoms of the gastrointestinal tract in ARF were nonspecific and generally emphasized the severity of intoxication syndrome. Most often, these were complaints about a decrease in appetite. Nausea was noted in every tenth case of ARF. In isolated cases, patients experienced vomiting - single or double - against the background of a severe course of the disease.Almost all patients with ARF complained almost simultaneously with an increase in temperature, reflecting the paretic state of the vessels of various parts of the nervous system: general weakness, feeling of heat and thirst, headache, decreased appetite, as well as complaints of joint and muscle pain. All these phenomena progressively increased in 2-4 days: excruciating fever, refusal to eat due to anorexia, a general breakdown and intense arthromyalgia forced patients to go to bed, leading to physical inactivity - 21% up to a complete immobility of patients - 9.8% . Headache increased very quickly, which in some people became so pronounced that insomnia developed within 5-7 days (20.7%) or, conversely, drowsiness - 4.1% of cases. Headache usually had a diffuse character, without a clear localization - 68.9%. If in the initial period of ARF, headache dominated, then in the midst of the disease, myalgia and, primarily, pain in the calf muscles, which along with dizziness caused a shaky gait, dominated in terms of intensity of the disease - 8.3% of cases. The pain syndrome, gradually dying away within 8-11 days, usually resolved in 1-2 days of normal temperature.The analysis of the clinical picture of rickettsioses in various endemic areas showed the predominance of the toxic effect of rickettsia from the group of pathogens of tick-borne spotted fevers on the human body. First of all, the result of this action was the presence of fever of a pyrethic nature and severe symptoms of intoxication in both studied infections. However, with different nosologies, we see the specific effect of each pathogen. Thus, clinical observations of patients with ARF and Typhoid fevershowed the predominant effect of the pathogen of ARF - conori rickettsia on the endothelium of the skin vessels, which was manifested 100% by a sign of this infection - abundant disseminated exanthema. The causative agent of Typhoid fevershowed a predominant effect on the lymphatic and cardiovascular systems, which was clinically manifested by lymphadenopathy and toxic myocardial lesions in almost every patient with a diagnosis of Typhoid fever.
5. Conclusions
1. Examination of patients with Typhoid fever allowed us to identify the following criteria for this rickettsiosis for the clinical diagnosis:- pyretic and hyperpyretic fever with prevalence of remitting type of temperature curve- of the symptoms of intoxication, the predominance of headache, insomnia- lymphadenopathy, in severe cases of a generalized nature- polymorphic rash on the limbs and trunk, without damage to the palms and soles, a possible phenomenon of rash- characteristic changes in the cardiovascular system, indicating toxic myocarditis- the appearance at the height of the disease in isolated cases of meningeal symptoms with lymphocytic pleocytosis.2. Clinical and diagnostic criteria for ARFare- pyrethic fever with a characteristic remitting or constant type of temperature curve;- severe intoxication syndrome without the development of typhoid status;- severe arthralgia and myalgia, sometimes with impaired gait;- the presence of primary affect, mainly on the lower extremities, sometimes in combination with regional lymphadenitis;- copious polymorphic, without the tendency to fusion of exanthema in all patients - roseola, transforming into papules and hemorrhages;- frequent localization of the rash on the palms and soles;- epidemiological history data - spring - summer season, stay in a natural focus, an indication of finds and tick bites.3. The highlighted clinical criteria for the diagnosis of tick-borne rickettsioses will not only detect the infection in endemic areas, but also identify cases of imported infection due to the expansion of international relations, population migration and the development of tourism.
References
| [1] | Abdad MY, Abou Abdallah R, Fournier PE, Stenos J, Vasoo S.A Concise Review of the Epidemiology and Diagnostics of Rickettsioses: Rickettsia and Orientia spp. // J ClinMicrobiol. 2018 Jul 26; 56(8). |
| [2] | Blanton LS. The Rickettsioses: A Practical Update. // Infect Dis Clin North Am. 2019 Mar; 33(1): 213-229. |
| [3] | Portillo A, Santibáñez S, García-Álvarez L, Palomar A.M., Oteo J.A. Rickettsioses in Europe. //Microbes Infect. 2015 Nov-Dec; 17(11-12): 834-8. |
| [4] | Brouqui P, Parola P, Fournier P.E., Raoult D. Spotted fever rickettsioses in southern and eastern Europe. // FEMS Immunol Med Microbiol. 2007 Feb; 49(1): 2-12. |
| [5] | Kasimov S. et al. haemosorption In Complex Management Of Hepatargia: o27 (l1-1) //The International Journal of Artificial Organs. – 2013. – Т. 36. – №. 8. |
| [6] | Parola P, Paddock C.D., Socolovschi C, Labruna MB, Mediannikov O, Kernif T, Abdad MY, Stenos J, Bitam I, Fournier P.E., Raoult D. Update on tick-borne rickettsioses around the world: a geographic approach. // Clin Microbiol Rev. 2013 Oct; 26(4): 657-702. |
| [7] | Dedkov V.G., Simonova E.G., Beshlebova O.V., Safonova M.V., Stukolova O.A., Verigina E.V., Savinov G.V., Karaseva .I.P., Blinova E.A., Granitov V.M., Arsenjeva IV, Shipulin G.A. The burden of tick-borne diseases in the Altai region of Russia.// Ticks Tick Borne Dis. 2017 Aug; 8(5): 787-794. |
| [8] | Rajoelison P, Mediannikov O, Javelle E, Raoult D, Parola P, Aoun O. Rickettsia sibirica mongolitimonae human infection: A diagnostic challenge.// Travel Med Infect Dis. 2018 Nov - Dec; 26: 72-73. |
| [9] | Rudakov N.V., Abramova N.V., Shtrek S.V., Shalamova E.V., Penyevskaya N.A., Rudakova S.A., Samoylenko I.E., Berezkina G.V., Zelikman S.Y., Kumpan L.V., Matushenko E.V., Naumkina E.V. Clinical and laboratory diagnosis of tick-borne rickettsioses in areas of low risk of infection Rickettsia sibirica. // Klin Lab Diagn. 2018; 63(11): 717-721. |
| [10] | Hidalgo M, Faccini-Martínez Á.A., Valbuena G. Tick-borne rickettsioses in the Americas: clinical and epidemiological advances, and diagnostic challenges. // Biomedica. 2013 Sep; 33 Suppl 1:161-78. Review. |
| [11] | Paris DH, Dumler JS. State of the art of diagnosis of rickettsial diseases: the use of blood specimens for diagnosis of scrub typhus, spotted fever group rickettsiosis, and murine typhus. //CurrOpin Infect Dis. 2016 Oct; 29(5): 433-9. |
| [12] | Erkin M. et al. The challenge of emerging and re-emerging infectious diseases in Uzbekistan: study of rickettsiosis using pcr diagnostic method //European science review. – 2018. – №. 5-6. |
| [13] | Jensenius M, Fournier P.E., Raoult D. Tick-borne rickettsioses in international travellers. // Int J Infect Dis. 2004 May; 8(3): 139-46. |
| [14] | Faccini-Martínez Á.A., García-Álvarez L, Hidalgo M, Oteo J.A. Syndromic classification of rickettsioses: an approach for clinical practice. // Int J Infect Dis. 2014 Nov; 28: 126. |
| [15] | Mamatkulov A. et al. Detection of Q-fever in Samarkand region of Uzbekistan: mite surveillance study //International Journal of Infectious Diseases. – 2019. – Т. 79. – С. 141. |
| [16] | Sekeyová Z, Danchenko M, Filipčík P, Fournier P.E. Rickettsial infections of the central nervous system. //PLoSNegl Trop Dis. 2019 Aug 29; 13(8). |
| [17] | Schibli A, Weisser M, Bingisser R, Widmer AF, Battegay M. Initial patient assessment of infectious diseases and diagnostic steps with fever // Internist (Berl). 2013 Aug; 54(8). |
| [18] | Soliman A. et al. Serological evidence of rickettsial infection among acute febrile illness patients in Uzbekistan //American journal of tropical medicine and hygiene. – 8000 Westpark DR, STE 130, MCLEAN, VA 22101 USA: AMER SOC TROP MED & HYGIENE, 2005. – Т. 73. – №. 6. – С. 79-80. |
| [19] | D'incau S, Lebowitz D, Toutous-Trellu L, Eperon G, Huttner B. Fever and rash in the adult patient // Rev Med Suisse. 2017 Apr 12; 13(558): 798-807. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML