-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2020; 10(1): 13-16
doi:10.5923/j.ajmms.20201001.04

Analysis of Complications and Causes of Lethal Outcomes at Acute Pancreatitis of Biliary Etiology
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLF. G. Nazirov, R. A. Ibadov, A. Kh. Babadjanov, B. R. Abdullajanov
Republican Specialized Scientific and Practical Medical Center of Surgery named after Academician V. Vakhidov, Tashkent, Uzbekistan
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The aim of the study is to improve the treatment outcomes of patients with acute pancreatitis by improving tactical diagnostic monitoring of specific pancreatogenic complications and optimizing the complex of therapeutic and preventive measures. Materials. The authors conduct a structural analysis of the main systemic pancreatogenic complications and causes of mortality at acute biliary pancreatitis in 438 patients from the total patients quantity and surgical treatment was performed in 25.6% (112 of 438) cases. Methods. The analysis of indicators was carried out by Ranson and APACHE II prognostic scales. Conclusion. The progression of biliary pancreatitis is characterized by the possibility of multicomponent development of various pancreatitis-associated systemic complications, against the background of which the mortality rate made up 11.4%. The main causal factors of an unfavorable prognosis in the structure of mortality were such manifestations of multiple organ failure as acute respiratory distress syndrome - 77.8% and renal failure - 48.1%, as well as septic manifestations - 33.3% and hemorrhagic complications - 11, one%.
Keywords: Pancreatitis, Multiple organ failure, Structural analysis of complications
Cite this paper: F. G. Nazirov, R. A. Ibadov, A. Kh. Babadjanov, B. R. Abdullajanov, Analysis of Complications and Causes of Lethal Outcomes at Acute Pancreatitis of Biliary Etiology, American Journal of Medicine and Medical Sciences, Vol. 10 No. 1, 2020, pp. 13-16. doi: 10.5923/j.ajmms.20201001.04.
1. Introduction
- In modern surgery of the hepatobiliary system, pancreatic diseases still remain an urgent socio-epidemiological and clinical issue of health care. For example, according to European gastroenterologists’ data, acute pancreatitis (AP) is a common cause of emergency hospitalization with a frequency of approximately 40 cases per 100,000 populations per year [1-6]. Two of the most common factors - biliary pancreatitis and an alcohol-alimentary form of the disease accounting for 70–80% of all cases are distinguished in the structure of etiological reasons. About 10-20% of acute pancreatitis are classified as severe, characterized by a high incidence of local purulent-necrotic and systemic pancreatogenic complications. In turn, mortality, despite the improvement of diagnostic methods, the use of modern methods of conservative and surgical treatment, remains high and varies in the range of 7.5-15.2% and at destructive forms reaches 40-70%. Hospital mortality in the first week after admission makes up 35-50%. There has been a slight decrease in mortality for recent years. Mortality rates remain high and reach up to 40-70%in the older age group, especially at destructive forms of severe acute pancreatitis [7-11].The development of AP severe forms is determined by two factors that reflect the severity of the disease: organ failure and pancreatonecrosis. About half of fatal outcomes cases in patients with severe acute pancreatitis (SAP) occur during the first two weeks and are mainly explained by multiple organ failure syndrome (MOFS), characterized by a systemic inflammatory response (SIR) and a high incidence of local purulent-necrotic and systemic pancreatogenic complications with variable degree of organs dysfunction [12-15]. Aim of study is to improve the treatment results of patients with acute pancreatitis (AP) by updating tactical diagnostic monitoring of specific pancreatogenic complications and optimizing the complex of therapeutic and preventive measures.
2. Materials and Methods
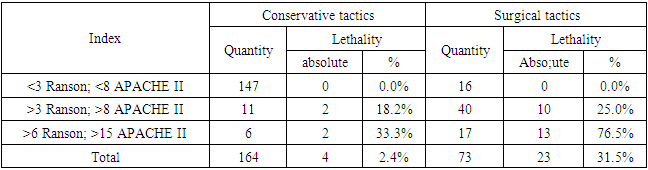
- A comparative analysis of 438 patients with acute pancreatitis (AP) of biliary etiology who were treated by the Republican Specialized Scientific and Practical Medical Center of Surgery named after academician V. Vakhidov and in the clinic of Andijan State Medical Institute for the period from 2009 to 2018 was carried out in this study. Surgical interventions were performed in 25.6% (112 from 438) cases. Patients were distributed according to the type of performed surgeries as follows: 5.9%, (26 of 438) - laparotomy, cholecystectomy (CCE), choledoch drainage, opening, sanation and stuffing box drainage; in 5.0% (22 from 438) cases - laparoscopy, drainage of the common bile duct according to Pikovsky, drainage of the omental bursa were performed; 4.8% (21 from 438) – laparotomy, necrosecestrectomy, drainage of the abdominal cavity and retroperitoneal space; 4.6% (20 from 438) - CCE, choledocholithotomy, drainage of the common bile duct, opening, rehabilitation and drainage of the stuffing box; 2.7% (12 from 438) patients had drainage of the stuffing box under ultrasound control; in 0.7% of cases - laparoscopy, laparotomy, drainage of the omental bursa and abdominal cavity. The choice of treatment tactics at biliary AP in favor of conservative intensive therapy was associated with an overall mortality rate of 2.4% (4 from 164 cases), while the use of surgical tactics in the early stages of the disease led to deaths in 31.5% (23 of 73) of cases (Tab. 1).
|
|
|
3. Results
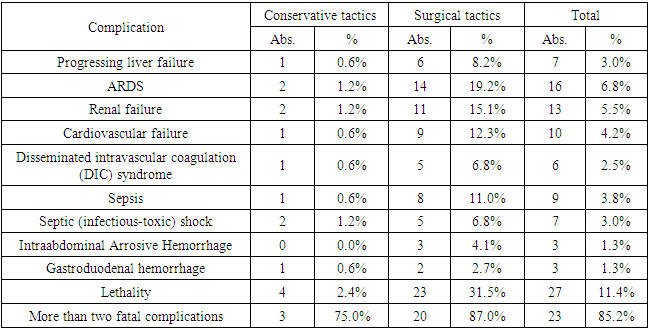
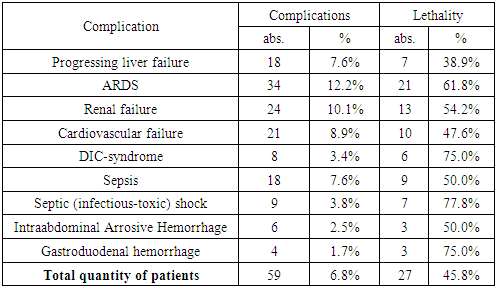
- Thus, the progression of biliary pancreatitis is characterized by the possibility of multicomponent development of various pancreatitis-associated systemic complications, against the background of which the mortality rate was 11.4% (with conservative tactics - 2.4%, with surgical interventions - 31.5%). In the structure of systemic complications, the main causal factors of an unfavorable prognosis were such manifestations of multiple organ failure (MOF) as ARDS - 77.8% (in 21 of 27 patients who died) and renal failure - 48.1% (13), as well as septic manifestations - 33.3% (in 9 patients) and hemorrhagic complications - 11.1%.
4. Discussion
- According to our data, the most common and significant systemic complication of severe AP is pancreatitis-associated ARDS, which is characterized by severe hypoxemia requiring the immediate use of respiratory support, and the progression of diffuse lesion of the lung tissue. In the framework of this research we studied the role of this fatal condition in the general structure of complications and causes of mortality at biliary AP.Early development was observed in 76.5% (26 from 34) cases from all cases of ARDS, in the structure of all APs early development of ARDS was observed in 11.0% (26 from 237), against the background of other complications - 3.4% (8 from 237) of cases (Fig. 1). In the structure of total mortality ARDS accounts for 6.3% (15 from 237) in the early stages of AP and 2.5% (6 from 237) in the late stages, already against the background of other complications. The mortality rate in the ARDS structure made up 44.1% (15 of 34) with early development and 17.6% (6 of 34) against the background of other complications.
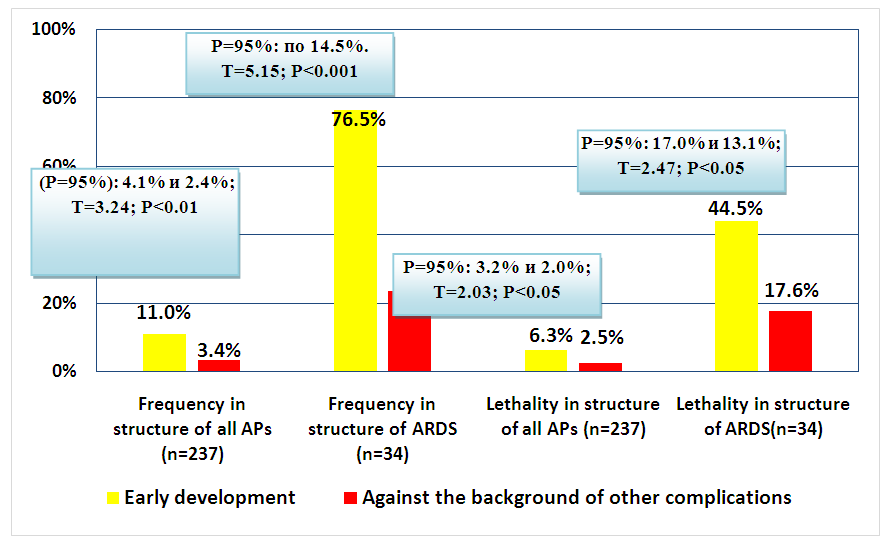 | Figure 1. Risk distribution of the development of ARDS as an early or late (against the background of other complications) factor of biliary pancreatitis complicated course |
5. Conclusions
- The problem of improving the tactical aspects of this severe pathology treatment affects not only surgical approaches, but also the issues of improving the quality of multicomponent conservative therapy. Despite certain disagreements on tactical issues, most experts agree on the need of developing diagnostic and treatment protocols for each form of acute pancreatitis, taking into account the experience and capabilities of each particular clinic. Differences in the frequency of systemic complications and mortality in conservative and surgical tactics can be caused, on the one hand, by the severity of the pathological process, when, within the edematous or destructive form of pancreatitis, a significant dispersion of indicators on prognostic scales is possible and, accordingly, a more serious condition in the group of surgical activity. However, on the other hand, it may also be the result of choosing an inadequate treatment of pancreatogenic complications.