-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2019; 9(2): 499-502
doi:10.5923/j.ajmms.20190912.11

Intra-abdominal Hypertension at Combined Injuries of the Abdominal Organs
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLI. B. Mustafakulov, A. M. Khadjibaev, Z. A. Djuraeva
Samarkand State Medical Institute, Samarkand branch of RRCEM, Uzbekistan
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The largest cavity of the human body is the abdominal cavity where there is a huge system of blood flow and many nerve endings, i.e. a huge receptor system. An increase of intra-abdominal pressure above normal levels can lead to negative consequences. Intra-abdominal pressure is a nonspecific manifestation of various surgical diseases. Therefore, high intra-abdominal pressure has independent practical importance. In pathological conditions, an increase of intra-abdominal pressure plays, may be not a key role in the development of systemic disorders, but competes with the leading damaging states. It has been proved that an increase of intra-abdominal pressure can have both a direct mechanical effect on the abdominal organs, and indirectly, through the diaphragm, on the lungs and heart, until the development of acute respiratory failure and decompensated circulatory failure. We have conducted a study of intra-abdominal pressure in 84 patients with combined abdominal trauma from 2008 to 2018in the Samarkand branch of the RRCEM. The age of the victims varied from 18 to 70 years (30.5 ± 8.9), while the majority of the victims were people of working age (up to 50 years), mostly men (n = 69). Combined abdominal injuries were accompanied by craniocerebral injury in 37 (44%) patients. The cause of the injury in most cases was a traffic accident (n = 67-79.7%), an unlawful injury - in 10 (11.9%) cases, catatrauma - in 7 (8.4%) victims. Alcohol intoxication was observed in 41 (48.8%) patients. In those patients whose surgery ends with suturing the abdominal wound tightly there is a high risk for developing intra-abdominal pressure and intra-abdominal hypertension syndrome. The signs of multiple organ failure were significantly expressed in the same group of patients, one of the reasons for which can be an increased intra-abdominal hypertension. Intra-abdominal pressure higher than 12 mm Hg is a “borderline” indicator, the increase of which leads to an increase of mortality.
Keywords: Abdominal trauma, Intra-abdominal pressure, Intra-abdominal hypertension syndrome
Cite this paper: I. B. Mustafakulov, A. M. Khadjibaev, Z. A. Djuraeva, Intra-abdominal Hypertension at Combined Injuries of the Abdominal Organs, American Journal of Medicine and Medical Sciences, Vol. 9 No. 2, 2019, pp. 499-502. doi: 10.5923/j.ajmms.20190912.11.
1. Introduction
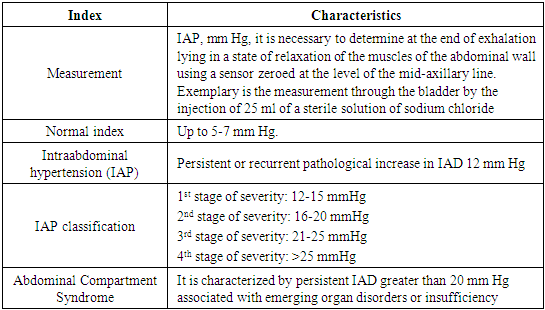
- Intra-abdominal pressure (IAP) is the formed pressure in the abdominal cavity. The IAP is normally approximately 5 mm Hg. A significant increase in intra-abdominal pressure occurs in 30% of casesat severe polytrauma, peritonitis. Syndrome of intra-abdominal hypertension (SIAH) (in the English-language sources Abdominal Compartment Syndrome (ACS)) is a pathological complex of symptoms that develops as a result of increased intra-abdominal pressure and is manifested by the onset of multiple organ failure [1-2] and is observed in 5.5% of such patients, with a mortality rate of 42% to 68% [3-4,14]. According to the data,in patients who were operated on due to the closed abdominal organ injury, ACS was up to 15% [11,14]. Due to the fact that against the background of an increase in intra-abdominal pressure, the development of multiple organ failure (MOF) is possible, mortality in patients with diagnosed ACS, according to the data, reached 70% [5,13]. Intra-abdominal pressure occupies a special place among the causes of multiple organ failure that arise after surgeries on the abdominal organs at severe polytrauma. In 1872 E. Wendt was the first to report on the phenomenon of intra-abdominal pressure, illustrated the formation of MOF and the high mortality rate of experimental animals which underwent an artificial increase of intra-abdominal pressure [6].The relevance of intra-abdominal hypertension in severe patients who are in serious condition is constantly increasing. There are evidences that the progressive increase of intra-abdominal pressure in these patients significantly increases the mortality rate [3,7]. Due to the considerable wording in the definition of ACS and its conducting, the first ever conference which was devoted to the problems of ACS was held in 2004. After multicenter international studies, the concept of the syndrome, the methodology of instrumental examination of patients were formulated, and methods for prevention and therapy were proposed [1,12]. According to data that have been cited in foreign literature, the numbers on the incidence of ACS vary significantly [8]. There are many reasons that can lead to the formation of ACS, but most often this syndrome occurs after severe injury of the abdominal organs, intra- or extra-abdominal bleeding [2,9].Aim of the study is to establish the diagnostic reliability of the intra-abdominal hypertension control for the choice of treatment method in patients with abdominal polytrauma.
2. Materials and Methods
- A study of intra-abdominal hypertension was performed in 76 patients with combined abdominal injury for the period of 2008-2018. The age of the studied victims ranged from 18 to 70 years (30.5 ± 8.9), while the majority of the victims were people of working age (up to 50 years), mostly men (n = 61). In 37 (48.6%) patients combined abdominal injuries were accompanied by traumatic brain injury. The cause of the injury in most cases was a traffic accident (n = 61-80.2%), in 10 (13.1%) patients - a wrongful injury, in 7 (9.2%) ones - a catatrauma. Alcohol intoxication was observed in 41 (53.9%) cases.The "golden standard" of the indirect measurement of intra-abdominal hypertension today is the use of the urinary bladder. Since the wall of the urinary bladder is well tensile and elastic, with a volume of not more than 25 ml it acts as a passive membrane and shows intra-abdominal pressure (IAP) for certain [9,10].
3. Results and Discussion
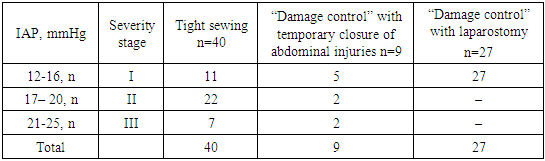
- According to the investigation protocol, IAP was measured upon admission to the ICU from the operating room and then every 6 hours for 5 days. These IAP indices are presented in table 1.
|
|
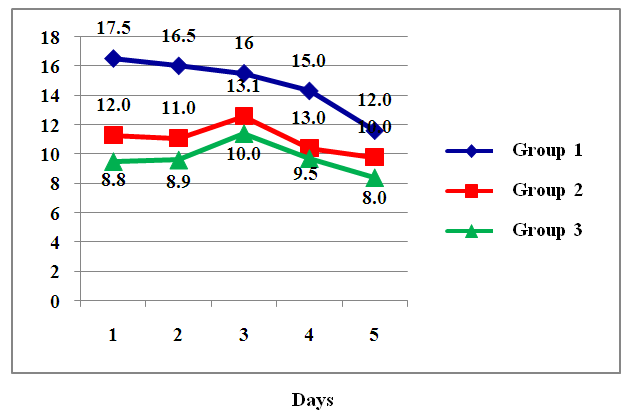 | Figure 1. Dynamics of intra-abdominal pressure over 5 days in patients with various options for closing the abdominal wound |
|
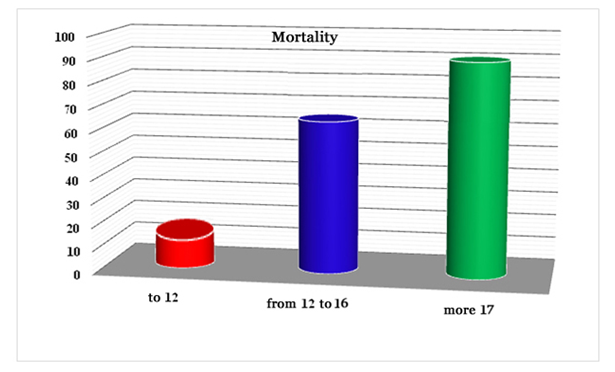 | Figure 2. Mortality (%) in groups depending on the IAP rate |
4. Conclusions
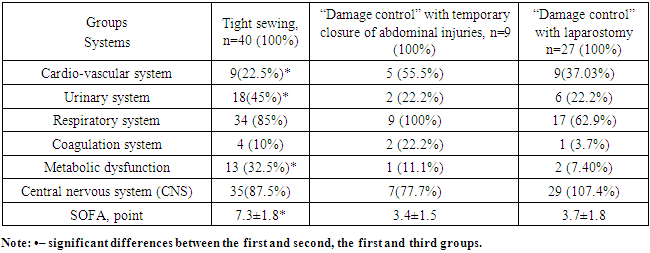
- In those patients in whom the operation ends with suturing the anterior abdominal wall tightly, the risk of IAP developing is high and the probability of ACS developing is high. In the same group of patients, signs of multiple organ failure are significantly evident, one of the reasons for which may be increased intra-abdominal hypertension. ACS is a rather unfavorable prognosis complication. The intra-abdominal pressure is greater than 12 mm Hg is a “borderline” indicator, the increase of which leads to an increase of mortality.