-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2019; 9(0): 405-408
doi:10.5923/j.ajmms.20190910.11

Prognosis in Patients with Myocardial Infarction
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLYusupov Donyorjon1, Kamilova Umida2
1Fergana Branch of the Republican Emergency Care Research Center
2Republican Specialized Scientific-Practical Medical Center of Therapy and Medical Rehabilitation, Uzbekistan
Correspondence to: Kamilova Umida, Republican Specialized Scientific-Practical Medical Center of Therapy and Medical Rehabilitation, Uzbekistan.
| Email: |  |
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The purpose of the research was to study the prognosis in patients with myocardial infarction. The study included 98 male patients aged from 35 to 60 years with primary Q-wave acute myocardial infarction, up to 10 days from the onset. Determination of early predictors of poor prognosis in patients with myocardial infarction identifies patients with high cardiovascular risk, which helps prevention complications and improve prognosis. Adverse allelic and genotypic variants of the T786C polymorphism (rs2070744) of the eNOS gene were significantly more common in patients with MI compared with the control group. According to the odds ratio, the risk of developing MI in the presence of carriage of an unfavorable genotypic variant T / C significantly increases by more than 1.8 times, which suggests the use of this genotypic variant for predicting the risk of MI in people of Uzbek nationality.
Keywords: Myocardial infarction, Prognosis, Endpoints, Genetic polymorphism
Cite this paper: Yusupov Donyorjon, Kamilova Umida, Prognosis in Patients with Myocardial Infarction, American Journal of Medicine and Medical Sciences, Vol. 9 No. 0, 2019, pp. 405-408. doi: 10.5923/j.ajmms.20190910.11.
1. Introduction
- Myocardial infarction (MI) is an important problem in modern medicine, since the incidence, disability and mortality for this reason remain high in developed countries. The high mortality of patients, as well as the fact that they have a part of cases when they have problems with heart failure, cardiac arrhythmia, reinfarction, and the resumption of angina, which worsen the quality of life and limit the number of patients, have social significance of acute myocardial infarction (AMI) [1,2]. Such a high medical and social significance of MI requires further improvement of its methods of early diagnosis, effective treatment and secondary prevention [3].The ability to predict the nature of adverse postinfarction remodeling of the left ventricle (LV) is equivalent to identify complications in the early period of myocardial infarction with high cardiovascular events and cardiac death in the long-term period.There are a number of indicators that show a high probability of poor prognosis after myocardial infarction: patient's age, the presence of myocardial infarction, disturbance of systolic and diastolic function of the LV, ventricular arrhythmias in the history of ventricular fibrillation, the front or anterior-inferior myocardial infarction, unstable angina, the progression of heart failure [4,5].Several multicenter clinical and retrospective studies have demonstrated the diversity and complexity of the factors determining the prognosis of AMI [6,7].The risk of cardiovascular complications and prognosis are largely determined by individual genetic risk factors. In this connection, the study of genetic factors in the development, course and prognosis of cardiovascular diseases is gaining great theoretical and practical significance. In the pathogenesis of MI, an important role is given to endothelial dysfunction, the dysfunction of which contributes to the aggravation of cardiovascular remodeling processes. There are a large number of works devoted to the study of the effect of polymorphism of NO synthase genes on the development of cardiovascular pathology, since the polymorphism of the eNOS gene can cause hereditary differences in the synthesis of nitric oxide and, thus, contribute to the emergence of different propensities for the development of diseases. [8,9]Purpose of research was to study of prognosis in patients with myocardial infarction.
2. Material and Methods
- The study included 98 male patients aged from 35 to 60 years with primary Q-wave acute myocardial infarction, up to 10 days from the onset. Diagnosis is based on the WHO criteria for the presence of the following symptoms: typical anginal pain attack or its equivalent for at least 30 minutes; appearance of pathological Q waves or QS in two or more ECG leads. The stationary phase of AMI treatment was carried out in accordance with recommendations for management of patients with myocardial infarction with elevation segment ST (ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation, 2017) and included thrombolytic therapy if indicated, early administration of beta-blockers, antiplatelet agents, anticoagulants, as well as nitrates (including intravenously), statins, ACE inhibitors, diuretics. According to the study plan, the final analysis included data of patients who within one year from the start of them to develop meaningful clinical outcomes: death, recurrent nonfatal MI; occurrence or progression of heart failure or coronary artery disease destabilization that required hospitalization. All patients were informed about the protocol and agreed to participate in the study. Exclusion criteria included: age over 60 years; permanent form of atrial fibrillation; hypotension (blood pressure <100/60 mm Hg); comorbidities that can independently affect the prognosis of life or remodeling of the left ventricle. Molecular genetic studies - the study of the C786T polymorphism of the NOS3 gene was carried out in 117 patients and 104 healthy people of Uzbek nationality using evidence of a chain reaction on CG-1-96 programmable thermal cyclers Corbett Research (Australia) and 2720 "Applied Biosystems" (USA) in the department of molecular medicine and cell technology at the research institute of hematology and blood transfusion. Statistical processing of genetic research data was carried out using the Open Epi version 9.2 software package. The endpoints of the study were studied after 6 months and 1 year: the frequency of repeated non-fatal and fatal myocardial infarction, mortality.
3. Results and Discussion
- When analyzing the detection of complications in the early post-infarction period, the presence of dependence on the localization of AMI was revealed. Thus, the development of aneurysm is 2.7 times more often observed in patients with anterior AMI. Signs of AHF developed 2.1 times more often in patients also with anterior localization of MI. Early post-infarction angina developed with the same frequency in groups with anterior and posterior localization of AMI. We have evaluated the forecast in the studied groups of patients. The development of early post-infarction angina is not associated with a sharp decrease in the initial EF, apparently there is a degree of occlusion of the infarct-related artery and other possible causes [10]. However, with regard to the development of cardiac aneurysm and AHF, both localization and type of MI have a differentiated meaning. Analysis of complications in revealed the following: the incidence of complications in the early post-infarction period is statistically significantly associated with the localization of myocardial infarction - most often aneurysm is observed with anterior localization of AMI.The decrease in ejection fraction (EF) at rest is a predictor of a poor prognosis after MI. The study of prognostic significance confirmed the presence of a significant association of late mortality, sudden death, development of HF and progression of ventricular arrhythmias with a reduced level of EF [11]. Analysis of post-infarction remodeling showed that LV systolic dysfunction (EF <40%) occurred in 14 (17%) patients. A moderate decrease in the contractile function of the LV (40
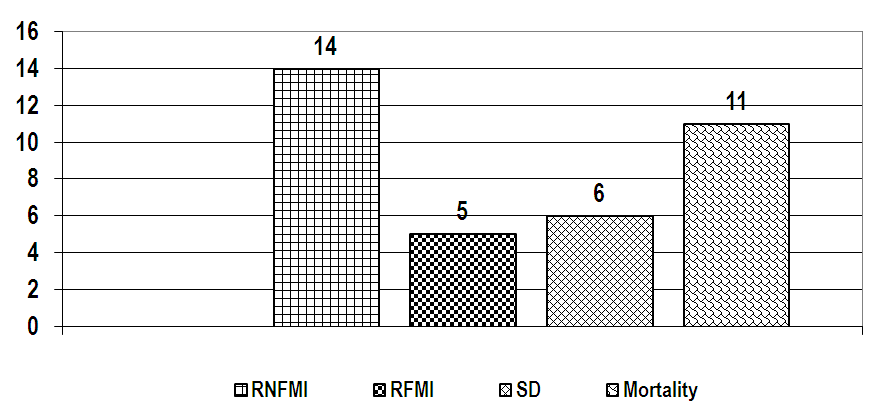 | Figure 1. The endpoints in MI patients after 1 years |
4. Conclusions
- Determination of early predictors of poor prognosis in patients with myocardial infarction identifies patients with high cardiovascular risk, which helps prevention complications and improve prognosis.