Akhmedova Nilufar1, Akhmedova Dilorom2
1PhD, Doctoral Student of the Department of Hospital Pediatrics №2, Tashkent Pediatric Medical Institute, Tashkent, Uzbekistan
2Professor, Director, Republican Specialized Scientific and Practical Medical Center of Pediatrics, Tashkent, Uzbekistan
Correspondence to: Akhmedova Nilufar, PhD, Doctoral Student of the Department of Hospital Pediatrics №2, Tashkent Pediatric Medical Institute, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The article presents the results of the studies of 104 patients with cardiomyopathies hospitalized in cardio-rheumatological department of the Republican Specialized Scientific and Practical Medical Centre of Pediatrics in Tashkent and the National Children's multi-profile medical centre of Karakalpakstan. Analysis of the results of the study showed that in children with cardiomyopathy marked increase in tissue levels (LDH, CPK) and cardiospecific (CPK-MB) enzymes, regardless of region of residence and form of the disease, which is the testimony of et of myocardial dysfunction. In this connection, these enzymes can be regarded as highly specific biochemical markers of myocardial damage, and the increase in their activity can be regarded as criteria for the diagnosis of cardiomyopathy in children. Of the biochemical parameters, a reliable prognostic criterion for the development and outcome of cardiomyopathies is a progressive increase in the level of endothelin with increasing duration of the disease.
Keywords:
Children, Cardiomyopathy, Creatine phosphokinase –MB, Tissue enzymes, Troponin, Endothelin
Cite this paper: Akhmedova Nilufar, Akhmedova Dilorom, Biochemical Indicators of Heart Failure and Myocardial Damage in Children with Cardiomyopathy, American Journal of Medicine and Medical Sciences, Vol. 9 No. 9, 2019, pp. 342-346. doi: 10.5923/j.ajmms.20190909.07.
1. Introduction
Diseases of the cardiovascular system have a special significance associated not only and even not so much with their wide distribution, as with the role that these diseases play in the disability of children and in the formation of the incidence of adults [3,16]. Among cardiovascular diseases in children, cardiomyopathy (CMP) occupies a special place, the growth of which has been noted recently, which is associated with the widespread introduction of highly informative instrumental methods for studying the heart [5,19]. The need to further study the problem of cardiomyopathy in children is also related to the fact that in recent years there has been a tendency to overdiagnose them due to the insufficiently active search for other known causes of myocardial damage and circulatory failure [11,14,24]. High disability and mortality of children suffering from cardiomyopathy, the lack of clear clinical and functional markers of diagnosis, the course of the process, and effective treatment methods determine the urgency of the problem. One of the early signs of the development of cardiomyopathy is a violation of the contractile function of the myocardium and chronic heart failure. In recent years, the attention of researchers has been drawn to the study of the role of a number of peptides in cardiovascular diseases: endothelin, neuropeptide Y and cytokines, chromogranin A, troponins, etc. [1,4]. For the first time, scientists wrote about the role of endothelial cells as a regulator of vascular tone in 1980. Researchers have characterized endotheliocytes as "a cardiovascular endocrine organ that promotes the interconnection of blood and tissues at a critical moment". It was also found that endothelin-1 is a marker and predictor of the severity and outcome of cardiovascular diseases [7]. In the heart muscle, the contractile function is regulated by a special protein tropomyosin complex. Under pathological conditions, the mechanism of functioning of the troponin-tropomyosin component is largely determined by the degree of hypoxic damage to the heart [13,15]. Currently, the determination of components of the troponin complex of cardiomyocytes is already quite widely used in cardiological practice, mainly for the diagnosis of myocardial infarction. Troponins are released from damaged myocardial cells and through the lymphatic system they enter the general bloodstream [8,9,13]. In this regard, the study of enzymes and cardiac markers as markers of myocardial damage in children with cardiomyopathy is relevant and appropriate.
2. The Purpose of the Study
About to limit the biochemical indicators of myocardial damage in children c cardiomyopathies s, depending on the form of the disease and the place of residence of children.
3. Materials and Methods
We examined 104 patients hospitalized in cardio-rheumatological department of the Republican Specialized Scientific and Practical Medical Center of Pediatrics in Tashkent and Children's multi-profile medical centre of Karakalpakstan. The average age of the surveyed was 8.9±0.6 years old and varied from 1 to 17 years. Comprehensive examination of patients included: collection of anamnestic data - family history, obstetric history of the mother, hereditary predisposition, history of the child's life, past diseases; term and nature of the onset of the disease, assessment of the general condition and physical development. The diagnosis was made on the basis of complaints, physical examination, laboratory and instrumental methods of research (clinical and biochemical blood tests, chest X-ray, ECG and Echo-KG). Analysis of anamnestic, clinical, laboratory and instrumental data showed that all patients, regardless of nosology, were united by the presence of chronic heart failure at the time of the study. The average disease duration was 19,2 ± 3,1 months. Distribution of children depending on the type of cardiomyopathy presented in fig. 1. As can be seen from the figure, most of the examined patients were children with dilated cardiomyopathy (DCMP) (45,2%) and hypertrophic cardiomyopathy (HCMP) (34,6%), and in a smaller percentage of cases, restrictive cardiomyopathy (RCMP) was diagnosed (4,8%). 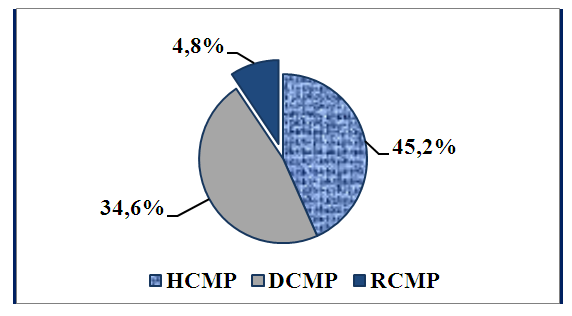 | Figure 1. The distribution of children depending on the type of cardiomyopathy |
Biochemical methods included determining total protein and protein fractions, C-reactive protein, blood electrolytes (potassium, sodium, calcium); the activity of lactate dehydrogenase (LDH), creatine phosphokinase (CPK), alanine aminotransferase (ALT) and aspartate aminotransferase (AST), as well as a cardiospecific enzyme - creatine phosphokinase - MB (CPK-MB) and cardiac markers (troponin I and endothelinyn-1). Enzymes were determined on a biochemical automat analyzer " Cobas 6000 R " c using reagents of the company “ Human ” (Germany). Cardiac markers were determined by immunofluorescence analysis on an “IMAXIZ» and «Multickan» semi-automatic machines using «Hema» reagents (Russia).Statistical processing of the results was carried out using the program " Statistica 6.0 ". The significance of differences in the compared parameters was calculated using Student's criterion.
4. Results and Discussions
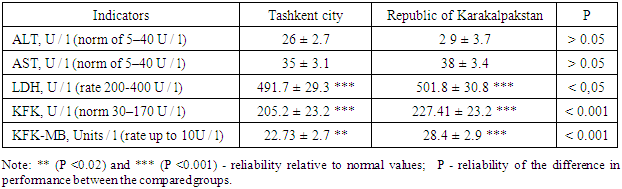
The goal was to identify specific biochemical markers of damage to the heart muscle in this pathology. We carried out laboratory studies, including the study of the activity of tissue enzymes and cardiac markers in children with cardiomyopathies. Analysis of the results of indicators of tissue and cardiac enzyme indicates that the median indicators of LDH, CPK and CPK-MB were significantly increased in comparison with the norm. It should be noted that in children living in the Republic of Karakalpakstan, these changes were more pronounced and significantly higher than those of children in Tashkent. The values of the remaining enzymes (AST and ALT) were within the normal range (Table 1). Table 1. Indicators of the level of tissue and cardiospecific enzymes in children with cardiomyopathy
 |
| |
|
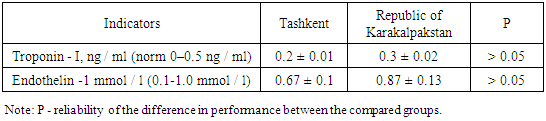
During the studies revealed increase in cardiac enzymes (CPK, creatine kinase MB fraction) in serum reflects the degree of damage to myocardial cells. It should also be noted that these biomarkers reflect the presence of necrosis of cardiomyocytes, but do not allow to clarify the cause of its development [8,9,12]. Our results determining enzyme levels revealed high accuracy increase of tissue enzymes LDH and CPK and cardiospecific isoenzyme of creatine phosphokinase MB fraction, the most pronounced increase in these enzymes has been common in children living in Karakalpakstan, as well as in ecologically unfavorable region. Based on these results, it can be concluded that the above enzymes can be regarded as highly specific biochemical markers of damage to the heart muscle, and the increase in their activity can be considered as criteria for the development of cardiomyopathies in children. Determination of the components of the cardiomyocyte troponin complex is the most sensitive and specific biochemical marker of myocardial necrosis and therefore is already widely used in cardiology practice mainly for the diagnosis of myocardial infarction. [1,2,5,20]. In 2000, the leading cardiological communities of Europe and the USA developed the so-called “ consensus ” document in the definition of myocardial infarction, in which troponin was approved as the main diagnostic criterion for myocardial infarction. In the past few years, the definition of troponins has been used in pediatrics, mainly in neonatology [2]. In these works, the examination of newborns was carried out on the 1st week of life, the study included children with CNS pathology, premature and low birth weight infants. Exclusion criteria were congenital heart defects (CHD), cardiac arrhythmias, genetic abnormalities. At the same time, an increase in troponins was noted in children in serious condition (intraventricular hemorrhages, prolonged artificial ventilation of the lungs, etc.). Based on these data, we found it appropriate to determine the degree of significance of troponin and endothelin-1 as a marker of the development of CMP in children. An increase in troponin concentration in children suggests that the terminal stage of chronic heart failure (CHF) is accompanied by the death of cardiomyocytes and the release of cardiospecific proteins into the blood. The level of troponin in our examined children corresponded to permissible values regardless of the region of residence, which indicates non-sensitivity and non-specificity this biochemical marker for this disease, and is most characteristic of the myocardial necrosis. (Table 2). Table 2. Indicators cardiac markers in children with cardiomyopathy
 |
| |
|
According to the literature [10,21,22], endothelin is considered as a marker and predictor of the severity and outcome of cardiovascular diseases. Endothelin is among the biologically active bicyclic broad-spectrum polypeptides, there are three isoforms endothelin: endothelin-1, endothelin-2 and endothelin-3 [7,17,18,23]. Today, endothelin-1 is one of the most significant regulators of the functional state of the vascular endothelium and the determination of plasma endothelin- 1 concentration helps to establish the diagnosis of heart failure in the early stages of the disease. [6,21,22]. But at the same time, according to the results of our research, high indices of endothelin -1 with severe CHF were observed as the disease progressed (Fig. 2).As can be seen from Figure 2, in patients with a disease duration of 5 years, the level of endothelin is -1 averaged 1 3 ± 0,08 mmol/l, in patients with a disease duration of 9 years, this average was 1.7 ± 0.1 mmol/l, and in a patient with a disease duration of 15 years - 1.98 ± 0.2 mmol/l, which is 2 times higher than normal values. A correlation analysis between the prescription of CMP, the severity of CHF and the level of endothelin -1 revealed a strong direct correlation (r = + 0.97). In this regard, the level of endothelin -1 can be regarded as a prognostic criterion for the course and outcome of the CMP.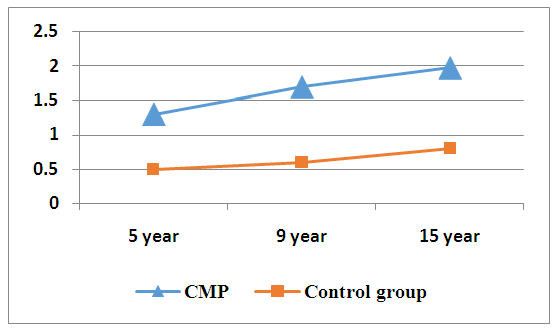 | Figure 2. Indicators of endothelin -1 depending on the duration of the disease |
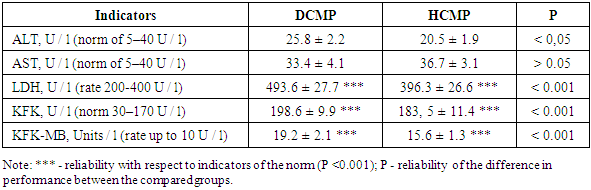
Further, in order to assess the state of the myocardium in children with CMP, we analyzed tissue and cardiospecific enzymes depending on the form of the disease, which indicated the presence of similar changes in these indicators, as well as depending on the place of residence of the children. However, it should be noted that in children with DCMP, the indicators of LDH, CPK, CPK-MB tissue enzymes were significantly higher compared with the comparison group (Table 3). In both forms of the CMP, the level of ALT and AST enzymes differed slightly and corresponded to the average values of the norm. Table 3. Indicators of tissue and cardiac enzymes depending on the form of cardiomyopathy
 |
| |
|
Indicators troponin children were also at the regulations and overt performance regardless of the disease, and endothelin -1 level was significantly higher in children with HCMP and corresponded to the upper limit of normal, as compared with children with DCMP (Table 4).The results of our studies revealed that with cardiomyopathy, the level of troponin does not significantly differ from the normal values, whereas the level of endothelin-1 increases significantly with the progression of the disease, which indicates the significance of this indicator in the development and prediction of the outcome of CMP in children. Table 4. Indicators cardiac markers depending on the form of cardiomyopathy
 |
| |
|
5. Findings
In Children with CMP regardless of the form of the disease marked increase in tissue (LDH, CPK), and cardiospecific (CPK-MB) enzymes that testify about myocardial damage. The most pronounced increase in the level of these enzymes is characteristic of children living in the Republic of Karakalpakstan. Reliable prognostic criterion of development and outcome of the CMP is also a progressive increase endothelin -1 level with increasing duration of the disease. Based on this, we can conclude that LDH, CPK, CPK-MB and endothelin-1 cardiac marker can be regarded as highly specific biochemical markers of myocardial damage, and an increase in their activity can be considered as criteria for the development of cardiomyopathies in children.
References
| [1] | Amelyushkina V.A., Kotkina T.I., Titov V.N. Biochemical markers of the affected myocardium. Klinicheskaya meditsina. 2000; 5: 9–13. |
| [2] | Baba Y., Kubo T., Yamanaka S., Hirota T., Tanioka K., Yamasaki N. et al. Clinical Significance of High-Sensitivity Cardiac Troponin T in Patients With Dilated Cardiomyopathy. Int. Heart J. 2015; 56 (3): 309–313. |
| [3] | Berezneva N.A., Sorokina T.E., Averyanova N.S., Gromyko O.E., Arsenyeva E.N., Kustova O.V., Vashakmadze N.D., Basargina E.N., Pinelis V.G. Blood pressure and gene polymorphism for children with hypertrophic cardiomyopathy. Rossiyskiy pediatricheskiy zurnal. 2012; 6: 10-3. |
| [4] | Bershova T.V., Bakanov M.I., Basargina E.N., Gasanov A.G., Ivanov A.P., Monaenkova S.V. Dynamics of biochemical markers of myocardial remodeling in children with dilated cardiomyopathy against the background of complex therapy. Rossiyskiy pediatricheskiy zhurnal. 2014; 5: 25-9. |
| [5] | Chernykh N.Yu., Groznova O.S., Tarasova A.A., Shigabeev I.M. Biochemical markers of ischemia, heart failure and myocardial deformity with hypertrophic cardiomyopathy. Pediatriya (Pril. K zhurn. Consilium Medicum). 2018; 4: 80–84. |
| [6] | Davenport A.P. Endothelin. Pharmacol. Rev. - 2016; 68 (2): 357-418. |
| [7] | Dremina N.N., Shurygin M.G., Shurygina I.A. Endothelin in health and disease. Mezhdunarodniy zhurnal prikladnykh i fundamentalnykh issledovaniy. 2016; 10: 210-4. |
| [8] | Eisenberg M.A., Green-Hopkins I., Alexander M.E., Chiang V.W. Cardiac troponin T as a screening test for myocarditis in children. Pediatr. Emerg. Care.2012; 28 (11): 1173–8. |
| [9] | Gilyarevsky S.R. Myocarditis: modern approaches to diagnosis and treatment. M.: Me dia Sphera, 2008; 324 p. |
| [10] | Hiyama T.Y. Endothelin-3 expression in the subfornical organ enhances the sensitivity of Na (x), the brain sodium- levelsensor, to suppress salt intake. Cell Metab. - 2013; 17: 507-519. |
| [11] | Hsia T.Y., Ringewald J.M., Stroud R.E., Forbus G.A., Bradley S.M., Chung W.K., Spinale F.G. Determinants of extracellular matrix remodeling are differentially expressed in paediatric and adult dilated cardiomyopathy. Eur. J. Heart Fail. 2011; 13 (3): 271-7. DOI: 10.1093 / eurjhf / hfq184. Epub 2010 Dec 8. |
| [12] | Izumi T., Nishii M. Diagnostic and prognostic biomarkers of acute myocarditis. Interleukin-10. Herz. 2012; 37 (6): 627–31. |
| [13] | JCS. Joint Working Group. Guidelines for diagnosis and treatment of myocarditis (JCS 2009): digest version. Circ. J. 2011; 75 (3): 734–43. |
| [14] | Kessler E.L., Nikkels P.G., van Veen T.A. Disturbed Desmoglein-2 in cardiomyopathy. Hum Pathol. 2017; 67: 101-8. |
| [15] | Korotkova A.A., Titov V.N., Staravedov I.I. The prognostic role of cardiac troponin I in patients with ST-free syndrome. Kardiologiya. 2002; 4: 19–22. |
| [16] | Kozhevnikova O.V. Risk factors and markers for early diagnosis of cardiovascular diseases in children. [dissertation abstract] Moscow; 2017. 311 p. |
| [17] | Liefeldt L. Effects of transgenic endothelin-2 on diabetic cardiomyopathy in rats. Eur. J. Clin. Invest. - 2010; 40 (3): 203-210. |
| [18] | Ling L., Magazine J.J., Davenport A.P. Endothelin-2, the forgotten isoform: emerging role in the ardiovascular system, ovarian development, immunology and cancer. Br. J. Pharmacol. – 2013; 168 (2): 283-95. |
| [19] | Linyaeva V.V., Leontyeva I.V., Pavlov V.I., Ivanova Yu.M., Vozdvizhenskaya E.S. Biochemical and electrophysiological markers for children with hypertrophic cardiomyopathy. Pediatriya. Zhurnal im. G..N.Speranskogo. 2015; 94 (2): 60-2. |
| [20] | Shammas N.W., Padaria R.F., Coyne EP Pericarditis, myocarditis, and other cardiomyopathies. Prim.Care. 2013; 40 (1): 213–36. |
| [21] | Shurygin M.G. Endothelin expression in experimental myocardial infarction under conditions of altered concentration of fibroblastic and vasoendothelial growth factors. Bulleten VSNTsSO RAMN. 2013; 1 (89): 125-9. |
| [22] | Shurygin M.G. The number of endothelin production in myocardial infarction. Fundamentalnye issledovaniya. 2015; 1: 1281-7. |
| [23] | Tanowitz H.B. Role of endothelin 1 in pathogenesis of chronic chagasic heart disease. Infect. Immun. 2005; 73: 2496-2503. |
| [24] | Yanagimoto K., Okamoto Y., Kodama Y., Nishikawa T., Tanabe T., Kawano Y. Speckle Tracking Indicates Drug-induced Cardiomyopathy After Chemotherapy in Cancer. J. Pediatr. Hematol. Oncol. 2017; 39 (1): 10-14. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML