-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2019; 9(9): 322-324
doi:10.5923/j.ajmms.20190909.02

Evaluation of Risk Factors for Cardiovascular Diseases
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLTurdiev M. R. , Kamilova U. K. , Ismailov S. I.
Republican Specialized Scientific-Practical Medical Center of Therapy and Medical Rehabilitation, Tashkent, Uzbekistan
Correspondence to: Kamilova U. K. , Republican Specialized Scientific-Practical Medical Center of Therapy and Medical Rehabilitation, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The aim of our study was to evaluate the role of determining the total cardiovascular risk on the SCORE scale in primary care in the prevention of CVD. 793 respondents were examined, of these 475 (59.89%) were women and 318 (40.1%) men. Prediction of cardiovascular risk over 10 years was carried out using the SCORE scale. Cardiovascular risk factors for cardiovascular diseases such as smoking, hypercholesterolemia (HCh), abdominal obesity (AO), low of physical activity (FA), frequency of arterial hypertension (AH) were assessed. The results of studies of total cardiovascular risk on the SCORE in 793 examined patients: the average cardiovascular risk was found in 9.0%, moderate risk in 4.0%, high in 4.0% and very high in 1.0% of patients.
Keywords: Cardiovascular risk, SCORE scale, Prevention
Cite this paper: Turdiev M. R. , Kamilova U. K. , Ismailov S. I. , Evaluation of Risk Factors for Cardiovascular Diseases, American Journal of Medicine and Medical Sciences, Vol. 9 No. 9, 2019, pp. 322-324. doi: 10.5923/j.ajmms.20190909.02.
1. Introduction
- Cardiovascular diseases (CVD) are the leading cause of death worldwide. About 17.3 million people die from CVD each year, accounting for 31.5% of all deaths in the world and 45% of all deaths from non-communicable diseases (NCDs). It is important to engage in primary prevention of chronic diseases from childhood, as numerous studies have confirmed that the so-called “risk factors”, which are formed in childhood and adolescence, have “stability” and subsequently pass into the lifestyle of an adult. In 2016, the European Guidelines for the Prevention of Cardiovascular Diseases in Clinical Practice [1], developed by the European Society of Cardiology with the participation of representatives from 10 other professional societies and invited experts, were published. These guidelines identify effective actions at the population and individual levels aimed at preventing CVD and reducing their contribution to morbidity and mortality. Analysis of the reasons for a significant (more than 2-fold) decrease in mortality from CVD over the past decades in many developed countries showed that the contribution of treatment of CVD patients to mortality reduction is relatively high, ranging from 23% to 47%. In this regard, the quality of care for patients with CVD should be given great attention. At the same time, the contribution of widespread promotion of healthy lifestyles and the reduction of risk factor (RF) levels at the population level (total population or population groups) in reducing CVD mortality is even more significant, ranging from 44% to 60% [2,3]. Prevention is effective while adhering to the principles of a healthy lifestyle and reducing the level of major risk factors in the population, it can prevent up to 80% of premature deaths from CVD and up to 40% of deaths from cancer [4,5]. In connection with the above, the implementation of active cardiovascular prevention at a broad population level and in daily clinical practice is the most important condition for further reduction of mortality [6,7].The aim of our study was to evaluate the role of determining the total cardiovascular risk on the SCORE scale in primary care in the prevention of CVD.
2. Materials and Methods
- The sampling was carried out by random sampling of 793 people from the population of the Surkhandarya region aged 40 to 60. Risk factors were determined using a questionnaire and the risk of developing cardiovascular events was assessed using the SCORE scale. All persons interviewed on the standard questionnaire; containing questions about family history, heredity, smoking status, hypercholesterolemia (HCh) level of physical activity (FA), diet, Rose's questionnaire, a survey on the course of arterial hypertension (AH). Smokers were people who smoked at least one cigarette / cigarette per day. The smoking status was determined as follows: never smoked, smoked in the past, smokers at the present time. FA was assessed as normal FA: in the sitting position <5 hours a day and walking daily for at least 30 minutes and / or exercise at least 2 hours a week, and low FA (NFA): in the sitting position> 5 hours a day and walking daily <30 minutes and / or physical exercise <2 hours per week. or walking daily <30 min. and physical exercise <2 h per week.). When assessing nutrition, a WHO questionnaire was used, which included questions on the frequency of nutrition, intake of edible salt, carbohydrates, animal fats and proteins. Salting of cooked food and / or daily intake of salty products are taken for violations of reception of edible salt. Excessive intake of animal fats was considered. To assess abdominal obesity (AO), ATP III (Adult Treatment Panel III) criteria – from > 102 cm for men and > 88 cm for women and the International Diabetes Federation (MFD) were used.
3. Results
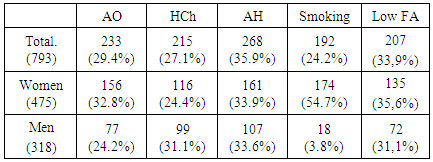
- 793 respondents were examined, of these 475 (59.89%) were women and 318 (40.1%) men (Table 1). Hereditary treatment was rejected in 213 (26.86%) of the patients. At the same time, the occurrence of significant differences between men and women was not.233 (29.4%) of the surveyed had AO, while obesity was more common in women - 156 (32.8%). Smoking as a risk factor was found in 192 (24.2%) patients, while every other 174 (54.7%) man belongs to the category of smokers, while for women this indicator was 18 (3.8%). In the present study, it was revealed that HCh is one of the common RF CVD. In a random sample of people of working age, HCh was diagnosed in 215 (27.1%) cases. Among men, an elevated level of cholesterol is found in 31.1% of cases, while among women, GHS occurred in 24.4% of cases.In the present study, an average of 268 (35.9%) respondents have AH, while among men, AH is spread in 33.6% and in women – 33.9%.During questioning and active questioning, low physical activity was detected in 207 (33.9%) people (lifestyle features, habits, restriction due to the occurrence of pain or discomfort in the heart area, the appearance of inspiratory shortness of breath during exercise). The survey results show that every second respondent has low physical activity, while there is no statistically significant difference between men and women.
|
4. Discussion
- Prevention of CVD is a complex of coordinated activities aimed at the entire population or certain groups of the population (individuals) to prevent the development and progression of CVD or minimize the burden of CVD and related disability [8]. It is known that prevention of CVD should combine population intervention methods aimed at promoting healthy lifestyles and individual types of intervention for people with moderate, high risk of CVD and patients with an established diagnosis of the disease, including due to their correction of RF [9,10].In the foreword of the recommendation it is noted that prevention, to be successful, should be carried out at the level of the general population through promotion of a healthy lifestyle (HLS), and at the level of patients with increased risk or with diagnosed CVD - by eliminating "unhealthy" behavior and reducing RF levels.The concept of “risk factors” is based on the results of prospective epidemiological studies and is currently the methodological basis for planning and organizing primary prevention of cardiovascular pathology. According to the concept, distinguish between modifiable and non-modifiable risk factors. Non-modifiable risk factors are age, gender, genetic predisposition, which are used to develop a system for stratifying the risk of developing diseases.
5. Conclusions
- The activity of preventive measures should be the greater, the higher the initial cardiovascular risk in a person. At the same time, the number of persons who need to take preventive measures in order to prevent one cardiovascular event is significantly less among those with initially high cardiovascular risk compared with the group of people with low risk.