Karshiev Khurram Karshiyevich
Doctor of the Department Maxillofacial Surgery, Tashkent State Dental Institute, Tashkent, Uzbekistan
Correspondence to: Karshiev Khurram Karshiyevich, Doctor of the Department Maxillofacial Surgery, Tashkent State Dental Institute, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
In patients with phlegmon of the maxillofacial area with a complicated course, along with clinical changes observed marked changes in adaptive immunity. In order to determine the immunological changes in the body was performed a comparative study of circulating immune complexes and immunoglobulins content. Their greatest change was revealed in phlegmons of the maxillofacial area complicated by severe sepsis. The most sensitive research methods were used to determine immunity parameters. In order to increase the effectiveness of treatment in phlegmon of the maxillofacial area complicated by sepsis and severe sepsis were used a combination of highly efficient physical methods and a promising antiseptics. Local application of sodium hypochlorite solution with complex intensive treatment of complicated phlegmons of maxillofacial area did not have a significant impact on the clinical and immunological parameters of the inflammatory process. The inclusion of intravascular laser irradiation of blood in combination with irrigation of a wound with a freshly prepared solution of sodium hypochlorite into the complex of intensive treatment leads to significant improvement not only clinical but also laboratory parameters in the maxillofacial phlegmons complicated by sepsis. Two-time irrigation of wounds did not contribute to the improvement of clinical and laboratory indicators of immunity. The combination of ultraviolet blood irradiation with two-time irrigation of wounds with complex treatment of phlegmon complicated by severe sepsis had the most effective influence on clinical and laboratory parameters. Based on this, it should be assumed that the combined use of ultraviolet blood irradiation with two times irrigation of wounds with sodium hypochlorite solution in the intensive treatment of phlegmon of the maxillofacial area is the most effective treatment method.
Keywords:
Odontogenous inflammatory diseases, Odontogenous infection, Odontogenous sepsis, Immunity, Immunoglobulins
Cite this paper: Karshiev Khurram Karshiyevich, The Effect of Various Methods of Complex Treatment on Immunity Indices in Phlegmons of Maxillofacial Area Complicated by Sepsis, American Journal of Medicine and Medical Sciences, Vol. 9 No. 9, 2019, pp. 315-321. doi: 10.5923/j.ajmms.20190909.01.
1. Introduction
In recent years, among the diseases of the maxillofacial area, aggressive acute purulent-inflammatory diseases have become more common. In this regard, the attention of clinicians is increasingly attracted by the state of the immunological reactivity of the organism and the micro flora of a purulent wound. It has become generally accepted opinion about the leading role of facultative and especially obligate anaerobic non-spore-forming microorganisms in the development of acute purulent-inflammatory diseases of the maxillofacial area. Many studies have found that, when body resistance decrease, these representatives of anaerobes acquire the ability to penetrate tissue barriers and cause severe purulent inflammatory processes [2,4,8].The object of the research is to study the effect of local irrigation of wounds with a freshly prepared sodium hypochlorite solution and the use of sodium hypochlorite in combination with intravascular laser irradiation of blood and ultraviolet blood irradiation on clinical and laboratory parameters in phlegmons of the maxillofacial area complicated by sepsis and sepsis severe.
2. Materials and Methods
A total of 59 patients have been examined with common phlegmon of the maxillofacial region complicated by sepsis and severe sepsis.The levels of immunoglobulins and circulating immune complexes were determined according to the standard procedure. The study was performed on the day of admission, on 5-6th days and on discharge from the hospital. A sodium hypochlorite solution was obtained using an Espero-1 apparatus and intravascular laser irradiation was performed by LTM-01 apparatus as modified. Ultraviolet irradiation of blood carried out by the device DRT-240 according to the common procedure. Statistical data processing. Statistical processing of the research results was performed using SPSS Statistics 17.0, Windows. Results are presented as mean values (M ± sh). The significance of the differences of the samples was carried out according to the non-parametric Mann-Whitney-Wilcoxon criteria; in the case of a normal distribution of indicators, the significanse of differences in mean values was determined by the Student's t-test. The significance level was considered significant at p <0.05.
3. Results
Taking into account the expressed inhibitory properties of odontogenic bacterial infection and its toxins on the protective function of adaptive immunity in purulent-inflammatory diseases of the maxillofacial area, especially in their severe course, in the complex of intensive treatment measures of 17 patients with phlegmons of the maxillofacial area complicated by sepsis included daily irrigation of the wound with freshly prepared sodium hypochlorite solution as an effective antiseptic. The general condition of patients of this group regarded as “severe”.As follows from the data presented in the figures (Fig. 1, 2), in patients of this clinical observation subgroup a noticeable violation of adaptive immunity factors have noted upon admission to the hospital.However, in patients ranged by us to this subgroup, the CIC (circulating immune complex) level was recorded as the highest and averaged 0.262 ± 0.018 conv. units, which is by 2 times more than the same indicators in healthy individuals (P <0.001).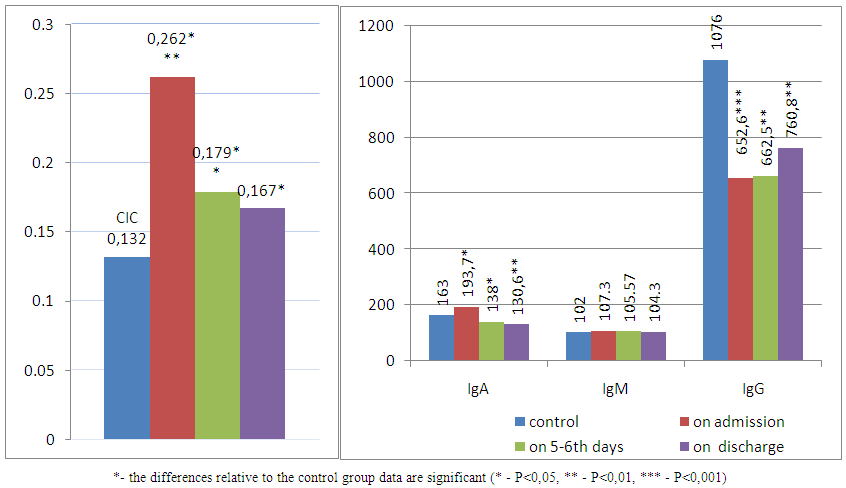 | Figure 1, 2. Indicators of the CIC and immunoglobulins A, M and G content dynamics in intensive therapy + NaClO3 of maxillofacial area phlegmons and their complications |
During the study of the dynamics of clinical and immunological parameters, it was found that on the background of a general satisfactory condition, decrease in body temperature and cleansing wounds from purulent-necrotic masses for 6-7 days of complex treatment, there was a decrease in the CIC concentration on average to 0.179 ± 0.013 conv. units, which is significantly (P <0.01) lower compared with baseline. But in the period of observation, it was still exceeded by 24.2% than the CIC values of healthy people. In addition, there were no changes on the part of the immunoglobulin concentration values A - 136.66 + 6.1, M - 105.57 ± 4.2 and G - 664.8 ± 46.2 compared with the initial indices (1 63.5 ± 6.5, 102 ± 4.1, 662.45 ± 45.3 mg /%, respectively).As the general and local signs of the inflammatory process were reduced in patients of this subgroup, a certain normalization of the laboratory indices of immunity studied by us was noted. So, before discharge from the hospital (9-10 days), the concentration of the CIC decreased to 0.167 ± 0.013 conv. units, while the initial indicator for admission was 0.262 ± 0.018 conv. units (P <0.001). After completion of treatment in inpatient conditions in patients with phlegmon of the maxillofacial area, before discharge, there was a significant positive trend in serum immunoglobulin values.Thus, the number of immunoglobulins M and G significantly increased on average to 130.63 ± 5.4 and 760.27 ± 49.5 mg%, respectively, compared with the initial and control values (P <0.001). At the same time, on the part of Ig A there were no significant changes compared with the previous group (P> 0.05).On study of immunity parameters at discharge from hospital on the background of the general satisfactory condition, a clean wound with signs of significant absorption of infiltrates, was noted a significant decrease in the concentration of the CIC to the level of 0.150 conv units. At the time of discharge the concentration of immunoglobulin A was 164.0 mg%, immunoglobulin M - 122.0 mg%, and immunoglobulin G was 988 mg%.We found that when sodium hypochlorite solution is used in complex treatment of phlegmon of the maxillofacial area, complicated by sepsis, thanks to its antiseptic (especially against obligate anaerobes) and necrolytic properties, contributed to a more rapid cleansing of the wound from purulent-necrotic masses and a noticeable increase in the growth of granulation tissue with underlying rapid decrease in the linear dimensions of purulent wounds, accompanied by an earlier resorption of infiltrates. This, in turn, laid the groundwork for improving the immunological status of the patient's organism due to the effective elimination of bacterial antigens, toxins, purulent detritus from the foci of acute odontogenic infection.In recent years, there has been an intense search for effective ways to treat phlegmon of the maxillofacial area with a complicated course. All this has led to the inclusion of intravascular laser blood irradiation (ILBI) into the complex of therapeutic measures, which according to a number of researchers has an immunocorrective effect. In order to increase the effectiveness of complex treatment of maxillofacial area phlegmon, complicated by sepsis, in 19 patients, in the complex of therapeutic measures were additionally included ILBI and courses of local irrigation of wounds with sodium hypochlorite solution. It should be emphasized that the general condition of patients, body temperature, pulse rate, as well as immunological indicators on the day of admission, i.e. before surgery (Fig. 1, 2), did not significantly differ from the same indicators in patients in the previous subgroup of clinical observations.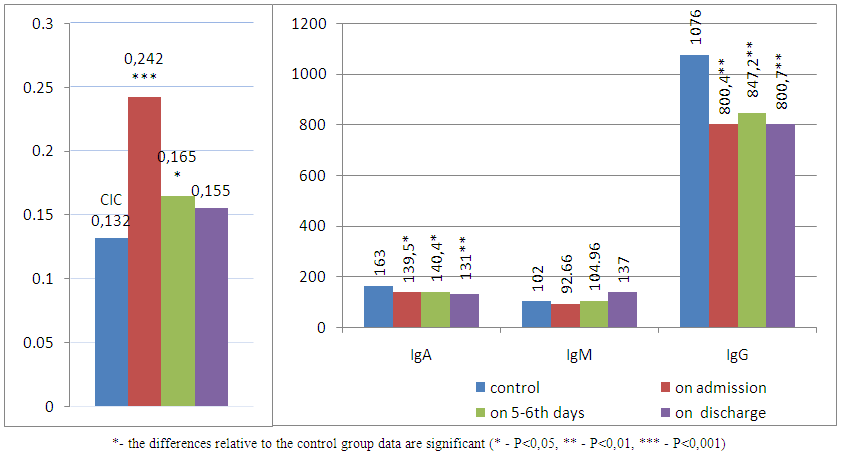 | Figure 3, 4. Indicators of the CIC and immunoglobulin A, M and G content dynamics in intensive therapy + ILBI+ NaClO3 of phlegmon maxillofacial area and their complications |
As a result, on the background of the general satisfactory condition, the cleansing of wounds from purulent-necrotic masses and significant decrease in infiltrates with signs of tissue regeneration and reduction in wound size in this patients subgroup, on the 6-7th days of complex treatment were noted also a significant (P<0.05) decrease in the CIC level (average to 0.165±0.013 conv. unit) in comparison with the initial indices (0,242±0,016 conv units). Although these parameters were still significantly (P<0,05) higher than the control values (0,132+0,07 conv units) (Fig. 3,4). In the study of the immunoglobulin level dynamics in patients of this subgroup on 6-7 days of complex treatment were noted positive changes in adaptive immunity. In particular, slightly increased the level of IgM, G, in contrast to the level of IgA, where there was a significant decrease (on average to 122.9 ± 4.9 mg%). Moreover, all these indicators of adaptive immunity still significantly exceeded the level of the corresponding values in practically healthy individuals (P <0.01). At the stage of discharge of patients from the hospital (9-10 days), the level of the CIC decreased on average to 0.155 ± 0.015 conv. units, but still significantly exceeded the control values. There was a significant increase in the level of immunoglobulin A. M and G, on average, to 139.9_ + 4.3. 167.83 ± 5.9 and 834.12 ± 55.66 mg% (p <0.05, P <0.001), P <0.01), respectively, compared with the control.Recently, great importance has been attached to medical methods of treatment using new highly effective therapeutic factors with powerful bactericidal and bacteriostatic properties in the treatment of acute purulent-inflammatory diseases of the maxillofacial area. Given this, the complex of therapeutic measures of 9 patients of the third subgroup of clinical observations, in which the phlegmon of the maxillofacial area was accompanied by severe sepsis, was strengthened by including local anti-inflammatory therapy, and a double wound irrigation with fresh sodium hypochlorite solution.The general condition of this subgroup of patients, body temperature, pulse, adynamia, as well as immunological parameters on the day of admission to the operation (Fig. 1, 2, 3, 4) did not significantly differ from those of the previous group. The content of the CIC in the blood of patients was almost 2 times higher than the same indicators level of donors: 0,258 ± 0,020 conv units vs. 0.132 ± 0.008 conv units in the control. After 6-7th days of treatment, the analysis of laboratory parameters of adaptive immunity showed a significant reduction in CIC (P <0.001) level in the blood of all 9 patients: an average of up to 0.182 ± 0.011 conv. units (P <0.001). Before discharge from the hospital for 9-10th days, was noted a further decrease of CIC content was noted on average to 0.172 ± 0.012 conv. units compared with baseline (P <0.01).However, they still significantly exceeded the control values (P <0.01). As shown by the results of our study, there was a statistically significant decrease (P <0.001) of the content of IgA in the blood upon admission to the hospital. After carrying out a complex of therapeutic measures on the 6-7th day, after reinvestigation level of the immunoglobulin A continued to remain at the same level. After the completion of such multicomponent therapy, patients showed only a slight increase in the content of IgA (P <0.001) in the blood compared to the previous study period. In the study of the dynamics of Ig M on the day of admission, a significant increase was observed in its concentration compared to same indicators in donors (P> 0.05). After the complex of therapeutic measures with double irrigation of the wound with a freshly prepared solution of sodium hypochlorite for 6-7 days, according to the results of repeated analyzes, no special changes were observed in its blood content. A statistically significant increase in the level of serum immunoglobulin Ig M (P <0.05) was noted before discharge from the hospital.The results of the study of Ig G content showed that on the day of admission there was a significant decrease (P <0.001) of its concentration compared with the level of control. After 6-7 days of complex intensive treatment, there was a tendency towards a further significant decrease in its concentration (p <0.001). At the end of complex intensive therapy, it was observed a significant increase of its content in blood (p <0.001) compared with the previous study period.Twice daily irrigation of the wound with sodium hypochlorite included, in the complex treatment of maxillofacial area phlegmons, led to a fairly rapid decrease in the CIC level and an increase in the production of body immunoglobulins, and ultimately to a reduction in the length of hospital stay. However, it should be noted that before discharge from the hospital, in patients the CIC level was still remaining significantly (P <0.05) elevated, compared with the control group. Recently, great importance is attached to the joint use of highly effective physical (UV irradiation of blood) and drugs in the treatment of acute purulent-inflammatory diseases of the maxillofacial area with a complicated course, in particular with sepsis. We have treated 14 patients who had odontogenic phlegmons of the maxillofacial area, complicated by severe sepsis. They constituted a separate group of clinical observations as in all these 14 patients, in contrast to the previous subgroup of patients, in the treatment complex (5 sessions) was additionally included UV irradiation of blood with a twice a day irrigation of the wound, with freshly prepared sodium hypochlorite solution. The general condition of all patients of this group was assessed as severe, the body temperature reached 40.5°C, and the pulse rate reached 130 beats per minute.Immunological studies conducted directly before the surgery showed an increase in the CIC concentration by 2.2 times (P <0.001) in the blood of patients of this subgroup compared with the corresponding indicators in the control. After carrying out a complex of therapeutic measures with repeated analysis on the 6-7th day of treatment, there was a significant (P <0.05) decrease in the CIC content in the blood, on average, 0.157 ± 0.09 conv. units. Continuation of intensive therapeutic measures contributed to a further decrease in the CIC concentration in patient’s blood. Before discharge from the hospital, the content of the CIC in patients of this subgroup was 0.147 ± 0.011 conv units. The results of the study showed that on the day of admission there was a significant (P <0.05) decrease in blood IgA.In reinvestigation on 6-7th days of the complex treatment, no specific changes in the content of immunoglobulins A in the blood were observed. By the time of completion of the inpatient treatment of patients in this subgroup of clinical observations, was recorded further significant (P <0.05) decrease in this indicator of adaptive immunity. In the study of immunoglobulin M content a slightly different picture was observed. The results of the study showed that on the day of admission there was only an insignificant decrease in their content in blood compared with the indicators in the control group of clinical observations. After the complex treatment with reanalysis on the 6-7th day, there was an insignificant increase in immunoglobulin M compared with the data of healthy individuals. Continued use of a combination of therapeutic measures in them contributed to a further significant (P <0.01) increase in the blood content of immunoglobulin M. Immunological studies of the content of immunoglobulin G carried out immediately before surgery and the appointment of complex intensive therapeutic measures showed a significant (P <0.01) decrease of their content in the blood. After opening, the wounds were irrigated with sodium hypochlorite solution, drained and was applied aseptic dressing. Patients were prescribed a comprehensive drug therapy, including five sessions of UV irradiation of blood (once a day) and irrigation of the wound with a solution of sodium hypochlorite twice a day.As the results of observations have shown, the general condition of this group of patients improved noticeably already on the 3rd-4th day after the beginning of treatment. Body temperature and pulse rate were approaching the physiological values; the wound cleansing with granulation and absorption of infiltrate also took place 1-2 days faster than in the patients of the previous group.It is established, that after several sessions of UV irradiation of blood on the background of a general satisfactory condition in patients of this group there was a marked decrease in the concentration of the CIC - on average to 0.157 ± 0.011 conv. units, which was significantly lower than the baseline (P <0.05), and there were also positive changes in the levels of immunoglobulins (M, A, G), compared with baseline values. As follows from the presented figures the level of serum IgA after 6-7 days after the start of treatment increases, on average, to 140.42 ± 9.3 mg%. The level of immunoglobulin M and G by this time was still elevated compared with baseline, and averaged 104.96 ± 12.4 and 847.21 ± 58.1 mg% (P <0.01), respectively and after 2-3 sessions of UV irradiation of blood and 4-5-fold irrigation of the wound with sodium hypochlorite, the wounds were completely cleared of necrotic tissue. In the course of complex treatment, patients also experienced a marked decrease in the linear dimensions of the wound due to a more rapid contraction of its edges compared with the previous group.Prior to discharge from hospital, the CIC decreased to the level of control values. The level of immunoglobulin M significantly exceeded the control indicators (P <0.01) and the data obtained at the previous stage of treatment (P <0.01). The concentration of Ig A in the blood of patients, according to our data, during the entire period of inpatient treatment did not undergo any noticeable dynamics. (Fig. 1, 2, 3, 4).Obviously, in severe cases of phlegmon of the maxillofacial area, complicated by severe sepsis, in patients studied by us found a sharp decrease in the immunological reactivity of the organism.
4. Discussion
Currently, appeared new antiseptic agents that have the ability to affect not only the pathogens, but also accelerate the purification of the wound, reduce intoxication, improve local immunity, i.e. that have multidirectional anti-inflammatory properties.Now the arsenal of such drugs has been replenished with one more, the active substance of which is sodium hypochlorite, containing hypochromic acid in its composition. During the study of the effects of sodium hypochlorite on the immune system, it is recorded its immunomodulating effect [7,13,16]. When a solution administered intravenously at a concentration of 5 mg / l, caused a powerful induction of IgM and a cellular response, and higher concentrations had immunosuppressive effect depending on the concentration. The data obtained served as the basis for introduction of it into clinical surgical practice (detoxification, the effect on pathogens of purulent infection, the improvement of microcirculation, necrolytic effect) [18,19]. In recent years, there has been an intensive search for effective ways to treat phlegmon of the maxillofacial area with a complicated course. The mechanism of intravascular laser radiation of blood in patients with phlegmons of the maxillofacial area complicated with sepsis is not sufficiently studied. Pavlova T.N. (1993) showed a positive effect of laser radiation on the course of phlegmon of the maxillofacial area. This was a reason to include intravascular laser irradiation (ILBI) into the complex of therapeutic measures, which according to the data of a number of researchers has an immunocorrective effect [6,21]. As F. Wennig and E. Knott’s studies have shown the quantum hemotherapy helps to stimulate phagocytosis, increase the number of T-lymphocytes and neutrophilic granulocytes, which play an important role in the immune responses of the body. It should also be borne in mind that in normal immunological reactivity (normaergy), the significance of the bacterial factor is not decisive in the development of the inflammatory process. Pathological reactivity (hypo-, hyper-anergy) reduces bacterial resistance and there is a possibility of purulent infection. It should be noted that the majority of researchers did not perform a complex assessment of the immune status of patients with purulent and inflammatory diseases of MFA, and studied one or another of its indices. So, when studying one of the important factors of the adaptive immunity - immunoglobulins, a significant decrease in the content was established. In the course of treatment, this indicator increased and reached the norm by the end of treatment. Prolonged reduction of this immunoglobulin, according to the authors, is an unfavorable prognostic sign of the disease. The amount of immunoglobulin G increases in the acute period of development of phlegmon, which indicates the stimulation of the body's defenses. The IgM content at admission fluctuated both upwards and downwards. In the study of the adaptive immunity in patients with MFA phlegmon it was found decreased immunoglobulin M and G. At the same time, in a severe clinical course of purulent-inflammatory process there was a decrease in all studied classes of serum immunoglobulins, which, according to the authors, indicates a suppression of adaptive immunity. Such a difference in the content of serum immunoglobulins in patients with phlegmons of MFA depends on the prevalence, severity and duration of the purulent - inflammatory process, which is the basis for a deeper study of this issue. Among the immunological factors determining the course of inflammatory disease, the circulating immune complexes (antigen - antibody) - CIC are of great importance. The formation of these complexes is one of the mechanisms of immune response aimed at neutralizing the antigen of various origins. Normally, the phagocytic cells constantly monitor the level of CIC in the blood. Therefore, the high content of immune complexes indicates the violation of phagocytosis. Despite the important role of CIC in the pathogenesis of immune inflammation, there is a small number of studies on their study in patients with purulent-inflammatory diseases. At the same time, the level of CIC in blood serum of patients with odontogenic inflammatory diseases was studied only in isolated studies. As follows from studies it was found that the concentration of immune complexes increased by more than 2 times and positive correlation between the CIC and immunoglobulins A, M and G was revealed. All this give a reason to consider that immune complexes are important components in the pathogenesis of odontogenic inflammation. Therefore, the study of the dynamics of the CIC contributes to the objective prediction of the course of purulent-inflammatory diseases of the maxillofacial area [15, 16]. In order to reduce or eliminate of the complicated course of phlegmon of the maxillofacial area, four treatment methods are used: combination of intensive drug therapy with one-time irrigation with sodium hypochlorite solution; intensive therapy with one-time irrigation of wound with sodium hypochlorite and ILBI; intensive therapy of two-time irrigation of wound with sodium hypochlorite and intensive therapy with two times irrigation of wounds with sodium hypochlorite solution in combination with UV irradiation of blood. The above methods, except for the last method, did not lead to a significant positive shift in clinical and laboratory parameters. Inclusion of UV irradiation of blood in the complex therapy in combination with local irrigation of purulent wounds with sodium hypochlorite resulted in recovery of shorter terms (on the average 9,8±0,08 days), improvement of the general condition of patients according to the clinical parameters of local dynamics of the disease and recovery of the violated parameters of adaptive immunity. According to the literature, UV irradiation of blood contributes to the activation of nonspecific protection factors, increase of erythropoiesis, lymphoid and leukopoiesis, increase of bactericidal activity of plasmas, which are confirmed by us during the studying the dynamics of these indicators in our patients. It was established, that the use of UV irradiation of blood and the local bactericidal activity of sodium hypochlorite contributes to a significant positive dynamics of the adaptive immunity indicators studied by us and cleansing the wound from purulent-necrotic masses.
5. Conclusions
Thus, the performed treatments in the comparative aspect of complicated phlegmon of the maxillofacial area showed that the combination of intensive therapy with single and double irrigation of wounds by freshly prepared sodium hypochlorite solution does not lead to noticeable positive results. At the combined application of intensive therapy with ILBI and single irrigation of wounds with sodium hypochlorite solution, a noticeable improvement of clinical and laboratory parameters was noted in patients with maxillofacial area phlegmons. Significant positive changes in immunological and clinical parameters are observed in patients with severe course of phlegmons of the maxillofacial area in cases of combination of intensive drug therapy with double irrigation of wounds with sodium hypochlorite and 5 time ultraviolet irradiation of blood.
References
| [1] | Abelevich AI, Surgical sepsis: method. recommendations. Abstract of diss. cand of med sciences. Nijny Novgorod, 2007; 30. |
| [2] | Agapov V.S., Tsarev V.N., Piminova I.A. Clinical and laboratory analysis of the results of local application of perftoran in the complex treatment of patients with odontogenic phlegmons. Institute of Dentistry. 2005; 2: 50-52. |
| [3] | Agapov V.S., Emelyanova N.V., Shapkova, T.P. Anesthesiology, reanimation and intensive care: Textbook. M., 2005; 256. |
| [4] | Alekseeva Yu.V. Etiological diagnosis and optimization of the treatment of inflammatory diseases of the maxillofacial area based on the determination of genetic markers of microorganisms of pathogens: Abstract of diss. cand of med sciences. Moscow 2005; 27. |
| [5] | Amkhadova M.A., Shalabayev O.D. Preoperative preparation of patients with severe odontogenic phlegmon. Stomatology (Moscow) 2011; 1: 35-36. |
| [6] | Bazhanov N.N., Aleksandrov M.T. Application of methods of laser fluorescent diagnostics in purulent surgery. Stomatology (Moscow) 2002; 1: 48-51. |
| [7] | Batirbekova F.R. The use of low-frequency ultrasound for the treatment of wounds with sodium hypochlorite in the complex treatment of maxillofacial area phlegmon: Abstract of diss. cand of med sciences. Moscow 1999; 23 |
| [8] | Bernadsky Yu. I. Basics of maxillofacial surgery and surgical dentistry (3rd edition). Moscow2003; 167 |
| [9] | Bogatov V.V., Burov N.M. The relevance of prevention and treatment of maxillofacial area diseases. Technologies of the XXI century in dentistry and maxillofacial surgery: materials of scientific. - practical conf. Dentists and maxillofacial surgeons of the Central Federal District of the Russian Federation with international participation. Tver, 2008; 22-23. |
| [10] | Bulygin G.V., Kamzalakova N.I., Solonchuk Y.R. Opportunities to improve the effectiveness of the treatment of purulent surgical infection. Surgery 2010; 5:56-62. |
| [11] | Varyushina E.A., Kornusova V.G., Simbirtsev A.S. Study of the local immunostimulating action mechanism of interleukin - 1β. Immunology 2000; 3: 18-22. |
| [12] | Veksler N.D. Immunocorrection in complex treatment of patients with abscesses and phlegmon of maxillofacial area. Abstract of diss. cand of med sciences. Irkutsk, 2002; 23. |
| [13] | Miroshnichenko A.G., Orlov A.B., Kocherovets V.I. Influence of sodium hypochlorite obtained electrochemically on the change of cell membrane properties (in Russian). Electrochemical methods in medicine. Dagomys, 1991; 13. |
| [14] | Yermolin D.V. Agapov V.S., Tsarev V.N. Influence of ozone therapy on the immune status of patients with odontogenic phlegmons (in Russian). Collection of scientific articles of the All-Russian Conference Moscow. 2002; 55-56. |
| [15] | Vyseletseva Yu.V. Clinical and immunological properties of the course and prognosis of the generalized odontogenic phlegmons of the maxillofacial area and their complications: Abstract of diss. cand of med sciences. Voronezh, 2011; 17. |
| [16] | Gaivoronskaya T.V. Optimization of treatment of patients with odontogenic phlegmons of the maxillofacial area (experimental clinical basis) Abstract of diss. Doctor of med sciences. Мoscow, 2008; 49. |
| [17] | Gendugova, O.M. Pathogenetic substantiation of the complex therapy of the patients with the purulent-inflammatory diseases of the maxillofacial area Abstract of diss. cand of med sciences. St. Petersburg, 2011; 27. |
| [18] | Petrosyan E.A., Sergienko V.I., Kulaev G.K. Sodium hypochlorite in the treatment of purulent wounds. Surgery info 1991; 1: 40-43. |
| [19] | Glukhov A.A., Korotkikh N.G., Azarova T.V. Reduction of terms of stationary treatment of patients with phlegmons of maxillofacial area and neck on the background of complex treatment with application of microdispersed flows of anolyte solution (in Russian) // Newspaper of new medical technologies. - Tula, 2013; 2: 291-294. |
| [20] | Nedelko N.A., Codet A.H., Petrosyan N.E. Purulent-inflammatory diseases of the maxillofacial area; main causes of development. Collection New Millennium Stomatology Мoscow 2001; 409-410. |
| [21] | Pavlova T.N. The use of helium-neon irradiated blood in the complex treatment of patients with phlegmons (in Russian) // Stomatology. 1993; 1: 16-19. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML