-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2019; 9(8): 302-306
doi:10.5923/j.ajmms.20190908.06

Evaluation of the Coronary Plaque Stability by Volumetric MDCT-coronary Angiography: Stable and Unstable Forms of Angina
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLA. I. Ikramov, M. M. Zufarov, N. M. Djuraeva, A. T. Amirhamzaev, M. M. Maksudov, N. T. Vakhidova, A. T. Sultanov, N. K. Makhkamov
Republican Specialized Scientific and Practical Medical Center of Surgery named after academician V.Vakhidov, Tashkent, Uzbekistan
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Introduction: Early, preclinical identification of patients with coronary atherosclerosis and a high risk of coronary complications development is the most important task of a cardiologist and requires studying the possibilities of non-invasive techniques, such as MDCT-coronary angiography. The progress of MDCT has led to a sharp surge of radiologists’ interest around the world to examine patients with coronary heart disease. Aim: To study the possibilities of volumetric MDCT-coronary angiography in the differentiation of patients with unstable and stable forms of coronary heart disease at the non-invasive examination stage depending on the type of atherosclerotic plaque. Materials and methods: 308 patients with coronary heart disease aged from 37 to 77 years, whose average age was 59.6 ± 0.61 years were examined. 209 (68%) of them were males and 99 (32%) – females. All patients were performed volumetric low-dose MDCT-coronary angiography using a 640-slice volumetric scanner. Results: The analysis results of the lesion level of all segments of the coronary arteries according to the MDCT-coronary angiography data in patients with coronary heart disease revealed significant differences. In patients with unstable angina compared with stable angina, the occurrence frequency of coronary artery stenoses from 50% to 75% was significantly higher by 2.6 times (χ2 = 22.8 p <0.0001), coronary artery stenosis higher than 75% - by 2.2 times (χ2 = 8.77 p = 0.003), occlusions – by 4.8 times (χ2 = 25.99 p<0.0001). Therefore, in patients with unstable angina destabilization of the clinical condition gas been stipulated by the presence of significant coronary artery stenosis and unstable soft-tissued atherosclerotic plaques. Conclusion: MDCT-coronary angiography is a highly informative method for assessing the condition of the coronary arteryes in patients with coronary heart disease which allows to reveal the presence, degree and extent of coronary lesion, as well as to determine the type of atherosclerotic plaque.
Keywords: Coronary artery, Volume computed tomography, Stable angina, Unstable angina, Invasive coronary angiography, Diagnostic informativeness
Cite this paper: A. I. Ikramov, M. M. Zufarov, N. M. Djuraeva, A. T. Amirhamzaev, M. M. Maksudov, N. T. Vakhidova, A. T. Sultanov, N. K. Makhkamov, Evaluation of the Coronary Plaque Stability by Volumetric MDCT-coronary Angiography: Stable and Unstable Forms of Angina, American Journal of Medicine and Medical Sciences, Vol. 9 No. 8, 2019, pp. 302-306. doi: 10.5923/j.ajmms.20190908.06.
Article Outline
1. Introduction
- In the last decade, due to the enormous significance of cardiovascular pathology which occupies a leading position in the list of the socially significant diseases, the interest of scientists all over the world to the study of the heart and vessel calcification, as well as the definition of the atherosclerotic plaque (ASP) has increased significantly [1]. The problem of the coronary arteries (CA) and the heart diseases has attracted the attention of scientists since the days of Virchow [2], but even today there are still many “white spots” and unclear issues in this problem that are pending. These include the causes and pathogenesis of coronary heart disease (CHD), association with atherosclerosis (AS) of CA, determining the type and stability of ASP, indications for screening of coronary Ca. Early, preclinical identification of patients with coronary atherosclerosis and a high risk of coronary complications development is the most important task of a cardiologist and requires studying the possibilities of non-invasive techniques, such as MDCT- coronary angiography (CA). The progress of MDCT has led to a sharp surge of radiologists’ interest around the world to examine patients with CHD [4,10].A proved high diagnostic efficacy of MDCT CA puts this technique in the first place among screening tests for the presence of coronary atherosclerosis. This technique allows non-invasively, quickly and accurately detect the presence of ASP in the CA, determine the type of ASP, assess the degree of stenotic lesion and clarify the indications for choosing a method of preventing or treating CHD [1,3]. At the same time, MDCT CA is subjected to valid criticism due to radiation exposure, the impossibility of examining patients with arrhythmia, the need to use beta blockers before the study and because of the relatively low specificity of the technique compared with coronary angiography (CAG) [9].
2. Aim
- To study the possibilities of volumetric MDCT- coronary angiography in the differentiation of patients with unstable and stable forms of coronary heart disease at the non-invasive examination stage depending on the type of ASP.
3. Materials and Methods
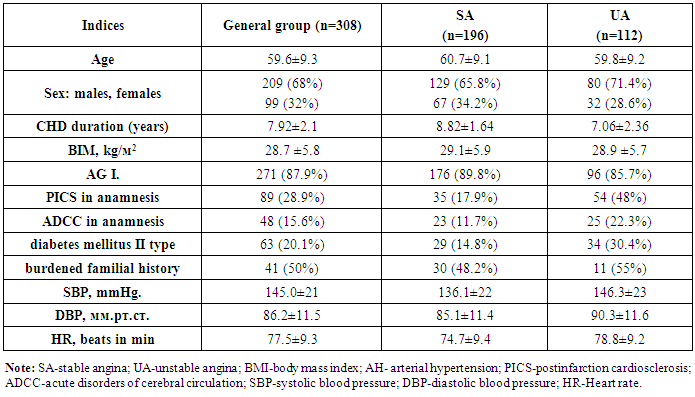
- 308 patients with coronary heart disease aged from 37 to 77 years, whose average age was 59.6 ± 0.61 years were examined. 209 (68%) of them were men and 99 (32%) - women. All patients were conducted volumetric MDCT CA on a 640-slice CT scanner (detector width 16 cm) with a tube rotation speed of 0.275 sec., with intravenous introduction of a contrast agent in the amount of 0.75 ml / kg, the voltage on the tube was 100 kV, the current strength was 600-900 mA, radiation dose (RD) in prospective mode 1.4-3.5 mSv [5]. All patients, depending on the clinical variants of CHD were divided into 2 groups: The first group consisted of 196 patients with unstable (progressive) angina of FC II by E. Braunwald et all. (1989) whose average age was 60.7 ± 0.92 years. There were 129 (65.8%) males and 67 (34.2%) females.The second group included 112 patients with stable angina of FC II-III, whose average age was 59.8 ± 0.82 years. There were 80 (71.4%) males and 32 (28.6%) females (Table 1).
|
4. Results and Discussions
- The examination results of patients with CHD were analyzed depending on the form of the angina: stable angina (SA) and unstable angina (UA). The possibilities of MDCT CA in the differentiation of patients with SA and UA forms of CHD were studied depending on the type of the ASP in the non-invasive examination stage. According to the data obtained from the biochemical blood analysis, no statistically significant differences were found between the groups. When analyzing the anatomical characteristics of coronary lesions, such as the frequencies of one-, two-, and multi-vascular lesions, it was found that in the group with UA, the absence of CA angiographic lesion was statistically significantly more frequent (14.8 vs. 8%, p = 0.04). It testifies that the pain behind the sternum, which made suspect UA in these patients, actually had a non-coronary nature. Similar differences were found when analyzing the distribution of CA in patients with SA and UA forms of CHD in the presence by calcification of CA (Fig 1).
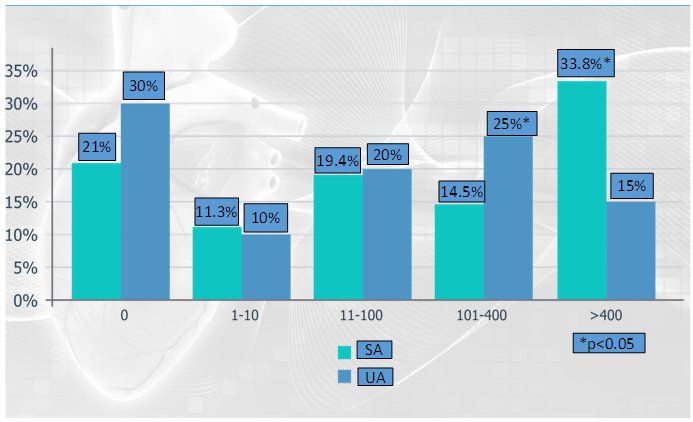 | Figure 1. The distribution of patients depending on the indicator of coronary calcium index (CCI) (Note: SA- stable angina, UA – unstable angina) |
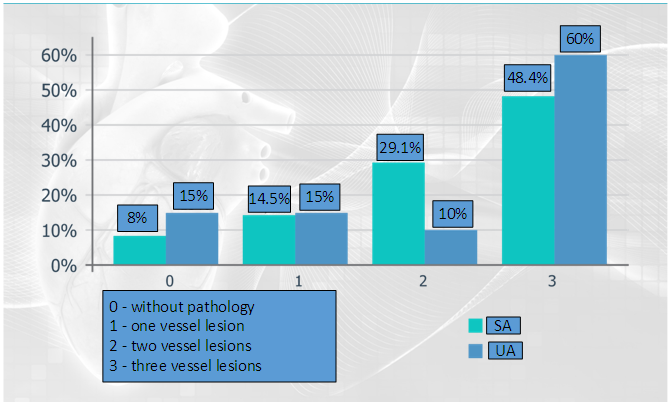 | Figure 2. Degree of coronary bed lesion in patients with stable and unstable forms of angina |
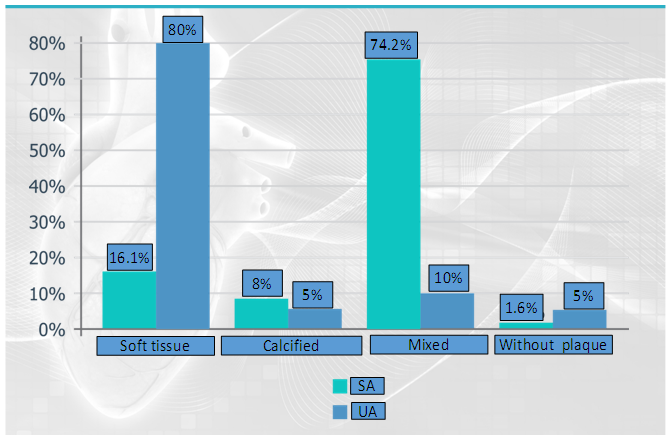 | Figure 3. Distribution of patients by atherosclerotic plaque type (Note: SA- stable angina, UA – unstable angina) |
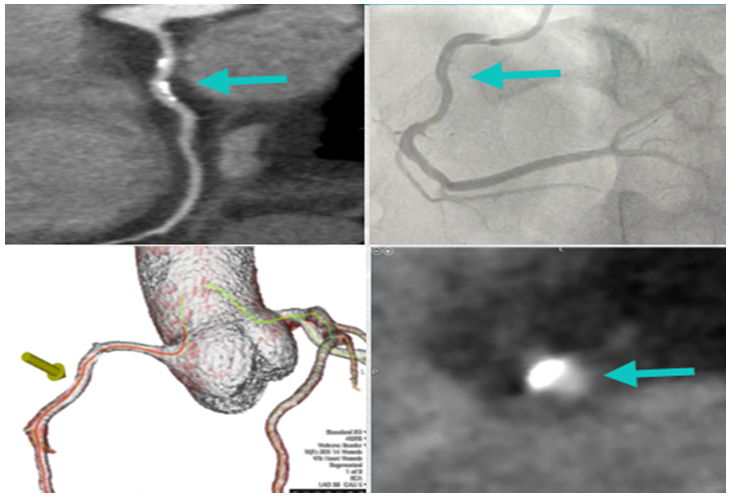 | Figure 4. MDCT CA and coronaroangiography images of the right coronary artery (RCA). Calcified ASP in the middle third of the RCA |
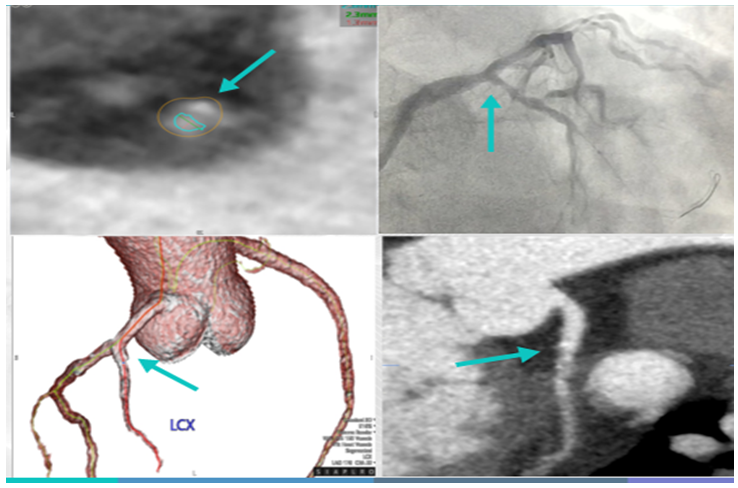 | Figure 5. MDCT CA and coronary angiography images of the left circumflex artery (LCX) with presence of STASP in the proximal third |
|

5. Conclusions
- MDCT CA is a highly informative method for estimation the condition of the CA in the patients with CHD, which allows to detect the presence, degree and prevalence of coronary lesion, as well as to determine the type of ASP. When comparing the MDCT CA pattern of CA lesion in patients with different clinical course of CHD (SA and UA) it was found that calcification of the CA was significantly less often (5.1% vs. 9.8%, p = 0.04), low CCI values were significantly often revealed (30.2% versus 21.0%, p = 0.034) and STASPs were detected (80.3% versus 16.1%, p = 0.005).