-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2019; 9(8): 281-283
doi:10.5923/j.ajmms.20190908.01

Cardiovascular Risk Assessment in Patients with Rheumatoid Arthritis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSaidova M. M.1, Kamilova U. K.2
1Bukhara State Medical Institute, Bukhara, Uzbekistan
2Republican Specialized Scientific-Practical Medical Center of Therapy and Medical Rehabilitation, Tashkent, Uzbekistan
Correspondence to: Kamilova U. K., Republican Specialized Scientific-Practical Medical Center of Therapy and Medical Rehabilitation, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The aim of the research was to study the structure and frequency of cardiovascular risk and comorbid diseases and to determine the total cardiovascular risk according to the mSCORE scale in patients with rheumatoid arthritis (RA). A retrospective study included 1190 RA patients who received treatment at the clinic of the Bukhara State Medical Institute. Of these, 932 (78.3%) were men and 258 (21.7%) were women. 458 patients were aged 35-49 years and 732 aged 50-60 years. Prediction of cardiovascular risk over 10 years was carried out using the mSCORE scale. The control group consisted of 35 healthy individuals. The frequency of occurrence of risk factors for cardiovascular diseases was assessed: heredity, smoking, hypercholesterolemia (HCh), abdominal obesity (AO), physical inactivity, frequency of arterial hypertension (AH), coronary heart disease (CHD), and diabetes mellitus in patients with RA. According to the results of the research on the SCORE, mSCORE scales, a very high risk on the mSCORE scale is 5.4%, which is 2.56 times more than on the SCORE scale.
Keywords: Rheumatoid arthritis, Cardiovascular risk, mSCORE scale
Cite this paper: Saidova M. M., Kamilova U. K., Cardiovascular Risk Assessment in Patients with Rheumatoid Arthritis, American Journal of Medicine and Medical Sciences, Vol. 9 No. 8, 2019, pp. 281-283. doi: 10.5923/j.ajmms.20190908.01.
1. Introduction
- Cardiovascular morbidity and mortality in patients with rheumatoid arthritis (RA) is higher than in the general population. The results of the multicenter studies showed that the increase in mortality in patients with RA is associated with the development of adverse cardiovascular events, including myocardial infarction and sudden coronary death [1,2]. The basis of the early development of atherosclerosis in RA patients, according to most researchers, are common immune-inflammatory mechanisms in the development of RA and atherosclerosis [3,4]. The concept of risk factors (RF) for atherosclerosis, developed on the example of cardiovascular pathology, has found its application in patients with rheumatic diseases. Arterial hypertension (AH) is the most important risk factor for cardiovascular complications, however, in patients with RA, there is a wide variation in the values of the prevalence of AH (from 16% to 76%), which is due to underreporting of the clinical characteristics of patients and the characteristics of antirheumatic therapy [5]. The role of endothelium, indicators of hardening of the arteries, heart rate variability in the development of cardiovascular pathology is being widely studied [6]. The development of cardiovascular complications in patients with RA is associated both with the influence of traditional risk factors, systemic inflammation, and the side effects of nonsteroidal anti-inflammatory drugs (NSAIDs) taken [7,8].NSAIDs by suppressing the activity of cyclooxygenase can lead to a decrease in systemic and renal synthesis of vasodilator prostaglandins, which causes an increase in vascular tone and fluid retention, accompanied by an increase in blood pressure and decompensation of chronic heart failure (CHF).The aim of the research: to study the structure and frequency of cardiovascular risk, comorbid diseases and to determine the total cardiovascular risk according to the mSCORE scale in patients with RA.
2. Materials and Methods
- A retrospective study included 1190 RA patients who received treatment at the clinic of the Bukhara State Medical Institute. Of these, 932 (78.3%) were men and 258 (21.7%) were women. 458 patients were aged 35-49 years and 732 aged 50-60 years. The frequency of occurrence of risk factors for cardiovascular diseases was assessed: heredity, smoking, hypercholesterolemia (HCh), abdominal obesity (AO), physical inactivity, frequency of arterial hypertension (AH), coronary heart disease (CHD), and diabetes mellitus in patients with RA. Prediction of cardiovascular risk over 10 years was carried out using the mSCORE scale. The recommendations of the European League against Rheumatism (EULAR) in patients with RA provided for assessment for cardiovascular risk on the scale of mSCORE, by calculating index SCORE multiplied by a factor of 1.5. The control group consisted of 35 healthy individuals.
3. Results
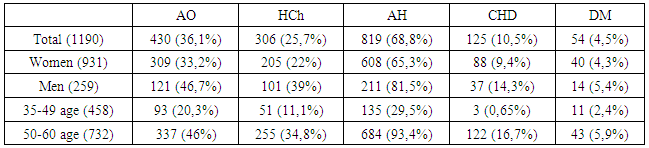
- The work was based on the results of a retrospective analysis of 1190 patients with RA who received treatment at the clinic of the Bukhara State Medical Institute. Of these women were 931 (78.2%) and men 259 (21.8%). 458 patients were aged 35-49 years and 732 aged 50-60 years. The diagnosis of RA was established using the ACR (1987) and ACR / EULAR (2010) criteria. The control group consisted of 35 healthy individuals. A retrospective analysis showed that 806 (67.7%) patients were seropositive for the rheumatoid factor and 384 (32.3%) patients with seronegative. An analysis of the main risk factors for cardiovascular diseases revealed that heredity was aggravated in 359 (30.2%) patients, smoking was found in 141 patients (11.8%). HCh was detected in 306 (25.7%) patients (Table 1). At the same time, HCh was significantly more common in men - 39% of cases versus 22% in women. AO was reported in 430 (36.6%) patients. Obesity occurred 3 times more often in patients aged 50–60 years and 2 times more often in men. AH occurred in 819 patients, which was 68.8%, while in patients aged 50–60 years AH occurred 5 times more often than in patients aged 35–49 years. CHD occurred in 125 (10.5%) patients: at the age of 35-49 years in 3 (0.65%) and in the age of 50-60 years in 122 (16.7%). Diabetes mellitus (DM) was in 54 (4.5%) patients, while in 11 (2.4%) patients aged 39–49 years and in 43 (5.9%) aged 50–60 years. According to the literature, the importance of the presence of risk factors for atherosclerosis (smoking, obesity, hypertension, hypercholesterolemia, diabetes mellitus, etc.) in the development of CVD in RA patients, the greater incidence of individual RF in RA compared with other rheumatic diseases.
|
 | Figure 1. The results of the study on the scales SCORE, mSCORE |
4. Discussion
- An increase in the risk of mortality from cardiovascular diseases can be traced already in the onset of rheumatic diseases and is associated with the presence of risk factors. Coronary atherosclerosis and related complications largely determine the clinical course and outcomes of a number of rheumatic diseases [9]. Analysis of literature reviews suggests that atherosclerosis is not so much a pathology associated with RA as a conjugate process of lesion of the cardiovascular system [10]. However, the lack of a clear understanding of the state of the cardiovascular system in various clinical variants of RA, both in combination with arterial hypertension (AH), and without AH in patients with rheumatoid arthritis impedes the development of adequate methods for preventing cardiovascular complications. Without assessing the severity of these disorders in RA patients, clarifying the characteristics of the functioning of the cardiovascular system in conditions of chronic systemic inflammation, it is impossible to understand the role of these factors in the development of cardiovascular pathology in RA.
5. Conclusions
- The association of RA and cardiovascular risk is the subject of close attention of rheumatologists and cardiologists. This is due, on the one hand, parallels the pathogenesis of atherosclerosis and RA, which is important for understanding the development mechanisms of both diseases. In this regard, it is important to timely assess the cardiovascular risk in patients with RA and the appointment of therapy aimed at reducing it. In patients with RA, the determination of the total cardiovascular risk on the mSCORE scale has important prognostic significance.