-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2019; 9(7): 259-261
doi:10.5923/j.ajmms.20190907.07

The Impact of the Term of Preliminary Traction and the Age on the Development of Aseptic Necrosis of Caput Femori after Conservative Therapy of Hip Dislocation
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLA. M. Jurayev1, I. M. Kadirov2
1Republican Specialized Scientific Practical Center of Traumatology and Orthopaedics, Tashkent City, Uzbekistan
2Republican Center of Children’s Orthopaedics, Kibray District, Tashkent, Uzbekistan
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

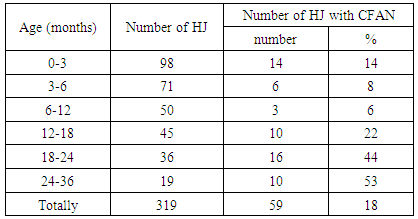
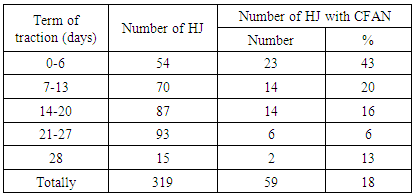
Background. The problem of the therapy of congenital hip dislocation (CHD) in children was always linked with sequlae appearing during and after the therapy. The objective. In this regard the objective of our study was to answer the question if duration of the functional traction effects the frequency of caput femori (CF) aseptic necrosis development and whether the age of CHD initial therapy had an impact on the further prognosis of hip joint (HJ) development as a whole. Materials and methods. We examined 276 patients (319 HJ), who had plaster traction before reduction of CHD. Patients were divided to groups according to age at the time of CHD primary therapy. Results. Out of 319 HJ fifty nine cases had development of CFAN (18%). The lowest parameter was detected in the group of patients from 3 to 6 months in 8%, while the highest one was determined in the age 24036 months, where it was equal to 53%. In cases of preliminary traction more than 3 weeks development of CFAN was equal to 6%. Conclusion. Duration of preliminary traction in conservative therapy of CHD is very important. Prognosis of complete development of HJ was significantly worse in children above 1 compared to those from 3 to 12 months.
Keywords: Hip joint, Congenital hip dislocation, Extraction, Caput femori aseptic necrosis
Cite this paper: A. M. Jurayev, I. M. Kadirov, The Impact of the Term of Preliminary Traction and the Age on the Development of Aseptic Necrosis of Caput Femori after Conservative Therapy of Hip Dislocation, American Journal of Medicine and Medical Sciences, Vol. 9 No. 7, 2019, pp. 259-261. doi: 10.5923/j.ajmms.20190907.07.
Article Outline
1. Introduction
- The term hip joint dysplasia (HJD) involves several anatomical alterations when there is disorder of caput femori (CF) and acetabulum (A) correlation, irregular development of HJ leading to the development of its instability. In developed countries frequency of HJD is 4-6 cases per 1000 alive-born neonates [1,2]. HJD is usually diagnosed within initial months of baby’s life with the help of screening orthopedic examinations and selective x-ray check-ups [3]. In cases when a positive Barlow (dislocation - sub-dislocation) or\and Ortolani symptoms, dislocation of CF and impossibility of its reduction or instability were detected in HJ by means of US, these patients were registered or started to be treated. The aim of the therapy was restoration of HJ congruency and to reach maximal functionally good result in spite of associated anatomical obstacles including muscle weakness, arthrosis or chronic pain.It is commonly accepted that for children with HJED at the age under 6 months abduction splints and other structures are used [4]. For children above 6 months old a closed reduction of CF is used in A with application of plaster bandages [4]. Some specialists apply preliminary traction prior to closed reduction. Study of case histories of patients shows that application of preliminary traction decreases the frequency of CF aseptic necrosis development (CFAN), developing after close reduction, and it diminishes the need of open reduction of CF [5,8]. However, the data of some authors do not confirm these results [9-12].
2. The Objective
- We performed our study to get answers to two questions. Does duration of functional traction effect the frequency of caput femori aseptic necrosis development and does the age when initial CHD therapy was performed have an impact on the further prognosis of hip joint development as a whole?
3. Materials and Research Methods
- In the Republican Center of Children’s Orthopedics of the MH of the RUz within 2010-2011 we observed more than 2500 patients with congenital hip dislocation and sub-dislocation. 276 of these patients with 319 congenital HJ dislocation were selected as we had complete information about these patients. Prior to reduction all patients had functional plaster traction, which gave us a chance to assess the efficacy of the procedure. As more than 2/3 of our patients were revealed and treated under 1 year old, we could also analyze the results of the therapy in that age group.The study involved patients with CHD without any associate pathology and complications of the basic disease. All patients who had primary treatment start at 36 months of life, patients who underwent surgery in 2 years after primary conservative therapy, and patients with HJ sub-dislocation or dysplasia were excluded from the study. Besides that, all HJ were followed up at least for 1 year after the primary therapy.Among 276 selected patients there were 238 girls and 38 boys. One hundred and twenty eight patients had left side CHD, 105 had right-side dysplasia, while bilateral one was observed in 43 of the patients, totally 319 HJ. In our research with the help of x-ray and MRI we determined the following alterations in the development of CFAN: fragmentation, rise of density, flattening and heterogeneity of CF ossific nucleus, shortening and widening of neck of femur, protuberance of medial metaphysic, and disorder of CF ossific nucleus appearance and growth.Though most of researchers state that in case of CHD the CF ossification center is visualized later and stays small for a longer term or does not appear at all, we observed four relevant unusual cases. In these cases there was earlier appearance of ossification center or greater size of ossification center of the damaged side compared to healthy side of the opposite HJ.In the age under 3 months primary therapy was performed in 98 cases of CHD; in 71 cases it was done within the period from 3 to 6 months and in 50 CHD cases in the age from 6 to 12 months. Thus, 68% of the patients received primary therapy before they were 1 year old.All patients had adhesive plaster traction in flexion and abduction position in hip jopint not more than 90°. The strength of traction was changed dependently on the age, size of baby and condition of a child’s skin, while in rare cases the load was over 1.5 kg (varied from 0.9 to 2 kg). traction was considered to be successful when CF ossification center dipped to Y-shape cartilage. In the patients without ossification center that parameter was evaluated according to the restoration of Shenton’s line. After that a close reduction was performed with anesthesia; plaster was applied in Lorenz I position. The plaster was removed three months later, and after that a patient wore Vilenski’s splint.
4. Results
- We performed comparison of CFAN development in the age aspect (Chart 1).
|
|
5. Discussion
- Trueta et al. [11] described the complete CF circulation in neonates and the period of early childhood. Damage f vascular lumen of developing CF can lead to the dysfunction of ossification center, dilution of growth area, disorder of stop of longitudinal growth of femoral bone. Strobino et al., Salter and Field, Trias and Trueta [11] studied the impact of pressure on joint and growth cartilages in detail. In relation to that traction is applied for an adaptation of contracted soft tissues surrounding HJ.A question about early open reduction of CHD in children under 2 arises due to the presence of these results of conservative therapy. Though it should be noted that local and foreign references are overfilled by reports of positive results of conservative therapy. Our study revealed noticeably bad results of conservative therapy of CHD with application of traction among children above 1. Prevalence of CFAN among children under 3 causes anxiety. During that period ossification center is not determined on x-ray images. That is why aseptic alterations are not revealed in time even in very severe cases. Out study confirmed our suggestion that cartilage part of CF is partially tend to aseptic alterations.
6. Conclusions
- Following conclusions were made in the result of detailed study of the results of the therapy in 319 cases of CHD:1. The term of preliminary traction in conservative therapy of CHD is very important. The lowest prevalence of CFAN was determined in the cases of traction term from 21 to 28 days before close reduction.2. Prognosis of complete development of HJ was much worse in children above 1 compared to the patients from 3 to 12 months old.3. CFAN prevalence among the children under 3 months was higher (14%) than that among 3-12 months old children.4. Metaphysis alterations noted in WTB of neonates prior to X-ray detection of ossification center serve to be pathognomic in CFAN diagnostics.