-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2019; 9(7): 255-258
doi:10.5923/j.ajmms.20190907.06

Pulmonary Complications as an Immediate Cause of Death at Craniocerebral Injury
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMasharipov Azamat Cabirovich
Tashkent Medical Academy, Tashkent, Uzbekistan
Correspondence to: Masharipov Azamat Cabirovich, Tashkent Medical Academy, Tashkent, Uzbekistan.
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The absence of sufficiently complete and clear information in the literature about the complexes of morphological changes in the respiratory system upon the death from craniocerebral injury in medical institutions indicates the need for in-depth studies in this direction. A study of the respiratory system in the death cases from craniocerebral injury has been carried out. The results showed that the deaths of inpatients at various stages of experiencing a closed craniocerebral injury at the scene are characterized by features of the morphological changes of the lungs, represented by a sequential change in the processes of circulatory disorders and pulmonary ventilation, inflammation.
Keywords: Craniocerebral injury, Morphology, Blood circulation, Pulmonary ventilation
Cite this paper: Masharipov Azamat Cabirovich, Pulmonary Complications as an Immediate Cause of Death at Craniocerebral Injury, American Journal of Medicine and Medical Sciences, Vol. 9 No. 7, 2019, pp. 255-258. doi: 10.5923/j.ajmms.20190907.06.
1. Introduction
- The practice of forensic medicine shows that in a significant number of death cases (up to 23%) from craniocerebral injury (CCI), the death of victims occurs as a result of secondary changes that have developed in a period of time from several minutes to several hours or more from the moment of injury, including the provision of medical care in hospitals. Pulmonary edema and pneumonia as “secondary changes” are diagnosed by forensic experts when examining corpses in 17.5-76.6% of all cases of CCI [5, 8], whereas in general the number of post-traumatic pneumonia reaches 35.1% [6, 9]. A common complication of CCI in neurosurgical practice is pneumonia [1, 4], which is diagnosed in 19.5% -57.1% of CCI cases [2, 3, 12]. Currently, the development of purulent complications is associated with nosocomial infection, excluding the possibility of infection of patients before the start of invasive procedures [7, 10-11]. In this regard, the development of pneumonia as a complication of a closed CCI is of interest. The absence of sufficiently complete and clear information in the literature about the complexes of morphological equivalents of adaptation processes in the respiratory system, data on the influence of exogenous and endogenous factors on the level of structural reorganization of this system at the death cases from CCI in medical institutions indicates the need for in-depth studies in this direction.Aim of the study was to improve the quality and evidence of expert findings on death from CCI in hospitals in cases of complications of the respiratory system.
2. Material and Methods
- The study included only those cases of CCI when the time of injury and death was known as the main criterion in studying the morphological changes of the lungs was the time of death on the scene of the CCI. 140 cases of severe CCI with lethal outcome have been analyzed.
|
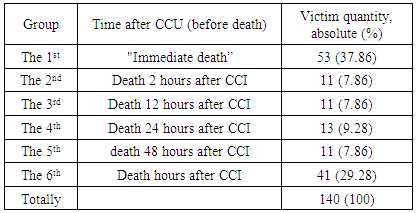
3. Results and Their Discussion
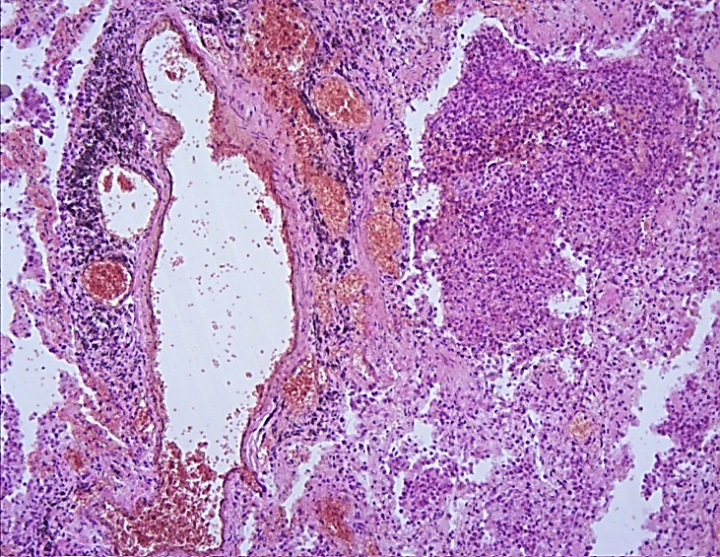
- A macroscopic examination of the corpses of persons who died in the result of a mechanical injury at the scene and a microscopic examination of the lungs revealed a complex of morphological equivalents of the pathological processes occurring in the lungs at this nosology. All victims in the study group died in the result of severe craniocerebral injury. In 32% of cases CCI was combined with mechanical trunk injury in the form of 1-3 ribs fractures without damage of the parietal pleura and ruptures of the abdominal cavity. In 46% of cases ethyl alcohol was detected in the blood. The severity of CCI was determined by the presence of the skull bones fractures (in 68% of cases), severe and mild cerebral contusions in combination with spotted or restricted diffuse subarachnoid hemorrhages. In 84% of cases hemorrhages to the ventricles of the brain were detected, in 32% of cases injuries of the lower stem section of the brain was diagnosed. Subdural hematomas with no signs of compression of the cerebral hemispheres were diagnosed in 78% of cases and in 26% intracerebral hemorrhages were found in the section. A macroscopic examination of corpses in 9 from 10 studied cases determined the first degree of venous hypertension. It was macroscopically revealed an increase of both lungs mass in 38% of cases with the presence of pulmonary edema signs, detected in just 56% of cases of the studied group; acute emphysema on the section in all lobes of the lungs was determined in 62% of cases. On the incision, the lung tissue in the peripheral regions, as a rule, looked pale, reddish-purple, anemic; the blood filling of the central parts of the lobes was more evident, the tissue was of a dark red-bluish color, with abundant secretion of a dark red frothy liquid. Microscopic examination of a complex of morphological equivalents of pathological processes was represented by changes in all parts of the respiratory system, including reactive rearrangements of the vascular bed, the microcirculatory part, with their accompanying abnormalities of hemodynamics and rheological properties of the blood. The bronchial lumens of large, medium and small caliber in each of the studied lung lobes in most cases (78%) were in a state of moderate and pronounced spasm; protrusion of the lamina propria of the mucous membrane of the bronchi with bundles of muscles has been determined; the epithelium in the form of short garlands and ribbons partially desquamated into the lumen; in the presence of a evident bronchospasm of large and medium caliber, including the presence of sclerosis of the bronchial wall found in 30% of cases, the epithelial layer is completely preserved, lies on the basal membrane (Fig.1).
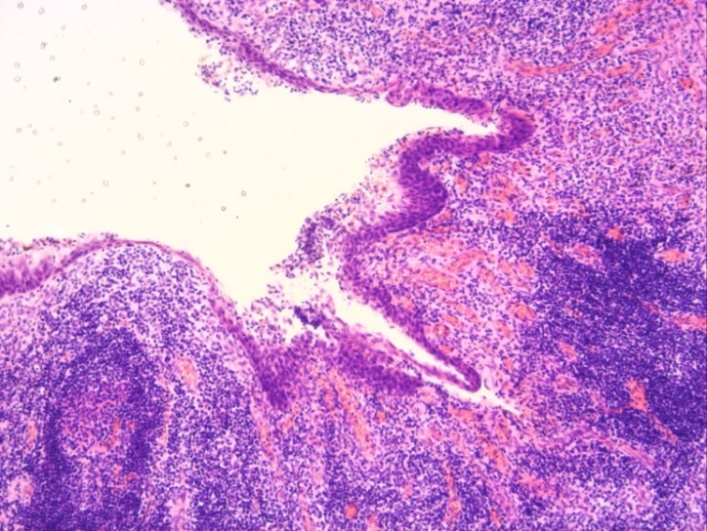 | Figure 1. Spasm of the bronchus due to vascular hyperemia, inflammatory infiltration. HE staining. x200 |
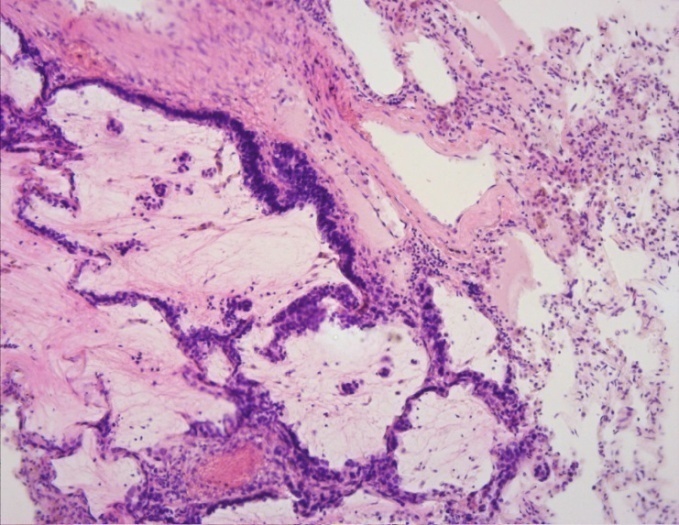 | Figure 2. Filling of the peribronchial glands with mucus. HE staining. x200 |
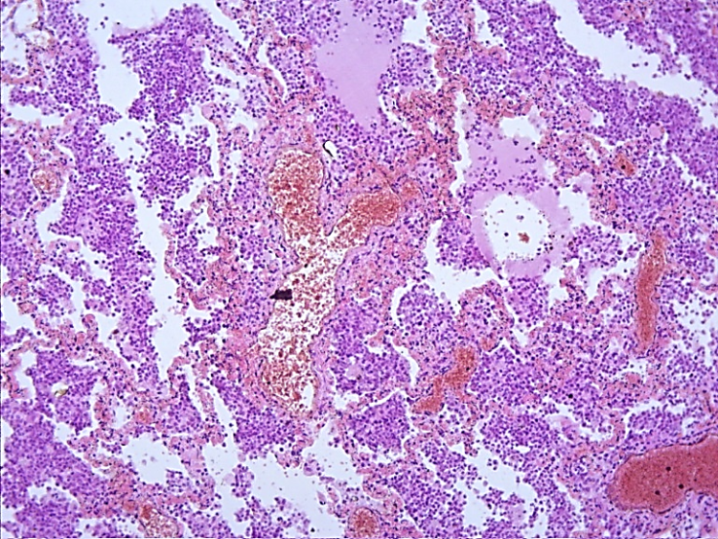 | Figure 3. Thickening of the interalveolar septa due to inflammatory infiltration. HE staining. x100 |
 | Figure 4. Hyperemia of arteries, vascular stasis of microvasculature. HE staining. x100 |
4. Conclusions
- Death cases of inpatients at various stages of experiencing a closed craniocerebral injury, in contrast to the deaths due to CCI at the scene are characterized by features of the lungs morphological changes represented by successive changes of circulatory disorders and pulmonary ventilation, inflammation.It has been macroscopically revealed an increase in the mass of both lungs in 38% of cases with signs of the lung tissue edema, in 62% of cases - due to acute emphysema, and on the incision the lung tissue looked pale, reddish-purple with abundant secretion of dark red foamy liquid.Microscopically, the complex of morphological equivalents of pathological processeswas represented by changes in all parts of the respiratory system, including reactive rearrangements of the vascular bed, the microcirculatory part, with their accompanying abnormalities of hemodynamics and rheological properties of the blood. Most of the vessels of the microvasculature were in the state of dystonia, filled with blood unevenly, the interlobular arteries are in a state of moderate and evident spasm, sharply bloodless. There are areas of swelling and homogenization in the walls of the arteries.