-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2019; 9(7): 225-228
doi:10.5923/j.ajmms.20190907.01

Effect of Plasmapheresis and Laser Radiation on Red Blood Cells in the Complex Treatment of Myasthenia
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLButaev Azamat Khasandjanovich, Rakhmonov Durbek Khusniddin-Ogli
Republican Specialized Scientific and Practical Medical Center of Surgery Named after Academician V.Vakhidov, Tashkent, Uzbekistan
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The main factor of myasthenia pathogenesis is the presence of autoantibodies to acetylcholine receptors in the blood. Myasthenia is accompanied by a significant increase the pathological forms of erythrocytes in peripheral blood. Plasmapheresis is the most effective way to remove antibodies from the blood. It has been found that plasmapheresis significantly increases the level of pathological forms of erythrocytes. Intravascular laser irradiation of blood is one of the most effective methods for preserving and restoring red blood cell forms. The authors investigated the effect of low-intensity laser radiation on erythrocytes in combination with plasmapheresis. Laser therapy in combination with efferent detoxification methods allows to eliminate antibodies from the blood, and on the other hand restores the optimal ratio among discocytes and pathological forms of erythrocytes.
Keywords: Myasthenia, Erythrocytes, Laser radiation
Cite this paper: Butaev Azamat Khasandjanovich, Rakhmonov Durbek Khusniddin-Ogli, Effect of Plasmapheresis and Laser Radiation on Red Blood Cells in the Complex Treatment of Myasthenia, American Journal of Medicine and Medical Sciences, Vol. 9 No. 7, 2019, pp. 225-228. doi: 10.5923/j.ajmms.20190907.01.
1. Introduction
- Myasthenia is an autoimmune disease due to the production of autoantibodies against acetylcholine receptors of efferent endings resulting in a defect in neuromuscular transmission. Depending on the involvement of various muscles the patient may have dysphagia or respiratory failure [8]. There are various methods of efferent detoxification such as hemosorption, plasmasorption and plasmapheresis which are effective ways of removing antibodies from the blood during myasthenia. Plasmapheresis is preferable among these methods [1]. All methods of modern medicine associated with the use of various devices with which the blood contacts are inevitably associated with mechanical and other effects on its cells. First of all, with effects on the most numerous cells that form its basis - red blood cells. Laser effects on the blood, both outside the body and with intravascular laser irradiation of blood, contribute to the reduction of pathological forms of red blood cells and an increase in the proportion of discoocytes. Low-intensity laser radiation (LILR) is used for intravascular blood irradiation in various pathological conditions including myasthenia [2]. Scanning electron microscopy is an indispensable method for assessing the effect of LILR on changing red blood cell forms [4-7]. But this method is laborious and expensive, requires special equipment.The “Rapid Thick Drop Method” (RTDM) is used to evaluate the effect of detoxification on red blood cells before and after plasmapheresis. This method was developed in the laboratory of our Center and takes only 10-15 minutes. [2].This research presents the results of studying the change in the shape of red blood cells in patients with myasthenia before and after plasmapheresis, as well as using intravascular laser irradiation of blood (ILIB) in combination with plasmapheresis.Objective: to study the effect of laser radiation and plasmapheresis on erythrocytes in the complex treatment of myasthenia.
2. Materials and Methods
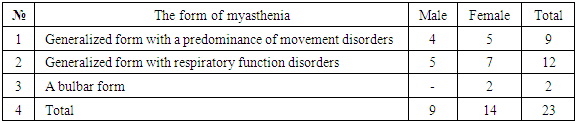
- The condition of 23 patients having received inpatient treatment was clinically examined and analyzed. There were 9 males and 14 females. Males’ age varied from 21 to 50 years, females’ age – from 20 to 55 years. In all patients the diagnosis was previously confirmed by clinical tests, including prozerin test, electromyographic data, CT / MRI investigations of the anterior mediastinum. In 21 cases a generalized form of myasthenia according to the distribution of muscle weakness was detected: with a predominance of movement disorders – 9, with respiratory function disorders – 2 cases. A bulbar form of myasthenia was detected in 2 patients. Comparison of myasthenia forms in men and women showed the following: in men a generalized form with a predominance of movement disorders (4 cases) and with respiratory function disorders (5 cases) was observed. A generalized form of myasthenia was detected in 12 women: in 7 cases – with respiratory function disorders, in 5 women – with a predominance of movement disorders, and in 2 cases – a bulbar form of myasthenia (Tab.1).
|
3. Results and Discussion
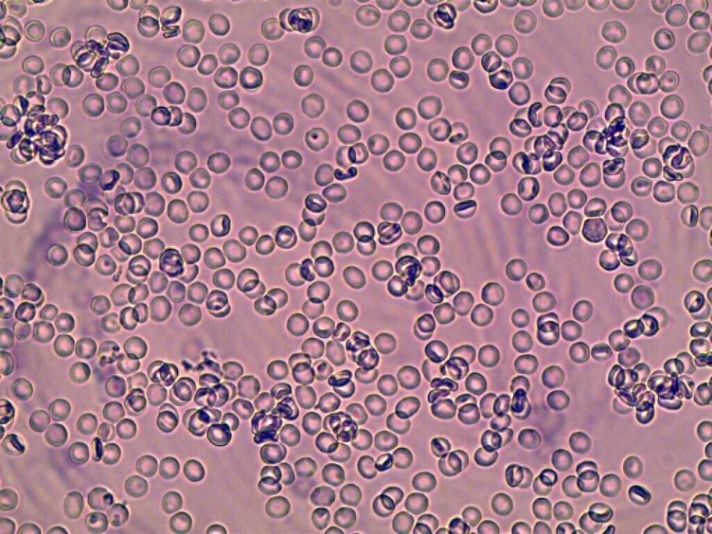
- After surgery in the early stages, 10 days after surgery, the “B” effect was observed in 5 patients: in 2 patients with bulbar form and in 3 patients with generalized form of myasthenia with a predominance of movement disorders. A satisfactory effect “C” was observed in 5 patients with a generalized form with a predominance of movement disorders and in 1 patient with a generalized form with respiratory function disorders. The effect “D” was observed in 12 patients: 1 patient with a generalized form with a predominance of movement disorders and 11 patients with a generalized form with respiratory function disorders. Patients with severe myasthenia and no effect after timectomy (n = 12) were performed membrane plasmapheresis in 3 sessions (session duration 60-90 minutes; 1000-1200 ml of plasma was removed in one session), with and without irradiation by an infrared laser. Comprehensive inpatient treatment gave a significant improvement in the form of increasing in strength in all muscle groups by 1.5-2.5 points, in 3 patients with a generalized form with dysfunction of breathing - a slight improvement, with an increase in strength of not more than 1 point.In the study of red blood cells after plasmapheresis, the following results were obtained: In normal conditions most erythrocytes are in the form of discocytes (biconcave disc) (Fig. 1).
 | Figure 1. Control. The predominance of discocytes in the peripheral blood. RTDM 10x40 |
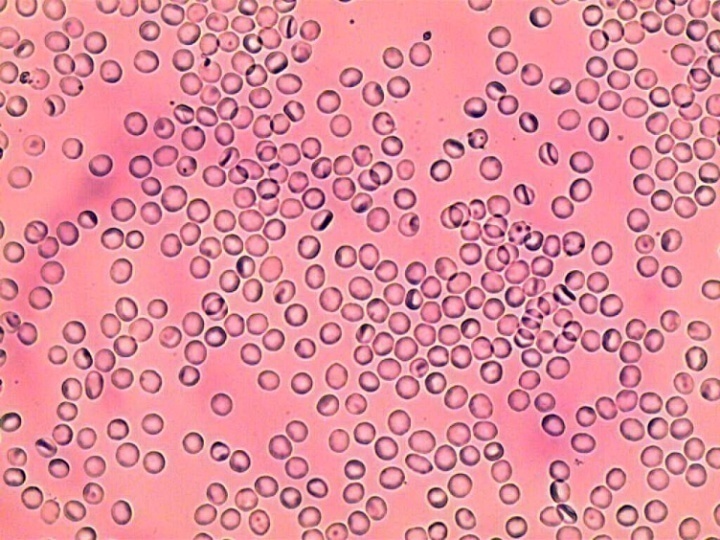
 | Figure 2. A large number of pathological forms of erythrocytes. Blood of a patient with myasthenia without treatment. RTDM 10x40 |
|
 | Figure 3. Patient's blood with myasthenia after plasmapheresis. The prevalence of pathological forms of erythrocytes is preserved. RTDM 10х40 |
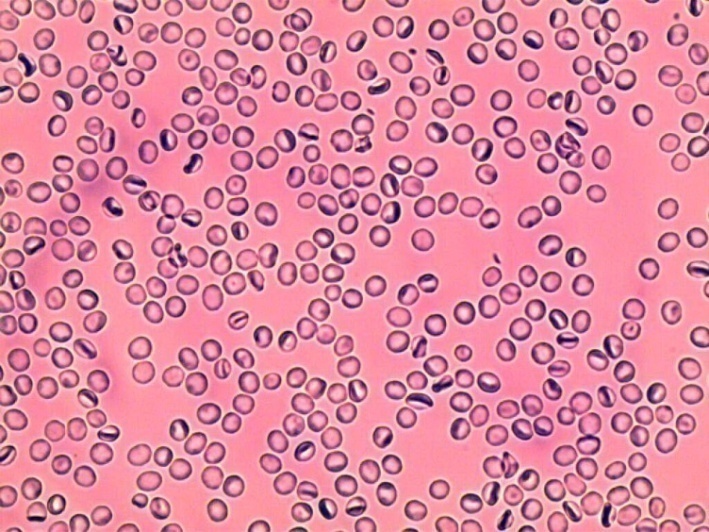
 | Figure 4. Patient's blood with myasthenia after plasmapheresis with blood irradiation by LILR. An increase in the number of discocytes is observed. RTDM 10х40 |
4. Conclusions
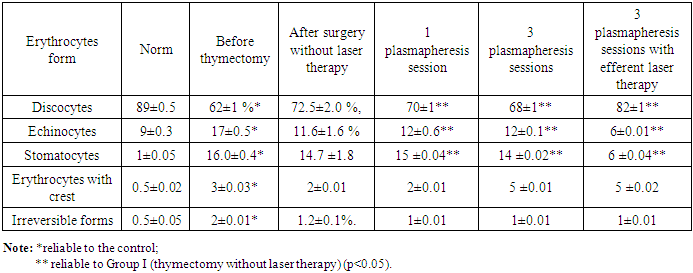
- The proportion of pathological forms of red blood cells in the peripheral blood increases at myasthenia. Plasmapheresis increases the proportion of pathological forms of red blood cells in peripheral blood. Irradiation of blood with a laser (wavelength of 0.63 microns) simultaneously with plasmapheresis significantly reduces the number of pathological forms of red blood cells.