-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2019; 9(6): 190-193
doi:10.5923/j.ajmms.20190906.03

The Incidence of Fractures in Multiple Myeloma and Their Dependence on the Severity of Osteoporosis and the Level of Total Calcium in the Blood Serum
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLOzoda Umarkulovna Achilova1, Murodulla Yuldashevich Karimov2, Khamid Yakubovich Karimov3, Abdurakhmon Abdumavlyanovich Kayumov4, Naima Kabulovna Akrarova1, Gulchekhra Zukhriddinovna Kuzieva1, Timur Raufovich Alimov3
1Hematopoietic Stem Cell Treatment Unit, Scientific Research Institute of Hematology and Blood Transfusion of the Ministry of Health of the Republic of Uzbekistan, Tashkent, Uzbekistan
2Department of Traumatology, Tashkent Medical Academy, Tashkent, Uzbekistan
3Department of Molecular Medicine and Cell Technologies, Scientific Research Institute of Hematology and Blood Transfusion of the Ministry of Health of the Republic of Uzbekistan, Tashkent, Uzbekistan
4Administration, Scientific Research Institute of Hematology and Blood Transfusion of the Ministry of Health of the Republic of Uzbekistan, Tashkent, Uzbekistan
Correspondence to: Ozoda Umarkulovna Achilova, Hematopoietic Stem Cell Treatment Unit, Scientific Research Institute of Hematology and Blood Transfusion of the Ministry of Health of the Republic of Uzbekistan, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Multiple myeloma (MM) osteolysis can affect any bone, but more often it affects those in which the content of the cortical substance is greater than the spongy. Osteoporosis, in general, is characterized by a progressive decrease in bone mass per unit volume, violation of bone microarchitecture, deterioration of the quality indicators of their tissue, resulting in increased bone fragility. Calcium level and mineral density are the indicators most quickly reacting in violation of bone metabolism. The article presents the results of using these data in predicting the occurrence of fractures in MM.
Keywords: Multiple myeloma (MM), Osteolysis, Osteoporosis, Calcium, Bone metabolism, Fractures
Cite this paper: Ozoda Umarkulovna Achilova, Murodulla Yuldashevich Karimov, Khamid Yakubovich Karimov, Abdurakhmon Abdumavlyanovich Kayumov, Naima Kabulovna Akrarova, Gulchekhra Zukhriddinovna Kuzieva, Timur Raufovich Alimov, The Incidence of Fractures in Multiple Myeloma and Their Dependence on the Severity of Osteoporosis and the Level of Total Calcium in the Blood Serum, American Journal of Medicine and Medical Sciences, Vol. 9 No. 6, 2019, pp. 190-193. doi: 10.5923/j.ajmms.20190906.03.
Article Outline
1. Introduction
- Bone tissue damage in multiple myeloma (MM) is a clinical pattern that can be observed in all patients in the advanced stage of the disease. Manifestations of changes in bone tissue in multiple myeloma are osteoporosis, osteolysis, hypercalcemia, pathological fractures, and a combination of these processes [1, 3, 5, 13, 16]. The pathophysiological mechanisms of osteolytic destruction in MM are rather multifaceted and consist not only in the secretion of osteoclast-activating factors by myeloma cells, but also in suppressing the proliferation of osteoblastic cells, which leads to the destruction of the bone matrix without subsequent replacement. Myeloma osteolysis can affect any bone, but more often the lesion occurs in those bones in which the content of the cortical substance is greater than that of the spongy [3, 5]. Osteoporosis, in turn, is characterized by a progressive decrease in bone mass per unit volume, violation of microarchitecture of bones and deterioration in the quality indicators of their tissue, resulting in increased bone fragility [6]. Unlike osteoporosis, which is characterized by a uniform decrease in mineralized osteoid, osteolytic lesion radiologically looks like a “completely empty area”, which indicates the absence of mineralization of the bone defect [1].Clinically, these forms of bone lesions practically do not differ from each other, but in the aggregate they determine the originality of the clinical picture of MM. So, in 70-90% of patients ossalgia of varying severity [1, 3, 5]. In the early stages of the disease, bone pain, non-intensive and non-permanent, is most often localized in the lumbosacral spine and in the chest. Such non-specific symptoms often provide a basis for the diagnosis of intercostal neuralgia or radiculitis [1, 2, 16].Sometimes the first symptoms of the disease are sudden sharp pains in the spine or chest that occur as a result of a pathological fracture and indicate far-gone changes in the skeleton that were asymptomatic before.The most frequently affected are: the spine, especially the lower thoracic and lumbar regions, ribs, skull, pelvis, sternum, and from the large tubular bones - the femur and humerus. Spinal fractures occur in 50% of patients with MM, in 30% of cases, fractures have a different location. Spinal cord compression develops in about 10% of cases [3-5]. Until recently, the mechanisms of bone tissue destruction were not fully studied [5, 14]. Most studies suggest that increased bone destruction is associated with tumor infiltration, correlated with tumor size [1, 11, 12, 16].According to recent studies, an intensive study of the molecular mechanisms of osteoporosis and osteolysis in MM is taking place. The accumulation of clonal malignant cells specific for this disease and their interaction with the stromal elements of the bone marrow leads to the activation and proliferation of osteoclasts, and also stimulates the production of various cytokines and growth factors, including interleukins (IL) 1β, 3, 6, 11, tumor necrosis factor- α (TNF-α), hepatocyte growth factor, as well as a heterogeneous class of lymphokines that increase bone resorption [13-15].In patients with MM, along with signs of intense bone resorption, expressed in an increase in the number and activity of osteoclasts, proliferation of functionally defective osteoblasts, their apoptotic death and, as a result, incomplete bone formation are noted [1, 5, 13]. In conditions of increased osteoclast activity and in the absence of a compensatory enhancement of recovery processes, osteoblasts are not able to compensate for the loss of bone mass.
2. Main Body
2.1. Purpose of the Study
- The purpose of the study was to study of the frequency of bone fractures in multiple myeloma and the determination of the dependence of fractures on the degree of osteoporosis and the level of Ca + in the blood.
2.2. Material and Methods of Investigation
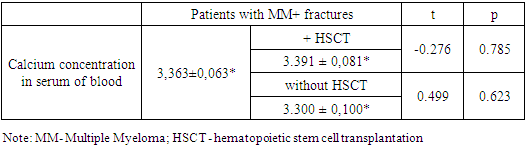
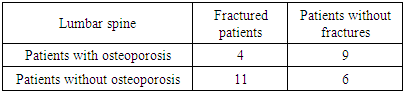
- The study was conducted in the Department of stem cell therapy at the Research Institute of Hematology and Blood Transfusion of the Republic of Uzbekistan. A total of 30 patients participated in the study. They are divided into 2 groups: group A - 15 patients with MM who had bone fractures, group B with signs of osteoporosis without bone fractures (control group). Among patients in group A2, there was a fracture of the femoral neck, 2 fracture of humerus, 4 patients of a compression fracture of the lumbar vertebrae, a 5 compression fracture of the thoracic vertebrae and 2 fracture of the ribs. At the same time, in 11 patients with multiple myeloma accompanied by fractures, autologous hematopoietic stem transplantation (HSCT) was performed (subgroup 1A) and, accordingly, in group A, a subgroup of patients who had fractures but who did not undergo HSCT could be distinguished.Diagnosis of the disease was carried out according to the standard algorithm for the diagnosis of multiple myeloma. MRI and digital X-rays were used to diagnose bone complications. To predict fractures in MM, it was decided to study bone mineral density using densitometry. The study of bone mineral density (g/cm2) of the investigated skeletal zones was carried out using an LUNAR Prodigy X-ray axial densitometer from GE (USA) with CORE v software. 8.5 by the method of dual energy X-ray densitometry.The study of BMD was performed in standard zones of the bones of the axial skeleton. Densitometric measurements were performed on the lumbar spine and proximal femurs (femoral neck). Given that the presence of osteoporosis can be the cause of pathological fractures in patients with MM, the incidence of fractures was determined depending on the presence of osteoporosis. According to the definition of the state of bone tissue according to WHO, T-score = 1 is taken as the norm. From 1 to 2 - osteopenia, 2 and above - osteoporosis.The level of total and ionized calcium in the blood was also determined. Calcium was determined on a biochemical analyzer using Human reagents.
2.3. Results and Discussion
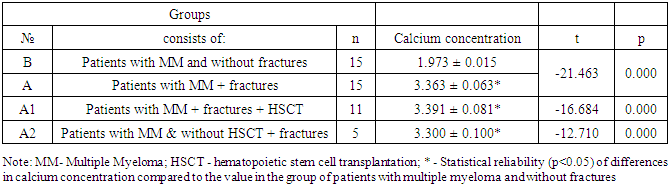
- Hypercalcemia was observed in 13 (80%) observed patients with fractures (group A) (table 1). In patients with fractures of the long tubular bones, the calcium level was high and reached 3.3 mmol/l, with fractures of the ribs and vertebrae, the calcium level was determined at the level of 3.0-3.1 mmol/l. In 2x patients who had multiple compression fractures of the thoracic vertebrae (more than 4x), the calcium level was 3.3-3.4 mmol/l. The level of ionized calcium in these patients was also higher than the norm by 0.6-1.1. Mol/l.
|
|
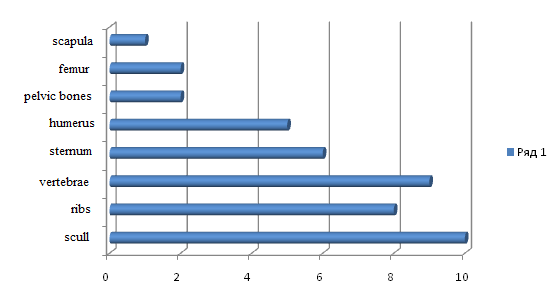 | Figure 1. The frequency of bone damage according to x-ray |
|
3. Conclusions
- Hypercalcemia is a symptom that determines the degree of bone damage in multiple myeloma: the higher level of total calcium is evidence of osteolytic lesions in the bones. Defined direct dependence of the level of calcium and frequency of fractures.Impaired bone mineral density (osteoporosis) is not associated with fractures. And it in general is an indicator of dysregulation of mineral metabolism in the bones.
ACKNOWLEDGEMENTS
- The author thanks the head of the Clinical Diagnostic Department of the Research Institute of Hematology and Blood Transfusion of the MH RUz – Nigora Asrarova for their assistance in organizing the implementation of laboratory tests.