-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2018; 8(0): 274-290
doi:10.5923/j.ajmms.20180810.04

The Auditory Working Memory of 13-15-Year-Old Adolescents Using Water with Varying Fluoride Concentrations from Selected Public Primary Schools in North Kajiado Sub County
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLBenjamin Induswe1, Gladys Opinya1, Lincoln Imbugwa Khasakhala2, Richard Owino1
1Department of Paediatric Dentistry & Orthodontics, School of Dental Sciences, University of Nairobi, Kenya
2Department of Psychiatry, School of Medicine, University of Nairobi, Kenya
Correspondence to: Gladys Opinya, Department of Paediatric Dentistry & Orthodontics, School of Dental Sciences, University of Nairobi, Kenya.
| Email: |  |
Copyright © 2018 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Water contributes significantly to the physiological functions in the in the human body. However, low fluoride doses have been reported to affect the central nervous system (CNS) without first causing the physical malformations of dental and skeletal fluorosis. Aims and objectives were to determine fluoride concentrations in water used by adolescents who were born and raised in North Kajiado and correlated it with their Auditory Working Memory Index (AWMI). The survey was cross-sectional and descriptive involving 269 school children aged 13-15 years. A purposeful sampling frame was used to select the schools. Fluoride in water was determined using the Fluoride Ion selective electrode. The AWM was assessed using the Wechsler intelligence scale for Children V (WISC-V) subtest. The mean auditory working index for the group was 111.5±22.6 while the boys had a mean AWMI of 111.46±22.37 and the girls 111.56±22.75. A comparison of the AWM of children from low (105.40±23.6) and high (99.52±23.2) fluoride schools and medium with high fluoride school had significant differences. The AWM for the children whose household water had low fluoride had higher AWMI 122.58±19.9 compared to those whose household had high fluoride in the with ANOVA F (2, 266) = 17.968, p≤.0001 and Tukey HSD for low and medium (m=-5.919, se=3.146, p=.145, low and high fluoride, (m=-18.559. se=3.124, p≤.001; medium and high (m=-12.640, se= 3.32, p≤.001 at 95% CL. In conclusion, low fluoride in the water seemed to enhance the AWM. However, the AWM declined with an increased in the fluoride concentration in water.
Keywords: Auditory working memory, Fluoride in household water, Adolescents
Cite this paper: Benjamin Induswe, Gladys Opinya, Lincoln Imbugwa Khasakhala, Richard Owino, The Auditory Working Memory of 13-15-Year-Old Adolescents Using Water with Varying Fluoride Concentrations from Selected Public Primary Schools in North Kajiado Sub County, American Journal of Medicine and Medical Sciences, Vol. 8 No. 0, 2018, pp. 274-290. doi: 10.5923/j.ajmms.20180810.04.
Article Outline
1. Introduction
- Fluoride is a chemical ion of fluorine which forms during rock formation and occurs naturally in the earth’s crust. Fluoride leaches and weathers into groundwater [1]. Water is the primary source of fluoride in the human body [2]. Other sources of fluoride include diet especially tea and fish and inhalation in places where coal mining is undertaken especially in China.In dentistry, fluoride has been used in the prevention of dental caries, and when used in low doses it has been shown that fluoride will increase the resistance to dental caries [3]. However, in higher doses of fluoride has been shown to increase dental fluorosis, skeletal fluorosis and also affect the development of the intellect [4, 5, 6]. Several studies have been done on both animals and humans to show the effect of fluoride on the memory and hence its impact on learning [7]. Reviews of studies have done on animals on the results of fluoride if any on the outcomes of neurobehavioural have concluded a moderate level of evidence adverse effects of exposures.A study on foetuses from endemic high fluoride areas had shown high levels of epinephrine and decreased norepinephrine levels which led to a reduced level of alertness. The increased level of epinephrine may be due to reduced metabolic enzymes or inhibition of the pathway that converts it to norepinephrine. It was also found that the exposed group to fluoride had significantly impaired reaction time, pursuit aiming, digit span, Benton visual retention and digit memory [8, 9]. In experimental animals at Water drinking concentrations of more than 100ppm of fluoride, studies have shown performance deficits in rats on memory tasks and learning [10]. There are no studies in Kenya hence the aim was to determine fluoride concentrations in water used by adolescents who were born and raised in North Kajiado and correlated it with their Auditory Working Memory Index (AWMI).
2. Materials and Methods
- The study was conducted in the Kajiado North Subcounty in North Kajiado in the Great rift valley which is also part of peri-urban Nairobi as a cross-sectional descriptive study.Sampling frame: The schools were first purposefully selected then divided into low, medium and high water fluoride areas. Participants in each of the schools were given the consent forms after explanation of the nature of the study to take to their parents to sign the consent form. Those who brought back the signed consent forms were given a clean labelled plastic bottle to collect the water they used domestically and a questionnaire to be filled by the parent. Those who brought back the water and filled survey form were recruited for the study.Sampling and sample size: The sample size calculation where by N=2(Z1-α/2+Z1-β) p (1-p)/ (P1-p2)2; Where N was the desired sample size. Z1-α/2 was the confidence level at 95% (SD 1.96) while, Z1-β is 1.28 β=10%, i.e. 95% clarify power. P was the mean difference between prevalence of p1 (61.8%) and p2 (38.2%); with N=2(1.96+1.28)2(0.236) (1-0.236)/ 0.618-0.382)2 = 67 per group and 74 children per group was used to cater for attrition.Participant inclusion and exclusion: The participants were 13-15-year-olds born and brought up in Kajiado county, Kajiado north subcounty and those who moved in early childhood by the age of four years old. They had to have been residents of the area for a continuous period without outward migration for a minimum period of seven years. Also, the children were excluded if they had any chronic illnesses. Fluoride Exposure assessment: By being residents of Kajiado North, Kajiado county the participants have been exposed to various degrees of fluoride that occurs naturally in Drinking Water. From previous studies with samples taken from different parts of Kajiado county indicate fluoride levels in the range of 0.1-10mg/l [11, 12]. The mean water fluoride content of Kajiado county was not available both at the county and ministry of water. Water sampling and analysis: the water samples were collected from water sources in and around the schools. The water was then taken to the government chemist for water fluoride analysis and department of mines and geology for lead, arsenic and copper analysis. Each child was given a clean, dry polyurethane bottle in which they were instructed to collect some water from the water used in the household. The water was stored in a refrigerator and taken to the government chemist the next day for fluoride analysis was none using the Orion Fluoride Ion electrode. A total of two hundred and sixty-nine water samples form the children’s household water supplies c and analysed.Instruments for data collection: Each child had their social demographic data collected by a questionnaire form. Auditory working memory: The auditory working memory was evaluated with the children in a spacious classroom where each child was placed one metre from the other. The children did a digit span and letter-number sequencing sub-test of WISC-V for AWM [13]. The oral test was done while they were seated on a chair facing the window and the teeth dried using gauze before the exam. They then proceeded to a room of almost thirty (the place selected was a quiet room) and did a digit span and letter-number sequencing test of WISC-V for Auditory Working Memory (AWM) [13]. Calibration for AWM was done by a qualified psychologist author three, and Cohen Kappa was 89% for the first author and 92% for the third author which were acceptable. The collected data was recorded on individual forms. The AWM was based on a scale by Weschler Intelligence Scale for Children, fifth edition (WISC-V) using the digit span and letter-number sequencing [13]. The digit span and letter-number sequencing were added to give the sum of scaled scores. The sum of scaled scores was then converted to an auditory working memory index which eas obtained from the WISC V manual. The working memory index was then categorised as gifted 120 and above; above-average 110-119; average 90-109; 80-89 below average; mentally challenges as 79 and below [13].Ethical clearance: The Kenyatta National Hospital/ University of Nairobi Ethics committee, National Commission of Science Technology and Innovation (NACOSTI), Kajiado county education office and Kajiado county commissioners office approved the study. The participants were informed of the nature of the research and its procedures before being given consent forms to take to their parents and or guardians for signing to participate in the study. Only those whose parents had given consent and the children assented to participate were allowed to participate in the study.Data analysis: The SPSS Version 20 was used to analyse the data. All the variables had descriptive statistics done. Statistical tests for differences were conducted using a t-test, chi-square for categorical variables and Analysis of Variance (ANOVA) and Tukey Honestly Significant post hoc tests to compare exposure within groups and means according to the distribution of each variable. A spearman’s association coefficient was used to measure the correlation between water fluoride and AWM, the degree of dental fluorosis and AWM. To assess any associations between all the assessed variables with AWM a regressional model was applied.
3. Results
- Socio-demographic characteristics: The distribution of the children by gender and age was that a total of two hundred and sixty-nine adolescents whose parents had given consent and allowed to participate were recruited to join the survey. Out of the 268 children, 178 (66.2%) were girls, and 91 (33.8%) were boys. There were more females whose caregivers gave consent as compared to boys. Above a third 184 (68.4%) were thirteen-year-olds, of whom 127 (63%) were girls, and 57 (37%) were boys. In the 14-year age group of fourteen-year-olds were 58 (21.5%) of whom thirty eighty (65.5%) were girls and twenty (34.5%) were boys. In the fifteen-year age category, they were twenty-seven (10%) of whom fourteen (51.9%) were boys, and thirteen (48.1%) were girls, Figure 1.
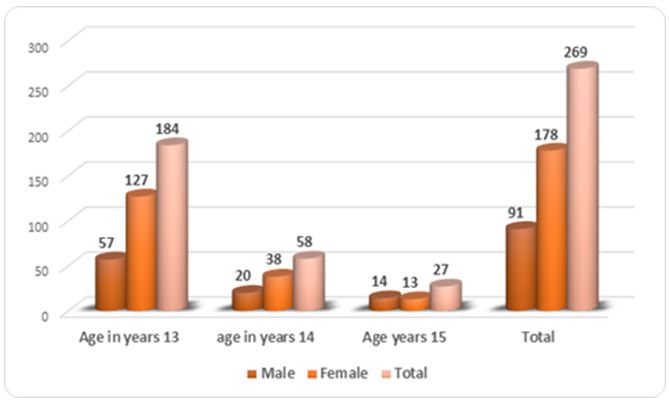 | Figure 1. The distribution of respondents by gender age |
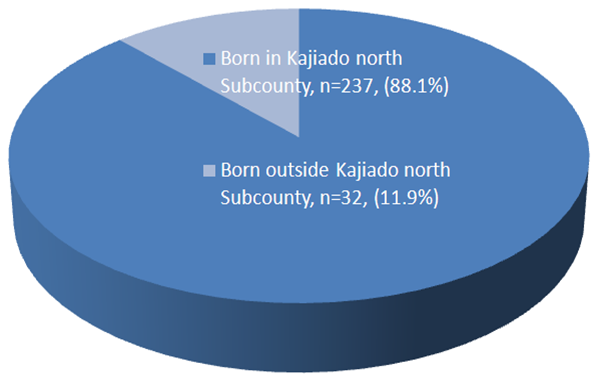 | Figure 2. Distribution of the children according to the place of birth |
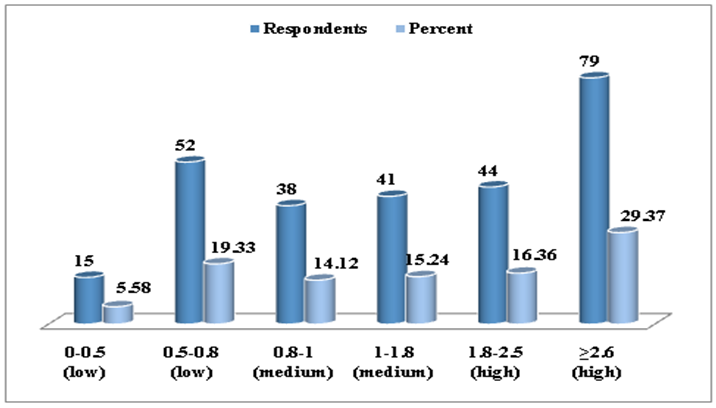 | Figure 3. The distribution of fluoride in household water |
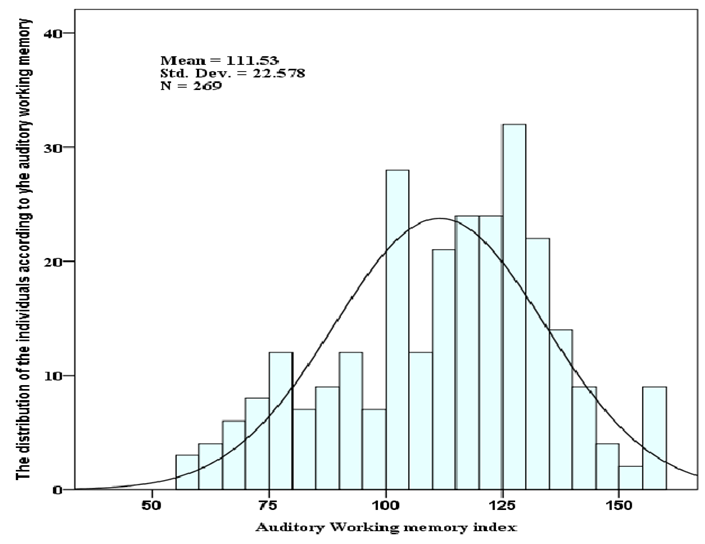 | Figure 4. The auditory working memory index |
 | Figure 5. The mean auditory working memory index and gender |
 | Figure 6. The means for auditory working memory Index by age |
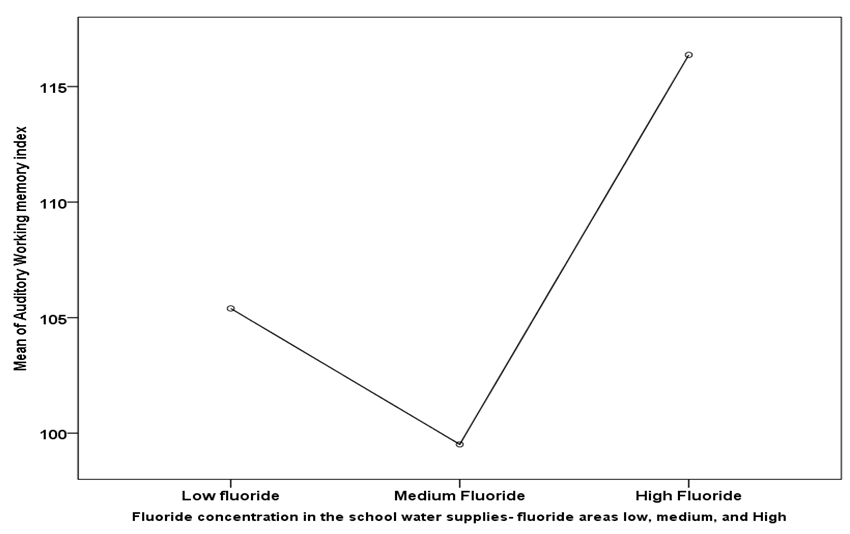 | Figure 7. Fluoride concentration in the School Water supplies-fluoride areas low, medium, and High |
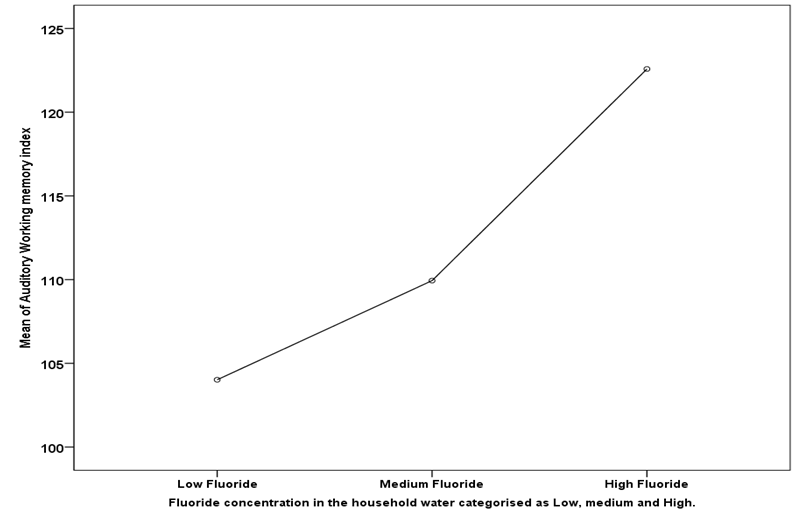 | Figure 8. Fluoride concentration in the household water categorised as Low, medium and High |
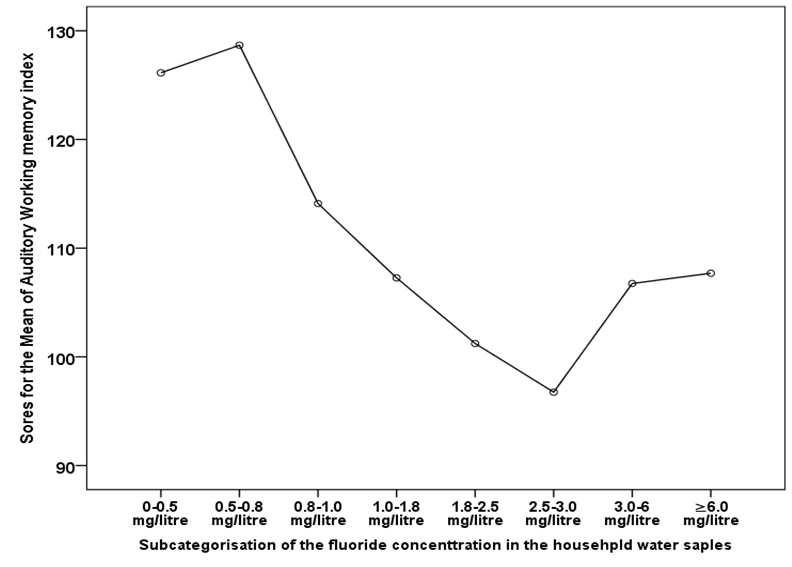 | Figure 9. The decrease in the auditory working index mean with an increase in the fluoride concentration in the household water |
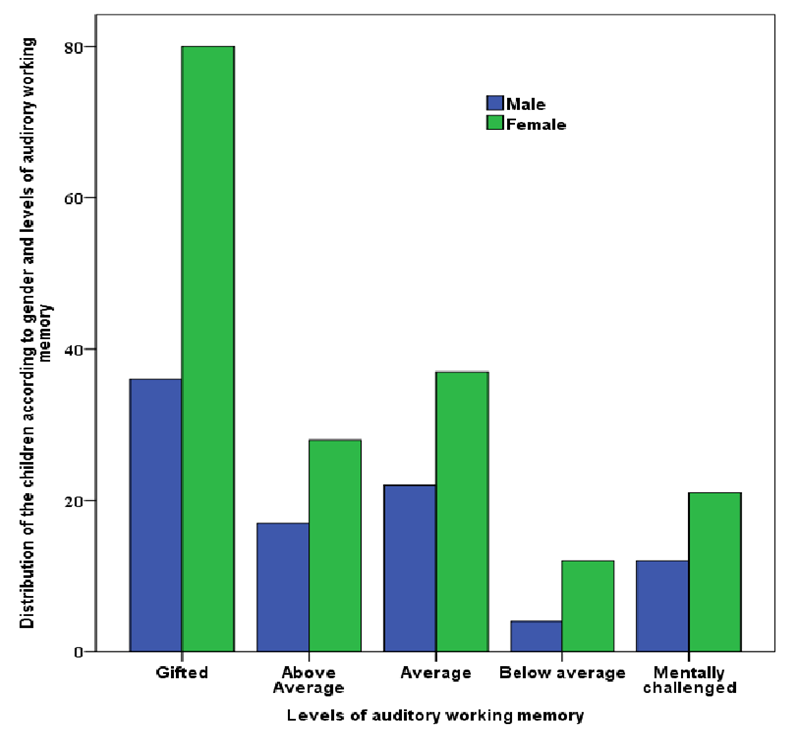 | Figure 10. The levels of auditory working memory by gender |
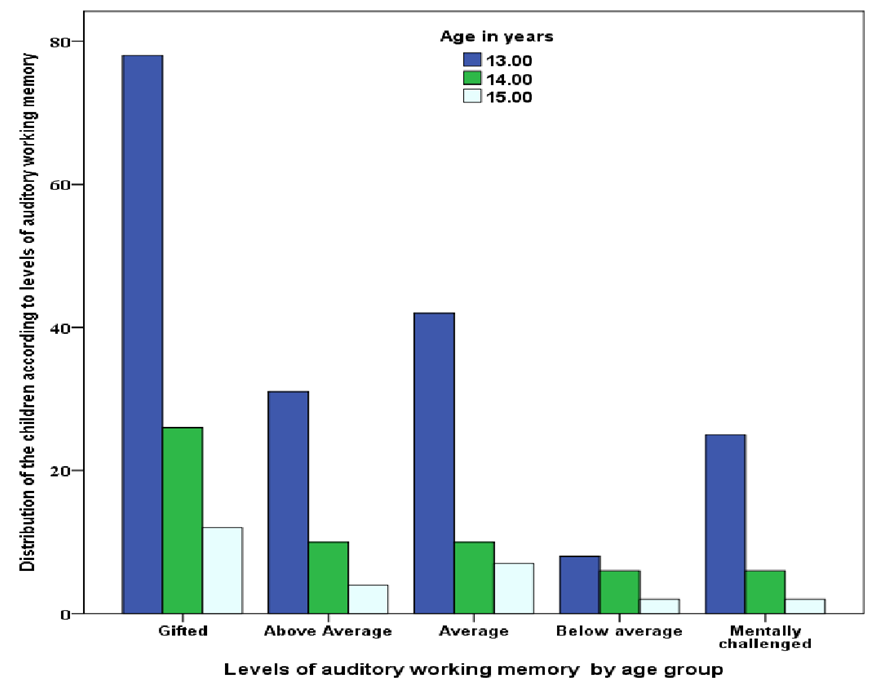 | Figure 11. The levels of working memory by age |
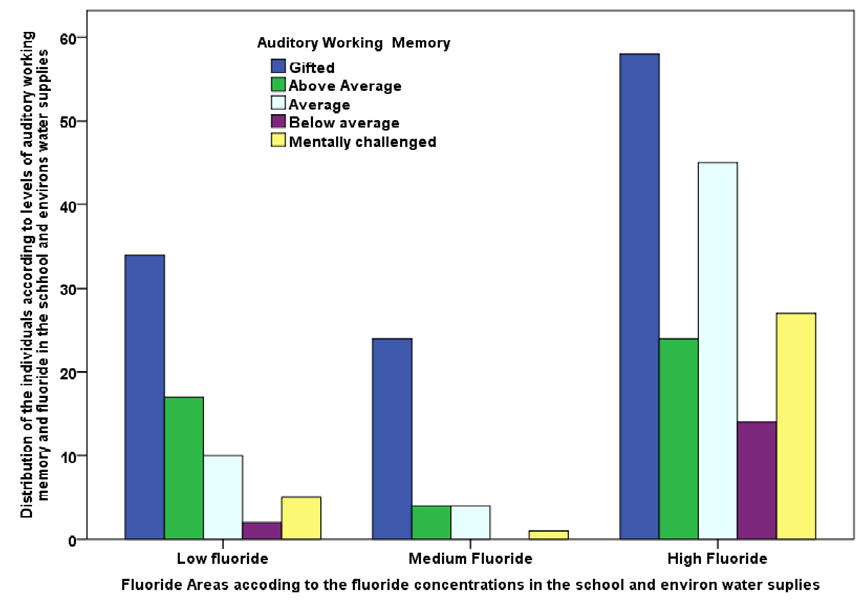 | Figure 12. Distribution of the auditory working memory of the children according to the location of the school in the fluoride area |
 | Figure 13. The Auditory working memory of the children according to household water categorisation |
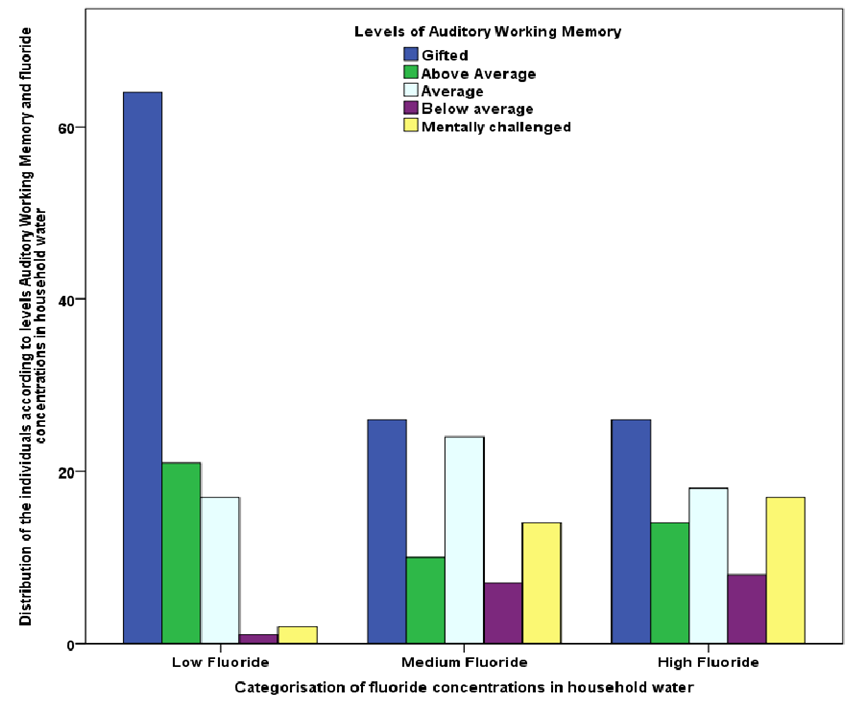
 | Figure 14. Distribution of the children based on fluoride concentrations in household water and the auditory working memory |
4. Discussion
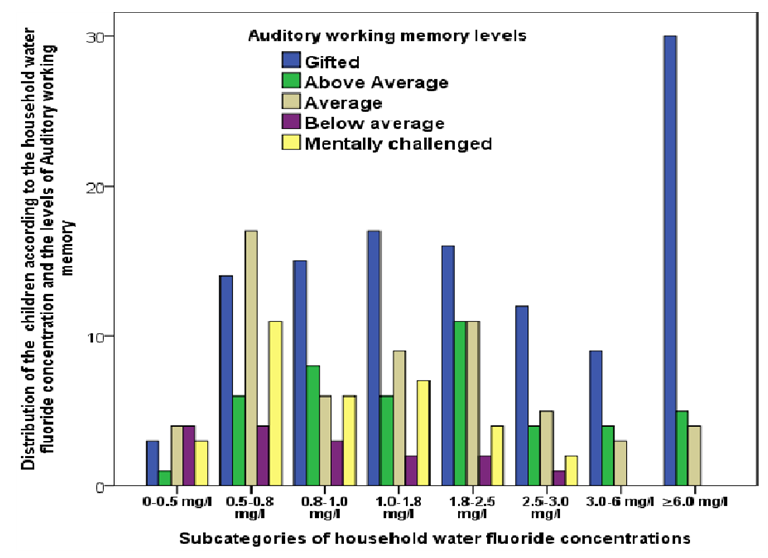
- The study population of female participants was high. This difference between the genders may be explained by the willingness of the females to participate in research than the males through the external support of supplying sanitary towel initiatives from both the Ministry of Education in Kenya and Non-Profit organisations operating in the area in the blight of a girl child. The low enrolment of the boys supports a report on the status of the boy child in Kenya by the National Gender and Equality Commission 2015 which gave a perception that 92% of the respondents believed that the boy child is lagging in the gender equality agenda [14]. This difference in higher numbers of females being recruited in a study can be associated with a higher rate of school drop out by the boys. The finding also affirms the status of the boy child in Kenya by the National Gender and Equality Commission 2015 which showed higher dropout rates for the boys than the girls at class four and five while at enrolment in schools in the lower primary; boys are equal to or even more than the girls.Fluoride is essential for the development of the child and should, therefore, be supplied in small amounts [15]. Excessive fluoride ingestion has both visible and invisible effects [15] [16]. This study investigated the difference in AWM subtest of WISC-V in children using low (≤1.0mg/l) water fluoride, medium (≥1.1≤2.0mg/l) and high (≥2.1mg/l) water fluoride living in Kajiado County which is in the former Rift Valley Province of Kenya. Water drawn from the sources of water supply to the participants detected no lead, arsenic or copper. The heavy metals in the drinking water may affect intelligence development of children.The study demonstrates that the mean AWM on WISC-V test of adolescents in high (≥2.1mg/l) water fluoride areas and high (≥2.1mg/l) household water fluoride was significantly lower than children in both low (≤1.0mg/l) water fluoride areas and low (≤1.0mg/l) household water fluoride. Considering that most of the confounders were adjusted for, the difference in AWM may be potential because of the high fluoride in the school water supplies and the high fluoride content in the household. The low AWM in children using water with high fluoride concentrations is a challenge to the Kenya government as there is inadequate quality surface water and as the peri-urban satellite towns are set up more children will be exposed to high fluoride from underground water sources. Secondly in the Kenya’s education system children are not assessed for their cognitive abilities before they are placed in a class. Such children may perform poorly in school where the teachers may fail to notice the cause of the poor performance and there is a need that children in high fluoride areas be assessed to determine their cognitive abilities.The current study found a higher proportion of children with high AWM in low household water fluoride than in high water fluoride areas. The finding in the current study is contrary to what a study in India reported higher fluoride levels resulted in higher levels of intelligence [17]. Memory is defined merely as the ability to retain information over time. Auditory memory is the ability to take orally presented information, process it, store it and be able to recall what was heard [18]. This cognitive functioning requires one to be attentive, record, process, store and retrieve the information when needed. Poor AWM results when children can’t record, process, store or retrieve the information that was exposed to, this has negative consequences on learning. Children with low AWL find it challenging to pay attention and follow instructions. AWM plays a critical role in literacy as it has a direct impact on reading and writing, spelling and mathematics skills. According to Cyndi Ringoean, a neuro-developmentalist, a child with poor AWM cannot learn using the phonics method [19]. When even doing self-reading, listening and processing the information when the child needs to do silent reading a good AWM to recall what was read. Addie Cusimano also opines that AWM is overlooked as a learning skill deficiency and he found severe deficiencies in children with hyperactivity and or attention deficit disorders [19]. Working memory is strongly correlated to intelligence in adults and children hence those performing better on working memory tasks have also shown a tendency to be better on the intelligence task [20] [21]. Several animal studies have tried to explain the possible mechanisms of neurotoxicity of fluoride [22] [23]. Fluoride when ingested through the child’s diet or crosses the placenta, its retained in the body about 80-90% in children and 60% in adults [15] [24]. Its absorbed into the bloodstream and forms complexes which are lipid soluble and can cross the blood-brain- barrier hence accumulating in the cerebral tissues [16]. This complexes then affect the development of the CNS by different mechanisms, e.g. inhibition of glutamate transporters, free radical generation and inhibition of mitochondrial energy and antioxidant enzymes [25]. This alteration in the structure and function in the CNS especially during the 1st eight years of life and also during foetal growth may lead to cognitive dysfunction, intellectual deficits and learning difficulties [22] [25]. Fluoride has also been shown to interfere with thyroid gland activity leading to an adverse effect on the development of the brain and function in children [26].Cognitive development is determined by genetic and environmental factors [27]. The regression analysis in this study showed that high fluoride content level in household water supply significantly affected AWM. That other factors like age, gender, child’s and parents’ level of education and income did not. The result is in agreement with the study by Seraj B and Xiang Q [6] [28]. The low AWM for the children using high fluoride in an agreement with a study where a systematic review and a meta-analysis that showed reported in the literature that children who used water with high fluoride had consistently low IQ which was an indication of fluoride neurotoxicity effects [29]. A recent study in Una, Himachal, Pradesh India where the fluoride in the water supplies was more than 0.5ppm and reported insignificant association between the low intelligence level with the high fluoride in the water. The challenge we observed in our current study was that there were children from the low fluoride area who attended schools supplied with high fluoride. A finding which we did not document in the current study is that 86% of the children carried water to school and this masked the relationship with water. However, when each child was correlated with the fluoride in the water which they regularly carry to school there were strong associations between the household water and the children’s AWM. At 0.5mg/liter there was a strong association between the children’s AWM and the subcategories of fluoride concentration as we found that the children had varied sources of for water and the fluoride concentration in the household water varied according to the source [30]. The study population recruited respondents from the semi-urban homogeneous community in Kajiado who attended public schools reducing the effect of environmental factors [6]. However, complete elimination of both environmental and genetic factors is near impossible [6]. The water fluoride content in both area and the household were used as an indicator of the child’s fluoride exposure. The study may support the hypothesis that excess fluoride in drinking water is neurotoxic. Therefore, there is a need for constant and close monitoring and regulation of fluoride levels in water supplied to the population especially in endemic fluorosis areas and also the implementation of public health policy to reduce the exposure to high fluoride in water.
Study Limitations
- It was a cross-sectional descriptive study, this may have flaws, and it was difficult to control the children using low fluoride in household water from attending a school in a high fluoride area. Similarly, those from the high fluoride household water may have participated at the low fluoride school. The study did not recruit the adolescents who had dropped out to assess the AWM; previous studies have shown that poor academic achievement is correlated with high school dropout and low school enrolment.
ACKNOWLEDGEMENTS
- The chairman, the dean of the department of paediatric dentistry, School of Dental Sciences, College of Health Sciences, the University of Nairobi for facilitating. The faculty and peers in the department of paediatric dentistry, School of Dental Sciences, for constructive criticism which improved the study. The children and the parents agreed to participate in the study. The headmistress and the teachers who allowed us to run the study in their schools and for organising the children. The relevant bodies which read and approved the research proposal at the university, county and National level.