-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2018; 8(0): 267-273
doi:10.5923/j.ajmms.20180810.03

Comprehensive X-Ray-Radioisotope-Ultrasound Diagnostics and Improved Treatment of Diabetic Foot Syndrome
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKurbanov Erkin Yusufovich1, Babadjanov Ahmadjon Sultanbaevich2, Jalolov Sulton Irnazarovich1, Aslamov Jasur Kahramonovich2
1Department of Purulent Surgery, Central Hospital, Samarkand, Uzbekistan
2Department of Surgery, State Medical Institute, Samarkand, Uzbekistan
Correspondence to: Kurbanov Erkin Yusufovich, Department of Purulent Surgery, Central Hospital, Samarkand, Uzbekistan.
| Email: |  |
Copyright © 2018 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

To date, the issues such as development of differentiated treatment tactics of diabetic foot syndrome based on diagnostic data of the state of vascular, microcirculatory changes and improvement of surgical approach to treatment remain topical. The main objective of the study is to improve surgical treatment of DFS basing on calcification of the middle coat of arteries (Monckeberg's arteriosclerosis) and micro-circulatory disorders of lower limbs. Material and methods: In the Department of Purulent Surgery of Samarkand Central Hospital 120 in-patients were surveyed. The patients were divided into three groups: the first group consisted of 79 patients with diabetic foot syndrome and diabetic gangrene of lower limbs, who had received x-ray-radioisotope-ultrasonography and advanced surgical treatment; the second group included 29 patients without diabetes who had received x-ray-radioisotope examination; the third group consisted of 12 patients who had been done multi-slice spiralcomputed tomography of the lower limbs arteries. Results: Ultrasound, radioisotope and x-ray examinations complement each other, allow to predict of the clinical course of pathological process and to select the right treatment tactics. Conclusions: When choosing the treatment tactics of patients with diabetic foot syndrome it is useful to take into consideration the state of the main arterial blood flow, the presence of Monckeberg's arteriosclerosis, and the degree of microcirculatory disorders.
Keywords: Diabetic foot, Microcirculation, Pertechnetate, Arteriolosclerosis, Calcification
Cite this paper: Kurbanov Erkin Yusufovich, Babadjanov Ahmadjon Sultanbaevich, Jalolov Sulton Irnazarovich, Aslamov Jasur Kahramonovich, Comprehensive X-Ray-Radioisotope-Ultrasound Diagnostics and Improved Treatment of Diabetic Foot Syndrome, American Journal of Medicine and Medical Sciences, Vol. 8 No. 0, 2018, pp. 267-273. doi: 10.5923/j.ajmms.20180810.03.
Article Outline
1. Introduction
- According to the World Health Organization data, the number of people suffering from diabetes in the world increased from 108 million in 1980 to 422 million in 2014. It is estimated that in 2012, 1.5 million cases of death were directly caused by diabetes, while another 2.2 million deaths resulted from high blood glucose [1]. According to WHO estimates, in 2030 diabetes will be the seventh most common cause of death [2]. Despite some progress in treatment, diabetes is still recognized as one of the most important non-communicable diseases, the prevalence rate of which has reached pandemic proportions (Suncor Yu.I. [3], Dedov I.I. [4], Tarasenko N.A. [5]). The incidence of disease is growing in an exponential manner. According to the International Diabetes Federation data, the number of people with diabetes projected to grow to 642 million by 2040 [6].Overall outcome of uncontrolled diabetes is hyperglycemia, or high blood sugar, which eventually leads to severe damage to many systems of human organism, especially the nerves and blood vessels [1]. The urgency of the problem is the severity of surgical complications of diabetes such as diabetic foot syndrome (DFS) and diabetic gangrene of the lower limb (DGLL). The amputations of lower limbs are performed 17-45 times more frequent in patients with diabetes than in people not suffering from this disease [7]. Angiopathy is sometimes based on calcification of the middle coat of arteries and arterioles (Monckeberg's arteriosclerosis, medial calcinosis). According to I.I.Dedov, sclerosis of tibial arteries is determined in more than 10-15% of cases [8]. The risk of medial calcinosis of the arteries on the background of its thickening and sclerosis increases with age from 5% among young people to 37% in the elderly. Arterial calcification (AC) in patients with diabetes is detected, on average, 3 times more frequent than in persons without disorders of carbohydrate metabolism. Hallmarks of medial calcinosis are evident not only on x-ray images, but also on duplex scanning of vessels of lower limbs [9, 10]. AC of tibia often develops in cases of long-lasting diabetes, especially combined with poor metabolic control and peripheral polyneuropathy [11]. Development of AC is primarily related to the formation of polyneuropathy and damage to the autonomous area of peripheral nervous system. In the state of autosimpatektomy disorder of the myocyte trophic structure of vascular wall accompanied by calcium deposits. As a result, the artery becomes stiff tube with a fixed diameter, which creates preconditions for the development of "functional" ischemia of extremities, i.e. ischemia arising amid conditions requiring the increase of volumetric blood flow and primarily during physical activity, as well as amid other conditions (inflammation) [11, 12]. In addition, a number of studies have noted the existence of the so-called rigidity or increasing density of the arterial walls of the lower extremities, resulting in restrictions to volumetric blood flow and formation of ischemia of the extremities even when ankle-brachial index (ABI) is more than 0.9 [13]. Despite AC in the treatment of diabetes, there is still gap in knowledge about it at different stages of development of DFS. The analysis of literature sources indicates that AC, common in patients with DFS had not been subject to adequate consideration while choosing the tactics of surgical treatment. Research data of the microcirculatory bed are somewhat ambiguous. Numerous morphological studies have identified changes in basal membranes and other components of the vascular wall in patients with diabetes. Great attention has been paid to a possible pathogenetic role of morphological changes of microcirculatory bed in the development of diabetic complications, particularly destructive involvement of feet. However, despite the apparent obviousness of such a link and numerous data on the correlation of morphological changes and impairment of capillaries, the value of microangiopathy as an independent factor in the development of tissue necrosis of foot has not been proven [14]. Thus, the current diagnostic methods need to be refilled with new data on microcirculatory changes in patients with DFS. Therefore, the main objective of the study is the improvement of surgical treatment of DFS based on calcification of the middle coat of arteries (Monckeberg's arteriosclerosis) and microcirculatory disorders of lower limbs.
2. Material and Methods
- In the Department of Purulent Surgery of Samarkand Central Hospital 120 in-patients were surveyed. The patients were divided into three groups: the first group consists of 79 patients with DFS and DGLL, who received x-ray-radioisotope- ultrasonography and advanced surgical treatment; the second group includes 29 patients without diabetes who received x-ray-radioisotope research; the third group consists of 12 patients who were done multi-slice spiral computed tomography of the lower limbs arteries. The status of microcirculation was defined using radioisotope method of research using technetium 99mTc proposed by us. Preparation with activity of 70-90 MBC and the volume of 0.3-0.5 ml saline solution was injected subcutaneously in the spaces between toes symmetrically on both sides. The degree of microcirculatory changes was determined by the speed of resorption of radiopharmaceuticals using a gamma camera equipped with electronic-computing device. All the patients were conducted dynamic fixing of technetium resorption within 30 minutes, as well as I was defined resorption time of 50% technetium (T1/2, or half resorption). Foot x-ray was done using the apparatus of "RUM-20M" (traditional radiography) and ECONET EVA-HF 525 (digital radiography), and using standard technique of PA and lateral projections. In this, not only osseous abnormalities were determined, but also the stages of AC of the arteries was identified. The following 5 stages of AC were distinguished based on radiographic changes: Ÿ 1st stage – vascular wall thickening caused by beginning of calcium salts incrustation, linear shadows of small intensity; Ÿ 2nd stage – ring shadow in the first metatarsal span (display on the radiograph of the foot in PA projection of cross-section of deep plantar artery); Ÿ 3rd stage – partial calcification of the vessel walls; Ÿ 4th stage – calcification of the vessel walls in the form of "stream of smoke"; Ÿ 5th stage – marked wall calcification of the vessel walls in the form of "curved cord" with lesion of its small branches. Ultrasound detection of pulsation of the femoral, popliteal, posterior tibial artery and dorsal artery of the foot using the device "Minidop" served as a clinical evaluation methods of macroangiopathies. In addition, ultrasound doplerography with measuring segmental blood pressure of limbs and determining the value of the ABI was also performed using the device "Minidop". Duplex scanning was performed using the apparatus "PHILIPS". The treatment was carried out taking into account the severity of clinical manifestations of DFS. Organ-preserving operations on the foot, in particular, amputation of fingers, were carried out with high excision of flexor and extensor tendons of the foot, sparing minimal excision of muscles, resection of metatarsal bone heads using improved methodology (resection of not less than ½ of the first and fifth metatarsal bones in the slanting direction; isolated resection of more than 2/3 of second, third, and fourth metatarsal bones in the transverse direction; when the amputation of several fingers – combined step-by-step resection of several metatarsal bones in the slanting direction). We abdicated exarticulation of Lisfranc's and Shopper’s joint, holding instead of them transmetatarsal resection of the foot by Sharp. In case of development of DGLL "big" ("high") amputations (legs and thighs) were done. Tibia level amputation was performed in the upper third part with extirpation of soleus muscle. Statistical processing was conducted on the personal computer Pentium 4, using Microsoft Word 2010 software system, in particular Excel, based on parametric criteria such as Student’s t-test.
3. Results and Discussion
3.1. Study of the First Group
3.1.1. History
- The study of the history of the first group of patients has shown that hospital admissions in 30 or more days after the onset of purulent-necrotic changes were observed at 30 patients (37.97%). Hospital admissions of patients during the first week after the onset of the disease made up 25.32%, which was not sufficient in relation to those who suffered from diabetes. Among all patients of this group period from the moment of occurrence of symptoms of DFS to hospitalization averaged 24.33 ± 2.63 days. In four cases (5.06%) of the main group diabetes was identified for the first time though patients had noted the presence of subjective symptoms. 40 patients (50.63%) irregularly consulted an endocrinologist, did not follow diet, the control of the level of glycaemia was not conducted by them in a timely manner. Mostly there were rural population. Duration of diabetes before hospital admission averaged 9.62 ± 0.62 years. 52 patients suffered from diabetes for 5-15 years, which account for 65.82%. Diabetic history of 44 patients (55.7%) made up 10 years or more.
3.1.2. Ultrasonography
- Arteria femoralis pulse off all patients in the first group was good; patients usually had arteria popliteal pulse (70 cases – 88.6%; in other cases weakened pulse); arteria dorsalis pedis pulse and arteria tibialis posterior pulse varied depending on the degree of vascular lesions of the foot. Ultrasound examination of patients showed that the value of ABI of 36 patients (46%) on admission to hospital accounted for 1.16±0.01, on average, that was related to the presence of AC. ABI of another 22 (28%) patients was equal to 0.69±0.02. 8 patients (6%) had critical ischemia, their ABI accounted for 0.5±0.02. The other 15 patients (19%) had no pulsation simultaneously in the two arteries of foot.
3.1.3. Radioisotope Examination
- Radioisotope examination of all 79 patients in the first group was conducted. Comparative analysis of the treatment results with the radioisotope examination of patients helped distinguish two subgroups of patients with completely different quantitative and graphical indicators: 1) The first subgroup consisted of patients with diabetic angio-neuropathy and developed DFS, who were conducted conservative treatment and organ-preserving operations on the foot. Pathological process proceeded relatively favourably and ended without major amputations (72 patients – 91.14%). 2) The second subgroup included patients with DGLL, they were conducted large amputation (7 patients – 9.6%).Resorption of technetium of patients with the first subgroup (no DGLL) was relatively slow and gradually. Resorption time of 50% technetium averaged 15.4 ± 0.44 minutes (T1/2 = 11-30 min). A graphical image of resorption of the preparation was crescent-shaped, or had gradually decreasing form (Figure 1, line 2).Study of microcirculation in the second subgroup of patients with DGLL, showed that the resorption of technetium of this category of patients proved to be extremely slow. During the observation in no case was observed resorption of 50% technetium (T1/2 > 30 min – P < 0.0001). Therefore, graphic image of curve was nearly horizontal. This type of graph got the name "horizon necrosis" (Figure 1, line 3). Treatment in this group of patients ended with big amputation (legs and thighs), that was associated with the phrase "over the horizon – amputation".
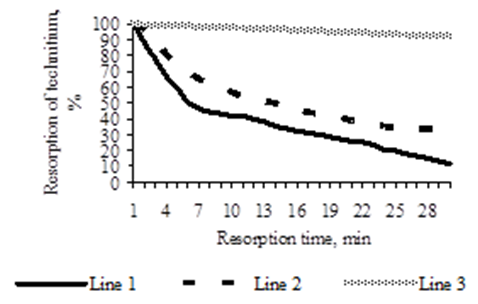 | Figure 1. Dynamics of technetium resorption in patients with diabetes and without diabetes |
3.1.4. X-ray Examination
- The results of X-ray examinations of 79 patients were analysed. AC occurred in more than half of the cases – 49 patients (62.03%). It was found that 4 clinically important subgroups of patients are clearly distinguished (Figure 2):
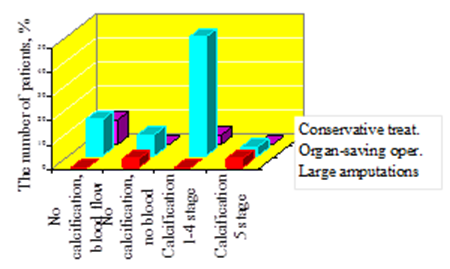 | Figure 2. Comparison of x-ray examination and treatment |
 | Figure 3. Calcification of the arteries of 3 stages, gangrene 4 fingers |
 | Figure 4. Total calcification of arteries 5 stage |
3.1.5. Results of Treatment of Patients in the First Group
- 66 operations out of all the operations in the first group were done on the foot, which accounted for 91.67%; 7 of them were large amputations, which amounted to 9.6%. 2 out of large amputations were performed on level of the tibia, which amounted to 2.78% and 5 of them were thigh amputations – 6.82%. One of the main reasons of large amputations were:- delays in hospital admissions of patients;- poor control of glycaemia and unawareness of foot care (the burn with hot bath or heating device, incorrect nail cutting) despite the fact that they were aware of their disease.The average length of stay of a patient in bed was 17.15 ± 1.46 days. Analysis of patients with foot operations showed that 34 operations out of them (47.22%) were necrectomy; the other 28 operations (38.89%) were amputations of one or more fingers; 1 of them (1.39%) was resection of metatarsophalangeal joint; the other 3 (4.17%) were transmetatarsal resection of the foot by Sharp. One patient died (1.27%), it was related to late hospital admission, the severity of the condition while hospitalization, and accompanying diseases.The objective of our analysis of the treatment of patients in the first group was the identification of repetition of surgical treatment and study of its causes. Operations were repeated only in 5 cases that accounted for 6.33% of patients in the primary group, and 6.94% (5 reoperations) of all conducted operations. Causes of these repetitive operations were underestimation of changes in the vascular bed and refusal of the patient from the proposed large amputation. Effectiveness of surgical treatment of patients in the first group showed the correctness of the proposed methods of improvement of traditional surgical treatment. Thus, ultrasound, radiologic and x-ray examinations complement each other, allow to predict the course of pathological process and to select the right treatment tactics. In addition, the radiologic examination showed that there were microcirculatory disorders in all of the surveyed cases of DFS and DGLL; it means they could cause both angiopathy and neuropathy.
3.2. Results of a Survey of Patients in the Second Group (without Diabetes)
- 15 of the 29 patients were patients with pyo-inflammatory diseases of the lower extremities without diabetes and without vascular pathologies of the lower limbs. This subgroup was considered in order to determine the status of microcirculation in lower limbs in relatively healthy persons (subgroup №1). The age of these patients ranged from 35 to 65 years. In the first subgroup were patients with infected wounds, ulcerous, phlegmonous-abscessing, osteomyelitis changes of the lower limbs. Patients’ conditions throughout the treatment period was satisfactory. All of these patients were conducted radiologic examination using radiologic study technetium 99mТс, as in the first group. It was found that technetium resorption of tissue depot of relatively healthy persons was fast, resorption time of 50% technetium averaged 5.8 ± 0.29 minutes (T1/2 < 10 minutes). The graphical image of preparation resorption, generally, had the form of a hockey stick (Figure 1, line 1). Resorption time of 50% technetium significantly (P < 0.0001) differed from the performance of the patients with DFS and DGLL. Thus, the comparison of the research results of healthy patients with the results from the first group of patients showed that the method of radioisotope detection of microcirculation by the degree of resorption of 50% technetium from tissue depot allows to obtain reliable quantitative information on the status of microcirculation. This information can be used while choosing the treatment tactics of patients with DFS.The remaining 14 patients of the second group were patients without diabetes, but with other vascular pathology (12 patients with obliterating atherosclerosis and 2 patients with obliterating endarteritis of lower limbs) to determine whether they had AC (subgroup №2). The age of patients ranged from 39 to 82 years. All of these 14 patients received x-ray foot in PA and lateral projections. In no case of the second group, AC was not detected. Thus, the comparison of the results of radiographic examination of patients with vascular pathology of the arteries of the lower limbs, but without diabetes in the second group with the results from the first group of patients showed that radiographic method of detection of AC is reliable. Foot x-ray data may also be used to choose the treatment tactics of patients with DFS.
3.3. Results of Examination and Treatment of Patients of the Third Group
- The third group consisted of 12 patients with DFS, who received MCT of arteries of the lower limbs. Since arteriography makes difference for diabetic patients in terms of adverse impact of contrast due to the diabetic nephropathy, this group of patients consists of patients, who did tomography of the arteries due to the arterial occlusion of lower extremities arteries. The age of patients ranged from 49 to 79 years, on average 63 ± 2.77. In this group were patients with infected wounds, ulcerous, phlegmonous-abscessing, gangrenous changes in the lower limbs.The time period from the moment of the first symptoms of DFS to hospitalization of patients in third group accounted for 21.4 ± 7.78 days, on average. Duration of diabetes before the hospitalization accounted for 14.17 ± 2.3 years. Ultrasound examination showed the following: arteria femoralis pulse was good in two cases (16.67%), in the remaining cases it was weakened; two cases had no arteria popliteal pulse (16.67%), and in 9 cases it was weakened (75%); 9 cases (75%) did not have arteria dorsalis pedis and arteria tibialis posterior pulses, 3 cases (25%) was weakened. All the patients of the third group were done MCT and were identified the main arteries occlusion of lower extremities due to atherosclerotic changes. The degree of occlusion of patients varied; mainly it was the popliteal and tibial artery. MCT of arteries showed that this survey provides a good overview of the changes occurring in the lumen of the vessel (Figure 5).
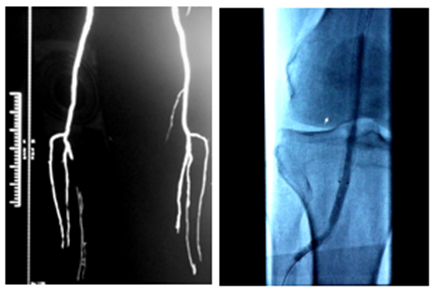 | Figure 5. Multislice computed tomography of the arteries. Occlusion of the right posterior tibial artery, uneven contraction of the right fiont tibial and both small tibial arteries. Stage of balloon angioplasty and stenting |
4. Conclusions
- When choosing the treatment tactics of patients with DFS it is useful to take into account the following:Ÿ Data of the main blood flow of the foot arteries (lack or presence of at least one of the two arteries – arteria dorsalis pedis, arteria tibialis posterior) obtained by duplex scanning (dopplerography).Ÿ Foot x-ray data based on the stage of the calcification of the main arteries of foot – arteria dorsalis pedis, arteria tibialis posterior with their branches – arteriae plantares, a. metatarsea dorsalis prima, ramus plantaris profundus, arteriae digitales. In case of AC at 1-4 stage, organ-preserving operations on the foot should be carried out. In case of radiographic detection of the total AC at 5th stage and the presence of arterial blood flow, the limb function should be maintained by performing a transmetatarsal resection of the foot by Sharp. Identification of total AC with lack of arterial blood flow, however, might lead to the large amputation at the level of thigh and lower leg. According to the data of arteries ultrasonography based on the main blood flow of the foot and radiography, taking into account the stage of AC, it is possible to predict the further course of the disease such as DFS and DGLL. However, the absence of AC does not exclude the severe course of DFS, resulting in a large amputation. Ÿ The study of radioisotope examination (if the resorption of 50% technetium is less than 30 minutes) showed that in the practical application radioisotope examination was the most effective in cases of the absence of AC and the main arterial blood flow of the foot arteries. Ÿ According to the results of MCT of arteries, in case of detection of the occlusion of lower extremity arteries based on duplex scanning, the treatment should be directed to the preservation of limb functions using a balloon angioplasty, stenting of arteries of the lower extremity, and only further organ-preserving operations on the foot should be carried out.