-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2018; 8(8): 213-218
doi:10.5923/j.ajmms.20180808.08

Chest Compression-only Cardiopulmonary Resuscitation in Nigerian University Students
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAdedamola Olutoyin Onyeaso1, Chukwudi Ochi Onyeaso2
1Department of Human Kinetics and Health Education, Faculty of Education, University of Port Harcourt, Port Harcourt, Nigeria
2Department of Child Dental Health, Faculty of Dentistry College of Health Sciences, University of Port Harcourt / University of Port Harcourt Teaching Hospital, Port Harcourt, Nigeria
Correspondence to: Adedamola Olutoyin Onyeaso, Department of Human Kinetics and Health Education, Faculty of Education, University of Port Harcourt, Port Harcourt, Nigeria.
| Email: |  |
Copyright © 2018 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

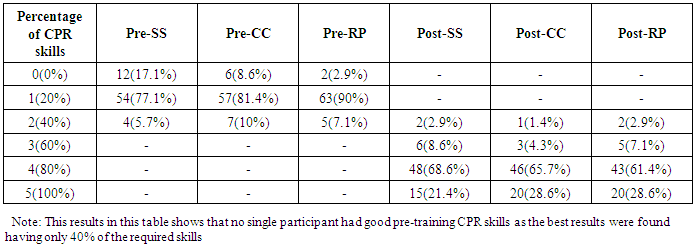
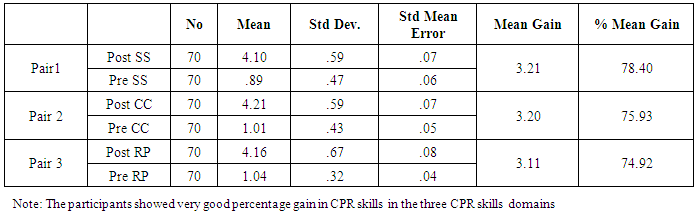
Introduction: Chest compression -only (Hands-only) CPR is believed to be as effective as the conventional CPR in providing bystander CPR for victims of out-of-hospital cardiac arrest (OHCA). Hitherto, there is no report on hands-only CPR from Nigeria. This study aimed at assessing the CPR skills of some students in a Nigerian University after training them on hands-only CPR method. Materials and Method: Using a quasi-experimental cohort study design, seventy (70) students in a Nigerian University were involved in the study in March 2018. The pre-training stage involved asking them to resuscitate a simulated victim of OHCA using manikins without mouth-to-mouth ventilation. An American Heart Association (AHA)-certified instructor scored their CPR skills using a modified Skills Evaluation Guide. After training the same participants on compression-only CPR using manikins, they were exposed (immediate post-training stage) to the same scenarios of simulated victims of OHCAs and were asked to carry out compression-only CPR to resuscitate the victims. The same instructor scored their immediate post-training CPR skills performance. Descriptive and paired T-test statistics were used to analysis the data with statistical significance set at P < 0.05. Results: The participants, 54 (77.1%) female and 16 (22.9%) male aged 17 to 30 years with mean age of 21.26 ± 2.92(SD) years, gave a statistically significant improvement in their CPR skills performance (P <0.001). While none of the participants had up to 50% in any of the skills before training, majority (78.6%) had 100% score in their post-training skills. Conclusion / Recommendation: The study has demonstrated a very effective method of impart of the bystander CPR skills to the participants. More studies on compression-only CPR are encouraged involving other Nigerian Universities and the general Nigerian public so as to increase both the awareness and the number of potential bystander CPR providers in Nigeria.
Keywords: Compression-only CPR, Nigerian University students
Cite this paper: Adedamola Olutoyin Onyeaso, Chukwudi Ochi Onyeaso, Chest Compression-only Cardiopulmonary Resuscitation in Nigerian University Students, American Journal of Medicine and Medical Sciences, Vol. 8 No. 8, 2018, pp. 213-218. doi: 10.5923/j.ajmms.20180808.08.
Article Outline
1. Introduction
- There is growing global awareness of the need for bystander cardiopulmonary resuscitation (CPR), but one of the challenges to the conventional CPR technique is the health hazard concern of health professionals and the laypersons about the risks associated with mouth-to-mouth ventilation [1-7]. The chest compression-only CPR technique has been reported to be a very effective alternative to the conventional CPR technique [8-15].Although there are reports from other countries of the world on chest compression-only cardiopulmonary resuscitation [7-10, 13, 14], there is none hitherto from Nigeria. Related previous Nigerian studies were all on conventional cardiopulmonary resuscitation technique [16-20].However, Nigeria is very much in need of relevant data in the advocacy for the incorporation of bystander CPR teaching and training into the curricula of Nigerian schools. The first ever reported attitude of Nigerian secondary school students to cardiopulmonary resuscitation (CPR) revealed that of all the questions (items) on attitude, the least favourable response from the participants was on mouth-to-mouth ventilation [21]. Also, a recent report from Nigeria confirmed also similar relatively poor attitude of Nigerian professional and student teachers to mouth-to-mouth ventilation for strangers who could be victims of out-of-hospital cardiac arrest [22].Recent studies support the usefulness of hands-only (chest compression-only) CPR in increasing secondary trainings and the overall rates of bystander CPR [23, 24].Therefore, this study aimed at assessing the pre-training and post-training cardiopulmonary resuscitation (CPR) skills performance of a cohort of University students using chest compression-only CPR technique instead of the conventional CPR method. It was hypothesized that the post-training CPR skills of the University students would not be statistically significantly better than their pre-training CPR skills.
2. Materials and Methods
2.1. Study Design
- Similar to some earlier studies [18, 19], a quasi-experimental cohort study design involving seventy (70) 200-level undergraduate physical and health education students (student teachers) in the Department of Human Kinetics and Health Education, Faculty of Education, University of Port Harcourt, Port Harcourt, Nigeria was carried out. The study took place in March, 2018. The study sample of the student teachers in the Department of Human Kinetics and Health Education were admitted in 2016 and are studying to graduate with Bachelor of Education Degree (majoring in either Health Education or Human Kinetics). They are being trained primarily to become teachers in primary and secondary schools. These student teachers are from different parts of Nigeria.The following null hypotheses were generated and tested:Ho1: that the post-training CPR skills of the University students would not be significantly better than their pre-training CPR skills. This is expected to be the test of the success or otherwise of the study.
2.2. Stage 1 (Pre-training)
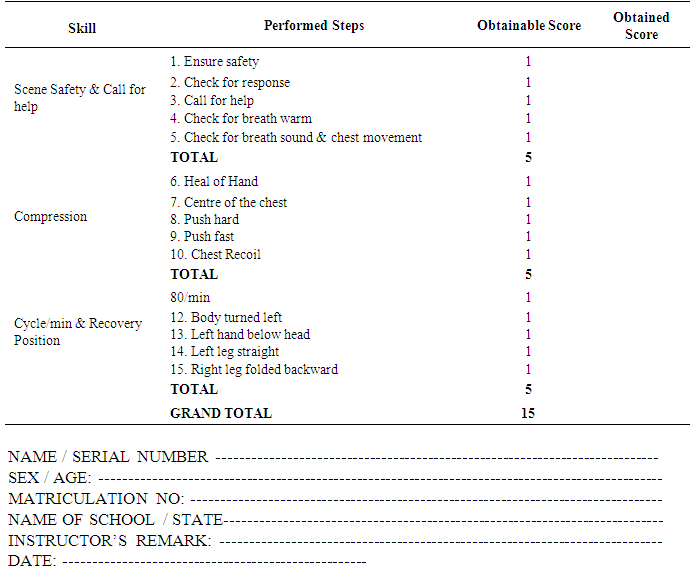
- A questionnaire containing a section for the demographic data of the participants and a section having the modified American Heart Association (AHA) ‘Skills Evaluation Guide’ to assess their pre-training cardiopulmonary resuscitation skills was used. Prior to the training on CPR, all of them were shown scenarios of victims of out-of-hospital cardiac arrests (OHCAs), using the manikins. They were asked to demonstrate what they would do in such a situation to save the victims through cardiopulmonary resuscitation without mouth-mouth ventilation. The Skills Evaluation Guide (SEG) was used to score the participants (undergraduates) pre-training skills while the questionnaire was used to obtain the demographic data of the participants.
2.3. Stage 2 (Training and Immediate Post-training)
- The teaching and training on CPR were carried out for 60 minutes using American Heart Association (AHA) CPR guideline. Their skills were evaluated using modified AHA Evaluation Guide involving three domains – (1) Scene Safety & Call for Help (S); (2) Chest Compressions (C); and (3) Cycle / min & Placement of victim in the correct Recovery Position (R) (See Appendix). After the CPR teaching and training sessions, they were then asked to individually attend to the same scenario given to them before the training and they were scored. The lead researcher, who is an American Heart Association (AHA) - certified CPR instructor assessed the CPR skills of the participants but was assisted in the teaching and training sessions by two instructors certified by the Nigerian Red Cross Society. The CPR skills were grouped into the three domains. The process of re-assessment of the CPR skills by the researcher for each of the participants took another 4 hours.
2.4. Determination of Poor and Good CPR Skills
- For each of the three (3) domains of the chest compression-only CPR skills, 50% was considered acceptable. Scores less than 50% were considered poor CPR skills while 50% and above were considered good CPR skills.
2.5. Statistical Analysis
- The Statistical Package for Social Sciences (SPSS) was used to analyze the data. In addition to descriptive statistics, one sample and two sample T-tests statistics were employed in the analysis and testing of the null hypotheses with significance level set at P< 0.05.
2.6. Ethical Approval and Participants Consent
- The participants were very glad to be part of the study because of the obvious benefit of gaining the CPR knowledge and skills so they freely gave their consent to be part of the work. Meanwhile, there was no indication for Institutional Approval because the work was considered related to the requirements for their course work in First Aid / Safety Education.
3. Results
- Figure 1 below shows the age and sex distribution of the participants with majority of the participants aged 21 years and the age range of 17-30 years. The mean age was 21.26 ± 2.92 (SD) years with 54(77.1%) as females.
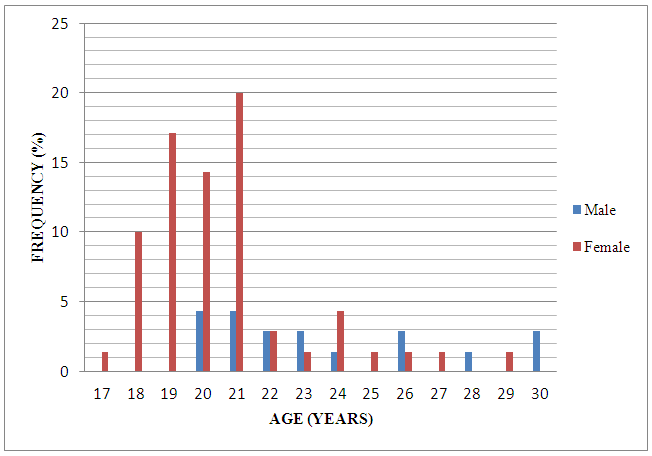 | Figure 1. Age and sex distribution of the participants |
|
|
|
4. Discussion
- This first hands-only cardiopulmonary resuscitation (CPR) study has demonstrated statistically significant improvement in the CPR skills of a group of university students following their first official exposure to CPR training. Although it was reported that conventional CPR technique resulted in better retention of the chest compression skills than the hands-only CPR training [25], hands-only CPR has been reported to be as effective as conventional CPR in acquisition of CPR skills for bystanders. [26, 27]. In addition, Kim et al [25] reported that the retention of artificial ventilation skills after conventional CPR training was poor. The very statistically significant improvement in the CPR skills of the participants in this study after the training is comparable to those of related earlier Nigerian studies that used the conventional CPR technique [18-20]. Meanwhile, the results of the study by Kim et al [25] suggested that conventional CPR with artificial ventilation performed by laypersons might provide less effective resuscitation in real cardiac arrest situations compared to hands-only CPR. They were of the opinion that lay rescuers perform hands-only CPR for adult victims of out-of-hospital cardiac arrest (OHCA), and perform artificial ventilation only if they are well-trained and have maintained the skills [25]. In fact, based on their results, they advocated for hands-only CPR to be the first-line method cardiopulmonary resuscitation training for lay rescuers [25].Despite the reported merits or advantages of hands-only CPR such as being more acceptable to lay rescuers, easier to remember and perform, and known to be as effective as the conventional [10, 11, 13-15, 28-34], one of the challenges of hands-only CPR is that it is believed that the quality of hands-only CPR decreases after the first minute following the occurrence of OHCA [28].Strengths and Limitations of this StudyThis study is not only the first ever report on hands-only CPR for lay persons in Nigeria but the sample is equally very fairly representative of youths from different parts of Nigeria because during their admission into the University the policy of ensuring a good representation from different States of the countries was followed. In addition, some of these participants (undergraduate students) when they graduate are going to become teachers in secondary schools where they will likely play important roles in teaching the secondary school students about CPR when this programme gets incorporated into Nigerian schools curricula, and thereby helping to increase the number of potential bystander CPR providers in our communities. A limitation of this study is that the training and practice of the CPR skills were simulations on manikins which are not exactly the same with real life OHCA situations.
5. Conclusions
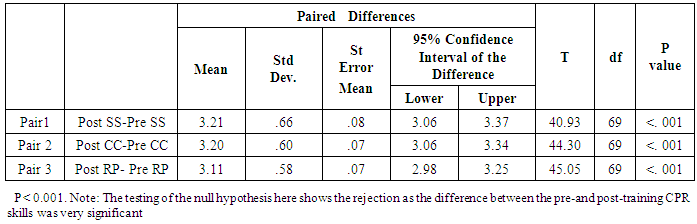
- The study has demonstrated a very effective impart of the bystander CPR skills to the participants through the hands-only CPR method with very statistically significant difference between their pre-training and their post-training CPR skills.
6. Recommendations
- More studies on compression-only (hands-only) CPR is encouraged involving other Nigerian universities and the general Nigerian public so as to increase both the awareness on bystander CPR and the number of potential bystander CPR providers in Nigeria.