Sh. E. Baymuradov, K. S. Elmuradov
Kashkadarya branch of the Republic Research Center of Emergency Medicine Kashkadarya, Uzbekistan
Correspondence to: K. S. Elmuradov, Kashkadarya branch of the Republic Research Center of Emergency Medicine Kashkadarya, Uzbekistan.
| Email: |  |
Copyright © 2018 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Treatment results of 326 patients with combined abdominal injury who were admitted to Kashkadarya branch of the Republican Research Centre of Emergency Medicine between 2001 and 2014 were analyzed. It was revealed that 235(72.1%) patients were in severe and critical conditions. A dominate injury in 163(50%) victims was an abdominal injury. The received treatment and diagnostic results showed the efficiency of the abdominal cavity injury timely detection which allowed to reduce a mortality and hospital stay duration.
Keywords:
A combined closed injury of the chest and abdomen, Peculiarities of a clinical course
Cite this paper: Sh. E. Baymuradov, K. S. Elmuradov, Treatment-Diagnostic Tactics at the Combined Abdominal Injury, American Journal of Medicine and Medical Sciences, Vol. 8 No. 8, 2018, pp. 194-197. doi: 10.5923/j.ajmms.20180808.05.
1. Introduction
A combined injury is one of the most actual medical and social issues of the developed countries [1, 3, 5]. The frequency and severity of combined injuries are constantly risen. Nowadays 60-70% of all injuries belong to the abdominal ones [2, 4, 10]. Abdominal injuries are observed in 19.6% of victims [6, 7, 15]. Mean level of lethality at the combined abdominal injuries makes up 58.5% and it is the highest one passing ahead the lethality at craniocerebral injury, traumas of the chest, the pelvis and other anatomic areas. Besides, the highest operative activity (88.3%) is registered at the combined abdominal injuries [8, 11, 13-14].Poor treatment results of victims are mainly connected with the absence of a unique surgical doctrine of medical assistance at severe combined injury, a treatment of majority of patients in the general surgical hospitals and insufficient conception of the surgeons about peculiarities of surgical tactics at the combined injuries [9, 12].The analysis of using diagnostic methods and the sequence of their application in the victims with combined abdominal injuries with the aim of treatment tactics to be enhanced is in the background of this research [4, 9, 12].
2. Aim
The goal of this investigation was to improve treatment results of the patients with chest and abdomen injuries on the base of adoption modern endovideosurgical technologies and optimization of emergency medicine organizational principles.
3. Material and Methods
Treatment results of 326 victims with combined abdominal injury admitted to the Kashkadarya branch of RRCEM between 2001 and 2014 were studied. Mean age of patients was 39.1 years. Males and females ratio made up 3.8:1 (258: 68). Car accident was a cause of injuries in 169(51.9%) patients, falls – in 80(24.5%), beating – in 54(16.6%), railway injury – in 17(5.2%), other reasons – in 6(1.8%). Alcoholic intoxication was registered in 200(61.3%) cases. Injuries of three and more anatomic areas were observed in 230(70.6%) patients.
4. Results
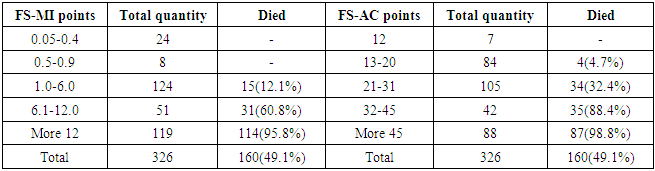
The most often abdominal cavity organs injuries were combined with craniocerebral injury (248 observations), the chest injury (117) and extremities fractures (126). 103 (31.6%) victims admitted in comatose state (7 and less points by Glasgow scale). Injury severity and patients condition at admission was estimated by field surgery – mechanical injury scale (FS-MI) and field surgery – admission condition scale (FS-AC) [2, 4] (table 1).Table 1. Patients randomization by injury and condition severities
 |
| |
|
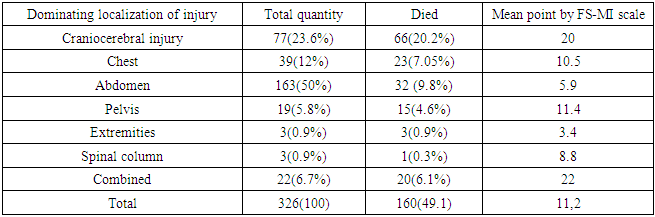
As it is presented in table 1, 235 (72.1%) patients at admission were in severe and extremely severe conditions (more than 20 points by FS-AC scale). In 294 (76.4%) cases the character of mechanical injuries was estimated as severe and extremely severe (more than 1 point by FS-MI scale). Abdominal injury was a predominant one in 163 (50%) cases (table 2).Table 2. Lethality and severity of injury subject to the predominant injury in the patients with combined abdominal trauma
 |
| |
|
Craniocerebral injury (CCI) dominated in 77(23.6%) patients, chest injury – in 39(12%). The most severe character of injuries was observed in the victims with a combination of predominant injuries (22 points by FS-MI scale) and at the CCI dominating (20.2 points). Most often we observed injuries of liver (131 cases), spleen (100 observations) and mesentery vessels (47 cases). Hollow organs ruptures occurred in 15 patients. In 77(23.6%) victims we registered multiple injuries of abdominal cavity. 160(49.1%) victims died, 17(5.2%) among them – during the first hour after admission. The main cause of death was the acute hemorrhage in combination with traumatic shock (87 observations): 76 among them died during 24 hours after admission. In later period the main cause of the death was pneumonia (29 observations) and growing brain edema with its dislocation (18 observations).The absence of abdominal cavity organs injuries clinical symptoms in the patients with combined injuries makes us give a leading role to the diagnostics by instrumental way of examination. For diagnosing abdominal cavity organs injuries 326 patients were performed: 249 – ultrasound investigation (USI), 53 – videolaparoscopy, 24 – laparocentesis. Survey radiography was performed in 97(29.8%) patients. Investigation informativity was significantly reduced due to the patients motional agitation and impossibility of performing investigation in vertical or lateral positions. In 63(64.9%) among 97 victims who were performed a survey radiography X-ray pattern did not allow to reveal or to suspect abdominal cavity organs injury. The USI at the Kashkadarya branch of RRCEM is a screening method for diagnosing abdominal injuries. Having a high sensitivity for revealing fluid accumulation, the method can be used with minimal time interval both from admission time and at the dynamic control providing information directly during the investigation. Urgent USI was performed in 249(76.4%) patients. In the cases when a primary USI did not give data about abdominal cavity pathology within first hours a dynamic control was carried out each 3-4 hours and then the investigation was performed twice a day until the patient’s transfer from the ICU to the surgical department. At the same time in 36(14.5%) patients with abdominal injuries and hemoperitoneum ultrasound pattern (in the dynamics) was uninformative. The USI data interpretation in those patients had difficulties due to a subcutaneous emphysema (16 cases), bloated bowels (7 observations), patient’s uneasy behavior or conducting resuscitation measures (4 cases), abdomen anterior wall injuries or commissural process in the abdominal cavity (3 observations). 49(15%) patients were undergone laparoscopy or laparocentesis due to insufficient USI. Diagnostic laparotomy was performed in 5(1.5%) patients due to the wrong interpretation of the USI data. A mean time from admission to the beginning of surgery in 124 victims with absolute indications for emergency surgery using the USI made up 8.4 hours. At the exclusion of 10 observations from that amount in which the examination method was broken (later USI performing and an increase of intervals between investigations up to 6 hours and more), the mean time from admission to the surgery made up 5.1 hours. As a rule, the delay with conducting the surgery was connected with an overvalue of sonography’s informativity (including a dynamic one) in the diagnostics of intra-abdominal injuries. The USI sensitivity (at the hemoperitoneum detecting) in the patients with combined abdominal injuries was 87.4%, specificity - 30%, accuracy - 87.9%. The laparocentesis was used in 24 patients, though in 22 – after USI the results of which did not allow to make a final conclusion about the nature of abdominal injuries. Indications for the surgery after laparocentesis were revealed in 12 cases. A diagnostic mistake was revealed in 1 case and it was connected with a failure of performing investigation method (a refusal from sodium chloride isotonic solution introduction into abdominal cavity). It did not allow to diagnose 600 ml limited hemoperitoneum in time. Laparocentesis sensitivity by our data made up 92.3%, specificity - 100% and accuracy – 96%. Laparoscopy was used in 53(16.2%) cases. A wrong interpretation of laparoscopy data (overstating of hemoperitoneum size) in 5 cases led to the diagnostic laparotomy. So, we observed a complication of intraperitoneal hemorrhage from the place of trocar introduction. False-negative results of laparoscopic investigation were not observed. In two cases at performing diagnostic laparoscopy in the patients with extremely severe condition we registered a sharp reduction of blood pressure which was probably caused by the insufflations of gas volume to the abdominal cavity. Mean time from admission till laparoscopy (at the exclusion of late laparoscopy cases) made up 2.9 hours. The method’s sensitivity and specificity were 100, the accuracy – 96.7%.Computer tomography (CT), as a rule, was used for a dynamic observation of parenchymatous organs intraorganic and subcapsular hematomas development which had been revealed by the USI. The use of this method allowed to detect the hematoma enlargement in 4 patients and to carry out the surgery in time; in 5 cases – to detect hematomas regression and to avoid of performing surgery. In 2 cases the CT data allowed to reveal abdominal cavity internal organs injuries which were followed by hemorrhage and to determine indications for the operative intervention. Severity condition of patients having been performed CT was not higher than 26 points by FS-AD scale. All patients had a stable hemodynamics and independent breathing.
5. Discussion
So, none of the used instrumental diagnostic methods is absolutely accurate or has some limitations. The analysis of applying diagnostic methods for detecting abdominal cavity organs injuries at the combined injury showed that the following diagnostic algorithm was the most reasonable one: - the USI is carried out within first 15 minutes after patient admission. - At the absence of intraperitoneal hemorrhage signs or at the detecting of a small hemoperitoneum the USI is repeated after 2-3 hours. - The revealing of hemoperitoneum more than 300 ml is the indication for the emergency surgery. - At uncertain USI data when it is impossible to estimate the character of intra-abdominal injuries, to our mind it is better to refuse from repeated USI but to perform a laparoscopy (in severe patients – up to 32 points by FS-AD scale) or to carry out a laparocentesis (in extremely severe condition – more than 32 points by FS-AD scale). It allows to reveal injuries being inaccessible for the sonography, to avoid of delaying surgeries or to refuse from them. - A dynamic USI with Doppler investigation and CT are reasonable to be performed at the revealing of intraorganic hematomas (liver, spleen) and at the absence of hemoperitoneum. - The augmenting of hematomas sizes, a revealing of arterial or arteriovenous blood flow in them are the indications for the surgery. This tactics was used in 167 patients. Operative interventions were performed in 107 (61.4%) of them. Mean time from admission to the surgery made up 3.4 hours. It was succeeded to avoid of diagnostic laparotomies. General lethality made up 38.9%.
6. Conclusions
Hereby, our developed treatment-diagnostic tactics allows to accelerate preoperative examination of victims with combined abdominal injury and to choose the most optimal treatment method.
Abbreviations
FS-MI scale - field surgery – mechanical injury scale FS-AC scale - field surgery – admission condition scale RRCEM - Republican Research Centre of Emergency MedicineCT - computer tomography
References
| [1] | Abakumov M.M. Actual issues of diagnostics and treatment of chest and abdomen injuries: resumes and prospects. In book: actual issues of emergency surgery. Yaroslavl, 1994, - p. 100-105. |
| [2] | Bolotnikov A.I. Diagnostics and surgical tactics at the combined car accident abdomen injury. – PhD author’s abstract, - М., 1999. |
| [3] | Briskin B.S., Smakov G.M., Karimova S.K., Potapova O. Yu. Combined injuries of peacetime. In book: Medical assistance at the combined injury. - М., 1997. - p. 82-86. |
| [4] | Bryusov P.G., Rozanov V.E. Surgical tactics in victims with combined injury. In book: Medical assistance at the combined injury. - М, 1997.- p. 64-66. |
| [5] | Bulava G.B., Abakumov M.M., Druzenko O.A. The use of leukinpheron for purulent complications prophylaxis in victims with chest wounds. Surg.-1999.-№7.- p. 36-39. |
| [6] | Gumanenko E.K. Combined injuries from injury severity condition estimation positions. - PhD author’s abstract, S-Petersburg, 1992. |
| [7] | Getman V.G. Thoracoscopy in emergency surgical pulmonoly. In book: Critical conditions at the lungs pathologies. - Kiev, 1980.-Vol 1, p. 76-79. |
| [8] | Grish L.A. The treatment of chest and abdomen penetrating wound in the conditions of rural and district hospitals. // Clinical surgery.-1971.-№4.-p. 71-72. |
| [9] | Dubrov E. Ya., Derkacheva E.V. Ultrasound diagnostics of spleen injuries. In book: Diagnostics and treatment of spleen injuries in victims with closed abdominal injuries. Vol. 145. -М., N.V. Sklifosivskiy’s Research Centre of Emergency Medicine., 2001. - p. 7-1. |
| [10] | Ermolov A.S., Abakumov M.M., Vladimirova E.S. Actual issues of diagnostics and treatment of closed abdominal injuries. In book: Actual issues of emergency surgery. - М., 1999, - p. 136-140. |
| [11] | Madiev R.Z. Treatment-diagnostic tactics at the combined injuries of chest and abdomen. PhD author’s abstract, –Tashkent., 2011. |
| [12] | Sitnikov V.N., Cherkasov M.F., Litvinov V.A. Videoendosurgical diagnostics and treatment of abdomen at the combined injury. Surgery 2006; 7: 45-50. |
| [13] | Khadjibaev A.M., Valiev E. Yu., Akhmedov R.N. treatment tactics of combined injuries of pelvis, inferior urinary tracts. Bulletin of emergency medicine 2009; 2: 38-42. |
| [14] | Khadjibaev A.M., Shukurov B.I., Khakimov A.T. Facilities of video-surgery at closed injuries of abdominal cavity organs in victims with combined injury. Bulletin of emergency medicine. 2010; 4: 23-26. |
| [15] | Yartsev P.A., Gulyaev A.A., Pakhomova G.V. The role of videolaparoscopy in the diagnostics and treatment of abdominal injury. Endoscop Surg 2008; 2: 28-31. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML