-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2018; 8(5): 99-102
doi:10.5923/j.ajmms.20180805.03

The First Experience of 3D-volumetric Computed Tomography Applying in the Diagnostics of Coronary Arteries Diseases
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLA. I. Ikramov, M. M. Zufarov, N. M. Djuraeva, A. T. Amirkhamzaev, M. M. Maksudov, N. T. Vakhidova, A. T. Sultanov, N. K. Makhkamov
Republican Specialized Scientific Research Centre of Surgery Named after Academician V. Vakhidov, Uzbekistan
Copyright © 2018 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Nowadays CT angiography rivals with invasive contrast X-ray angiography in the diagnostics of coronary arteries condition. We have used broad-detector MSCT «Aquillion One-640» (Genesis version) in the diagnostics of coronary arteries pathology and in the estimation of radiation dose in 140 patients with different frequency of heart rate. High-quality images at high heart rate and at minimal radiation dose were received.
Keywords: Coronary artery, Radiation dose, 3D-computed tomography
Cite this paper: A. I. Ikramov, M. M. Zufarov, N. M. Djuraeva, A. T. Amirkhamzaev, M. M. Maksudov, N. T. Vakhidova, A. T. Sultanov, N. K. Makhkamov, The First Experience of 3D-volumetric Computed Tomography Applying in the Diagnostics of Coronary Arteries Diseases, American Journal of Medicine and Medical Sciences, Vol. 8 No. 5, 2018, pp. 99-102. doi: 10.5923/j.ajmms.20180805.03.
Article Outline
1. Background
- Сoronary heart disease (CHD) and its complications are the most frequent cause of mortality and disability of highly developed countries’ population. The biggest quantity of sudden death cases also belong to CHD and its complications. The main cause of CHD is atherosclerosis of coronary arteries (CA). The illness takes asymptomatically for a long time due to: insignificant level of vessel’s lumen stenosis, remodeling of vascular wall, development of collateral circulation. Hereby, the early diagnostics of CA atherosclerosis before the clinical manifestations of the disease is extremely important [2].Volumetric 640 sliced computer tomography (width of detector along the axis Z 160 mm) which has started to be used for recent years in the clinical practice allows to cover the whole zone of interest (the heart) in one turn of the X-ray tube. We have analyzed 140 investigation results of patients performed coronary arteries computer tomography (CACT) – a retrospective analysis of the cardiac rate changes effect on the radiation dose (RD).
2. Objective
- To assess the capacity of volumetric CT and analyze the results of coronary artery studies of patients with different heart rate, compare E on 128 and 640 sliced CT.
3. Material and Methods
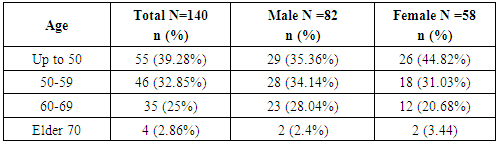
- 140 patients with CHD were examined. The patients were randomized in 2 groups: 1 - 98 (70%) cases in the group with heart rate (HR)<80 per min; 2 group – 42 (30%) cases with HR >80 per min. We have done a retrospective analysis of 140 patients with diagnosed CHD, with suspicion on CHD and also the patients after coronary arteries (CA) stenting. Patients age was 35-60 years, males were 82 and females – 58 (table 1).
|
4. Results
- The main advantage of this system is a possibility of volumetric scanning of the object up to 16 cm for 0.275 sec (during ultra-short period of time, without desk shift and therefore, without artefacts from movement). Radiation exposure made up 1.4-3.2mЗв (2.32 ± 0.41) at prospective investigation and 2.5-7.5mЗв (5.86 ± 1.33) at retrospective investigation. According to the experience of using 128 sliced CT it was revealed that the consumption of CM made up 75-100ml((Unigexol 350) (<70 kg 4.0 ml/sec, 70-100kg 5.0ml/sec)), radiation dose at prospective investigations was 4.5-8.0 mЗв, at retrospective ones – 9.0-17.0 mЗв, it is significantly higher vs the investigations done by wide-detector tomography (table.2).
|

5. Preparation of Patients for CACT
- Patients with HR>80 per min required to take beta-blocker in therapeutic dose subject to the absence of contraindications and sublingual absorption of isosorbide dinitrateа 1.25 mg directly before the scanning. All the patients signed an informational agreement about scanning process and possible complications. We have used a segmental classification of coronary arteries (CA) of the American Society of Cardiovisualization (SCCT) according to which CA are divided into 18 segments [fig.1] [3].
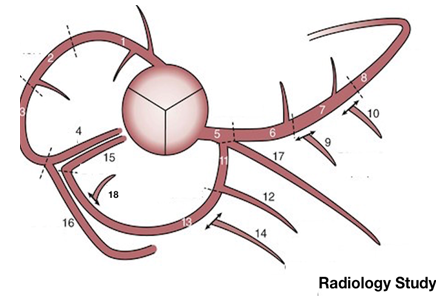 | Figure 1. Segmental classification of CA developed by the American Society of Diagnostician (addition from 2010): 1 – a right coronary artery, proximal one-third; 2 - a right coronary artery, mean one-third; 3 - a right coronary artery, distal one-third; 4 - posterior descending artery; 5 – a left coronary artery, main trunk; 6 – anterior descending artery, proximal one-third; 7 - anterior descending artery, mean one-third; 8 - anterior descending artery, distal one-third; 9 – the first diagonal branch; 10 – the second diagonal branch; 11- circumflex artery, proximal part; 12 - obtuse marginal branch; 13 - circumflex artery, distal part; 14 - obtuse marginal branch № 2; 15 - posterior descending branch; 16- posterolateral branch, diverging from the right coronary artery; 17 - intermediate artery; 18 - posterolateral branch, diverging from circumflex artery |
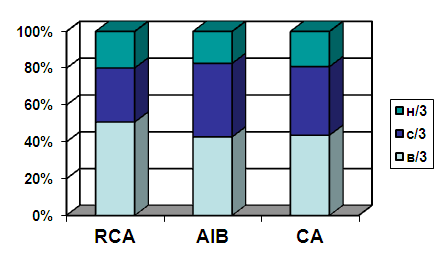 | Figure 2. Percentage of segmental involvements of CA (n=140) |
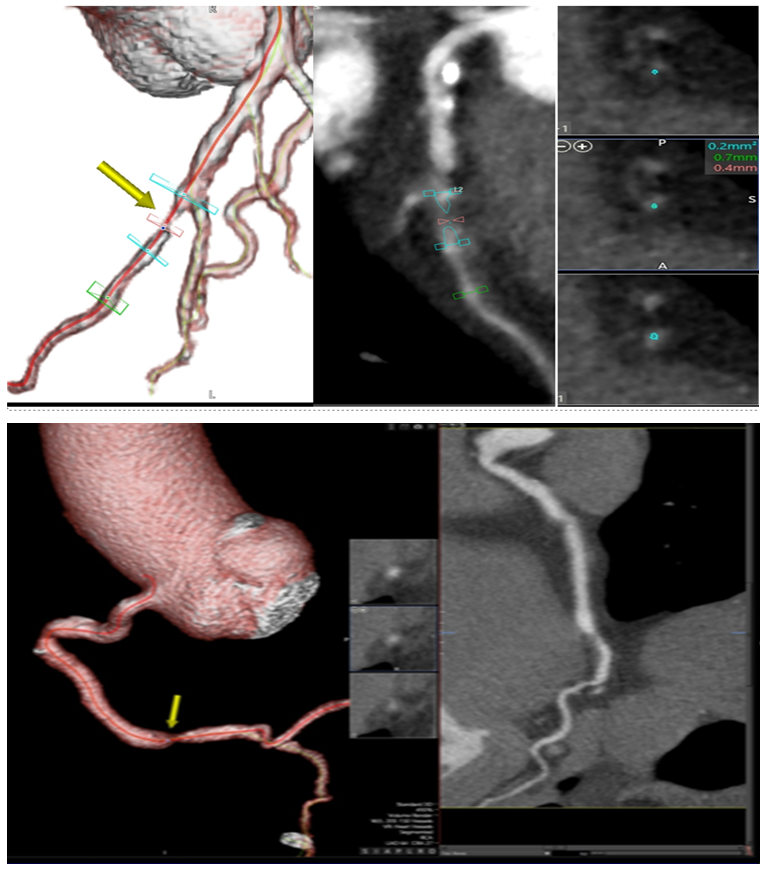 | Figure 3. Three-dimensional reconstruction of the coronary arteries and it’s tracking. Stenosis of the LAD (8 segment) on MSCT (soft-tissue plaque) |
6. Scanning Parameters
- The voltage of scanning tube was 100 kV, modulation of current was used in concordance with body build index. Time of data collecting at prospective scanning made up 70 ~ 80% between RR period; at retrospective scanning - 0 ~ 90% of RR interval. The rate of contrast medium (CM) introducing made up 5.0-5.5 ml /sec (55-70 ml). ROI was installed on the descending aorta to control CT values, with operation threshold +300 HU. When ROI volume reached +300 HU, the scanning was ran automatically.
7. Estimation of Radiation Dose
- We estimated DLP and effective dose (ED). ED will be calculated with the use of DLP (mGr*cm) multiply to e; e – dose index for appropriate anatomical area (0.017 mSv/mGr*cm) according to the quality criteria of the European Committee of CT standard [4].
8. Discussion
- Abada et al. [5] discovered the reduction of RD to 80% by applying 80 kV at CT of CA in compare with 120 kV. Pflederer et al [6] got 39% -fold reduction of RD using 100 kV at CT of CA in compare with 120 kV. We did not observe significant differences in the quality of CA segments images, RD was significantly reduced to 12-15% in compare with scanning protocol with 120 kV tube voltage.
9. Correlation between HR and Image Quality
- The heart is a moving organ and image quality of CA mainly depends on resolving time. Resolving time of 640 sliced CT is 0.275 second and 160 mm detector allows to cover the whole heart with one turn of gentry – optimal visualization of CA – it allows to keep a high quality of image in the wide range of HR. The influence of HR to image quality mainly depends on resolving time of CT [7]. Besides, 640 sliced CT automatically ignores abnormal cardiac cycle waiting for the next normal cardiac cycle providing a high image quality in patients with arrhythmia.
10. Correlation between HR and RD
- CT of CA has an advantage of non-invasive and high precision diagnostics [8] and is used in clinical practice in several aspects. But X-ray ionizing radiation of CT decreases the risk of malignant neoplasms. Therefore, it is very important to reduce RD without the loss of image quality. We performed prospective scanning at HR<80 per min and retrospective scanning – at HR>80 per min. As HR is higher RD is also bigger. At some cases at not high HR but at arythmic pulse we had to choose a retrospective mode for getting qualitative images.
11. Conclusions
- Thereby, wide detector computed tomographic scanners allow to perform CT of CA in ultra-short period of time without artifacts from movements at high HR up to 95 per min. A significant reduce of radiation dose and a quantity of contrast medium is necessary to be mentioned. 3D CT of CA can be adapted to the different HR providing a high quality of image at low radiation dose.