-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2018; 8(4): 61-65
doi:10.5923/j.ajmms.20180804.02

Obesity Indices and Serum Total Prostate Specific Antigen among Hausa Ethnic Group of Northern Nigeria; A Community Survey
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSalisu Muazu1, Bello Ahmad2, Hauwa Bako3
1Consultant Physician/Endocrinologist, Department of Internal Medicine, Rasheed Shekoni Specialist Hospital, Dutse and Ahmadu Bello University, Zaria, Nigeria
2Consultant and Associate Professor of Urology Urology Unit, Department of Surgery Faculty of Medicine Ahmadu Bello University Zaria, Kaduna State, Nigeria
3Chemical Pathology Unit Department of Medical Laboratory Sciences, Rasheed Shekoni Specialist Hospital, Dutse, Jigawa State, Nigeria
Correspondence to: Salisu Muazu, Consultant Physician/Endocrinologist, Department of Internal Medicine, Rasheed Shekoni Specialist Hospital, Dutse and Ahmadu Bello University, Zaria, Nigeria.
| Email: |  |
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

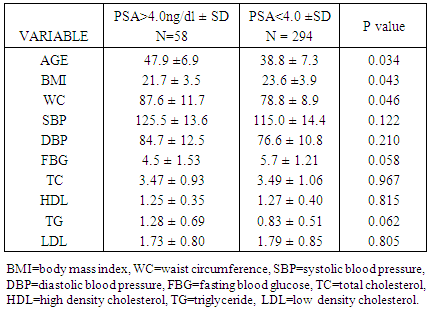
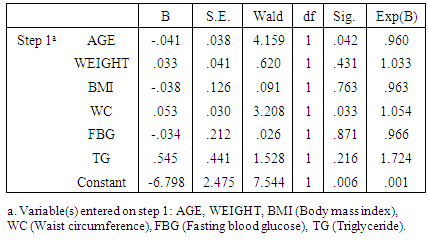
Background: Previous studies among Caucasians have shown that linear obesity exhibit an inverse relationship with serum total prostate-specific antigen (PSA). Similar study has not been conducted in this region of the world and also the relationship between obesity indices with serum PSA is not known. We therefore intend to investigate the influence of obesity and related indices on serum PSA levels. Methods: The subjects comprises of 352 healthy men of Hausa tribe extraction who consented and fulfilled the study inclusion criteria. The data obtained included, anthropometric and other physical examinations measurement which were recorded in a proforma. The body mass index and waist circumference assessed and serum prostatic specific antigen (PSA), lipids, glucose and thyroid stimulating hormone (TSH) were estimated. We compared serum PSA and other variables and performed logistic regression to find association between variables using SPSS 23 software. Results: A total of 352 adults were screened with mean age 39.6(9.4) years and mean serum total PSA of 2.73(4.10)ng/ml. The prevalence of elevated serum PSA was 16.5% (58/350). The overweight (BMI=25-29.9) 15.3% had significant high PSA level than underweight (BMI=<18.49) 12.5%, normal weight (BMI=18.5-24.49) 68.2% and obese (BMI>30) 4.0% as shown; 4.10, 2.37, 2.53 and 1.65 ng/dl respectively. p=0.013. The pre-diabetes 14.7% had high serum PSA value (3.40ng/dL) than diabetic 3.7% (2.01ng/dL) and normal glycaemia 81.8% (2.70ng/dL) Anova, p=0.019. The triglyceride (TG) had a significant positive correlation with the serum PSA (r= 0.198, p=0.012). Logistic regression showed positive linear relationship between waist circumference and age with total serum PSA. p=0.033. Conclusion: The waist circumference and age were positively associated with total serum PSA. There is need for caution when interpreting PSA screening test in the pre-obese, obese and pre-diabetic in this community.
Keywords: PSA, Waist circumference, Overweight, Obesity, Pre diabetes
Cite this paper: Salisu Muazu, Bello Ahmad, Hauwa Bako, Obesity Indices and Serum Total Prostate Specific Antigen among Hausa Ethnic Group of Northern Nigeria; A Community Survey, American Journal of Medicine and Medical Sciences, Vol. 8 No. 4, 2018, pp. 61-65. doi: 10.5923/j.ajmms.20180804.02.
Article Outline
1. Introduction
- The prostatic specific antigen (PSA) is a glycoprotein produced by the epithelial cells of both normal and cancerous prostate gland. Its regulation is under the control of androgens and progestins. Elevated serum PSA concentrations are known to be connected with three most common prostatic diseases, including prostate cancer, benign prostatic hyperplasia and prostatitis. [1] Prostate specific antigen levels are also affected by many factors that may be unrelated to prostate disease, including familial, age and race. [2]Serum PSA is age dependent, it tends to increase with age because the prostate enlarges with age and contains more PSA-producing tissue. [3] Although, the test lacks both the sensitivity and specificity to accurately detect the presence of prostatic diseases, it is a veritable prostate specific marker and can be used as a valuable tool for detecting and monitoring of prostate cancer.Previous reviews and studies have documented that both diabetes and obesity were associated with lower levels of serum PSA. [2, 4, 5] In Japanese population it was found that long standing diabetes and obesity tend to have lower serum PSA while overweight group was associated with higher PSA. [2] Although obesity is positively associated with prostate volume however, increasing body mass index and waist circumference maintains an inverse relationship with serum PSA irrespective of the prostate volume. [6] This support the previous finding that the lower serum PSA associated with obesity is perhaps due to haemodilution secondary to large plasma volume in obese men rather than prostate volume. [7]Furthermore, it was reported among the Koreans by Park SG et al [8] that BMI, waist circumference and subcutaneous adipose tissue were inversely associated with serum PSA but no observed relationship with visceral adipose tissue. When adjusted for visceral adipose tissue, body mass index was not associated with prostate volume. This implied that visceral adiposity is the main determining factor of the prostate volume increase and prostate specific antigen production.Body mass index seems to play a pivotal role in serum total PSA levels irrespective of presence or otherwise of obesity. The increasing BMI is associated with rising plasma volume, which in turn, progressively dilutes the serum PSA leading to lower levels. [7] A study by Culp S et al [9] showed a significant inverse relationship between increasing BMI and serum PSA among White non-Hispanic Americans. Similarly, Chia SE et al [3] found among Chinese and other Asians a concordance finding, using both the standard and Asian BMI classification, especially in the elderly.Metabolic syndrome and its individual components are also found to influence the levels of serum PSA in a heterogeneous manner. Among the components, hypertension is the most consistently associated with raised PSA levels as revealed by several meta analyses. [10-12] In addition, a study by Han JH et al [5] showed an inverse relationship between the body mass index, HDL, and FBG with the serum PSA level while Gacci M et al [13] in a recent review also reported an inverse relationship between metabolic syndrome and serum PSA level. The serum PSA is use, as a surrogate marker, in combination with other procedures, for the detection and monitoring of prostate cancer among the adult males. However, serum PSA testing of men at normal risk of prostate cancer is one of the most contested issues in cancer screening.The evolving urbanization process affecting the developing nations including Nigeria, comes with an increase in incidence of non-communicable diseases including obesity. Furthermore, studies have also shown a disproportionate burden of morbidity and mortality associated with prostate cancer among men of West African ancestry. [14-16]Obese men may have lower baseline prostate specific antigen and thus be at a higher risk for having prostate cancer undetected in a prostate specific antigen screening test. [6, 7]In view of the increase in morbidity and mortality associated with obesity, which is on the increase in this community and the significance of serum PSA in screening of prostate cancer and a study of this nature has not been done in this region. We undertake to document the association between obesity and serum total PSA and related factors in this community.
2. Materials & Methods
- The survey was conducted in a semi-urban community in Jigawa state of North Western Nigeria comprising 352 healthy men of Hausa tribe extraction. The subjects included peasant farmers, traders, artisans and middle cadre civil servants.Simple random sampling technique was used to recruit consenting adults who fulfilled the inclusion criteria including; adults male with no symptoms of prostatitis or evidence of urinary obstruction, not on drugs that may temper with PSA levels like finasteride, prostate biopsy or surgery.The study protocol was approved by the local health authority and the hospital ethical committee of the Jigawa state specialist hospital, Dutse.The data obtained included personal history, anthropometric and blood pressure measurements were conducted and recorded in a pre-designed and tested questionnaire. Body mass index was calculated using the formula weight in kilogramme/height square in metres while waist circumference in centimetres was determine at the largest mid abdominal diameter. The BMI was further categorise into; underweight (BMI<18.49), normal weight (BMI=18.5-24.49), overweight (BMI=25-29.9) and obese (BMI>30).On second visit subjects were instructed to fast overnight. A fasting venous blood was taken for the estimation of serum prostatic specific antigen (PSA), total cholesterol (TC), low density lipoprotein cholesterol (LDL), high density lipoprotein cholesterol (HDL), triglycerides (TG), glucose and thyroid stimulating hormone (TSH).Serum total PSA was determined using AccuBind Enzyme Link Immuno assay (ELISA) Microwells while enzymatic and glucose oxidase methods were used for fasting cholesterol, triglyceride and glucose estimations.Diabetes mellitus diagnosis is in accordance with WHO criteria, 2003, comprising of Normal glycaemia = (FBG <5.5>2.2mmol/L), Impaired glycaemia or pre-diabetes = (FBG=5.6-7.0mmol/L and Diabetes = (FBG>7.1mmol/L).Serum PSA levels of >4.0 ng/ml was considered high or risk of prostate cancer.
3. Statistical Analysis
- The data was analysed using SPSS package version 23.0 and presented as mean ± standard deviation, correlation coefficient (r-value) using Pearson’s correlation and regression analysis with p<0.05 level as significant.
4. Results
- A total of 352 adults were screened with mean age 39.6(9.4) years and mean serum total PSA of 2.73(4.10)ng/ml. The proportion found with total serum PSA >4.0ng/ml was 16.5% (58/350) figure 1.
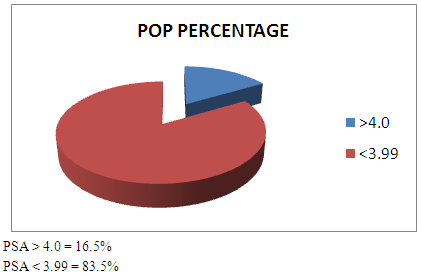 | Figure 1. Showing the percent distribution of PSA values among the study population |
|
|
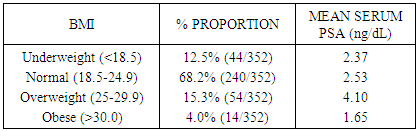
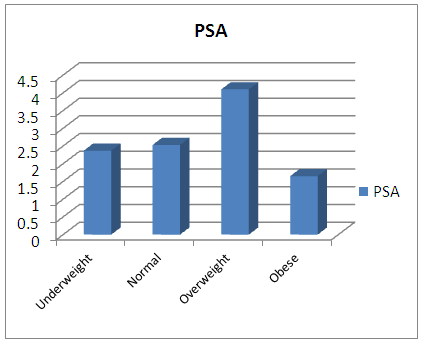 | Figure 2. Showing the bar chart distribution of Prostatic Specific Antigen (PSA) among the Body Mass Index (BMI) sub groups of the study population |
|
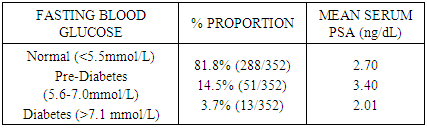
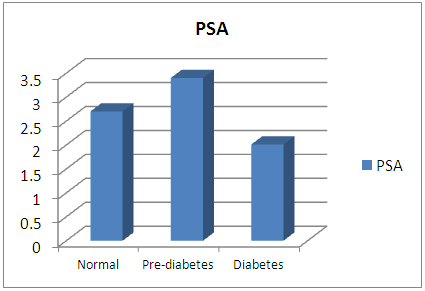 | Figure 3. Showing bar chart distribution of Prostatic Specific Antigen (PSA) among normal glycaemia, pre-diabetes and diabetic sub groups of the study population |
|
5. Discussion
- In this study 16.5% of the study population was found to have elevated serum total PSA (> 4.0ng/dl). Age and waist circumference were found to be higher in those with elevated serum PSA. Among the BMI sub class, the overweight had significant high serum PSA whereas obesity had lowest. The pre-diabetes subgroup also had the higher serum PSA than diabetes and in normal glycaemia groups.The prevalence of raised serum PSA level recorded in this study is on the high side considering the relatively low mean age of the study population. It is known fact that there exist a positive linear relationship between age and serum PSA levels which means the older the subject is the higher the serum PSA level. [3]Previous similar studies by Akinremi T et al [16] had documented in southern Nigeria a prevalence of 11.2%, Hsing A W et al [15] found 16.0% in a survey involving of screening adult males in Ghana while Oesterling JE et al [17] reported lower rate among the White non Hispanic Americans. This goes further to give credence to the finding that people of West African descent are prone to higher serum PSA levels perhaps due to high prevalence of prostate diseases or influence of unknown genetic and environmental factors.Although there was an inverse relationship between obesity and the serum PSA levels however, there was a direct relationship between the BMI and the serum PSA among the three subgroups of BMI excluding the obese class. The overweight category of subjects, (BMI of 25-29.9), showed a paradoxical rise in PSA level above all other categories of BMI. This finding is in concordance with several studies among the Japanese, the Europeans and the Koreans. [6, 7, 9] The preceding finding may be explained by the hypothesis that; overweight condition i an insulin resistance situation that is characterise by hyperinsulinaemia and excessive production of insulin like growth factor 1. It is known that, IGF-1 to stimulate growth of both, the prostate gland and other androgen-sensitive cancers, leading to production of excess PSA, via mediation of growth hormone action especially in the presence of low levels of IGF-1 binding protein. [18, 19]The serum total PSA decreases with increasing blood glucose levels especially among the elderly. The pre-diabetes group had significantly high serum PSA values than both the normal glycaemia and diabetic range groups. A community study by Naito M et al [2] among the Japanese, suggested that the overweight men had increased PSA levels, while diabetes was associated with a reduction of PSA levels in elderly. This finding perhaps may also be explained by the same principle of insulin resistance leading to hyperinsulinaemia, excess IGF-1 and hence increase in serum PSA production. [18] Despite documenting an inverse relationship between linear obesity with serum PSA levels in this study, nonetheless, the waist circumference was found to be positively associated and or predictor of raised serum PSA. Park SG et al [8] had previously reported among the Asians that waist circumference, visceral and subcutaneous adipose tissue were positively associated with prostate specific antigen. He went further to show that the visceral adiposity, associated with the increasing waist circumference, is the main determining factor for the increase in prostate volume and prostate specific antigen production.Other metabolic parameters including triglycerides was positively correlated while hypertension was weakly associated with serum PSA levels though it has not attain statistical significance. A recent review by Liang Z et al [12] has reveals a consistent positive relationship between hypertension and serum PSA. The failure of our results to attain level of significance with regard to hypertension may be attributed to the relatively small sample size used or other intrinsic characteristics of the subjects.
6. Conclusions
- The serum PSA among this naive community is high (16.5% of the study population) and is associated with overweight and pre diabetes sub groups. The age and waist circumference were found to be predictors of elevated PSA in this study. It is thus concluded that advance age and central adiposity, as depicted by increasing waist circumference, are risk factors for prostate cancer among the subjects studied. The implication of this result is that waist circumference may be used as a preliminary screening tool to detect elevated PSA and thus increase suspicion of prostate cancer, especially in the elderly group. However, there is need for caution with regards to interpreting PSA levels among overweight and pre-diabetic subjects where the baseline PSA is high. The low serum PSA associated with linear obese may be at a higher risk for having prostate cancer undetected in a prostate specific antigen screening test.It is imperative to engage the community members on health education and awareness programme to educate them on dangers associated with obesity and diabetes especially with regards to morbidity and mortality of chronic medical conditions including prostate cancer.The strength of the study lies in its idea and contents while lower mean age of the subjects and inability to measure the insulin and visceral adiposity to ascertain the supposedly hyperinsulinaemia among the overweight and the pre-diabetes subjects, might have reduce the power of the survey to make a definitive inference. It is therefore recommended that future studies on this topic to involve measurement of insulin and estimation of prostate size among the overweight and pre-diabetes so as to find the relationship between the hyperinsulinaemia, the volume of the prostate and the waist circumference with the PSA levels. There is also a need to look at the possibility of establishing BMI class specific cut off values for PSA in a larger sample and multi centre survey.