-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2018; 8(4): 55-60
doi:10.5923/j.ajmms.20180804.01

Attitude of Student Teachers to Cardiopulmonary Resuscitation in Relation to Their Gender and Age
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAdedamola Olutoyin Onyeaso1, Onyedikachi Oluferanmi Onyeaso2
1Department of Human Kinetics and Health Education, Faculty of Education, University of Port Harcourt, Port Harcourt, Nigeria
2Department of Preventive and Social Medicine, University of Port Harcourt Teaching Hospital, Port Harcourt, Nigeria
Correspondence to: Adedamola Olutoyin Onyeaso, Department of Human Kinetics and Health Education, Faculty of Education, University of Port Harcourt, Port Harcourt, Nigeria.
| Email: |  |
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Introduction: School teachers are central to the success of increasing the number of potential bystander CPR providers through CPR training programmes in schools and eventually in the larger communities. Nigeria is yet to take any meaningful step in this direction. This study aimed to assess impact of gender and age on the attitude of Nigerian teachers towards bystander cardiopulmonary resuscitation (CPR). Methods: A quasi-experimental study design was carried out involving 41 males and 41 females divided into two age groups: 17-20-year-olds and 21-28-year-olds. Using a self-administered questionnaire, the attitude of the participants (student teachers in a Nigerian University) towards bystander CPR was assessed before and after a bystander CPR training programme using internationally accepted standards. The data was analysed using both descriptive statistics and ANOVA. Results: Although neither gender nor age of the participants revealed any statistically significant association with bystander CPR (P > 0.05), both sexes and the age groups generally showed a positive attitude towards bystander CPR. Before the CPR training, female gender and the younger age group showed better positive attitudes towards bystander CPR but the findings were not statistically significant (P > 0.05). Conclusion: Both sexes and age groups had positive attitude to bystander CPR. However, none showed statistically significant association to attitude towards bystander CPR. There is need to repeat the study with a larger sample size in different communities.
Keywords: Age, Gender, Relationship, Bystander CPR
Cite this paper: Adedamola Olutoyin Onyeaso, Onyedikachi Oluferanmi Onyeaso, Attitude of Student Teachers to Cardiopulmonary Resuscitation in Relation to Their Gender and Age, American Journal of Medicine and Medical Sciences, Vol. 8 No. 4, 2018, pp. 55-60. doi: 10.5923/j.ajmms.20180804.01.
Article Outline
1. Introduction
- Attitude is a predisposition or tendency to respond positively or negatively towards certain idea, object, person, or situation [1]. Attitude influences an individual’s choice of action, and responses to challenges, incentives, and rewards (together called stimuli) [1]. Although bystander cardiopulmonary resuscitation (CPR) has the potential of increasing survival for out-of-hospital cardiac arrest (OHCA) by up to four times, but the rate of bystander cardiopulmonary resuscitation (CPR) remains relatively low in many countries of the world ranging from 19.0 to 104.0 per 100,000 population per year and varying rates of survival [2, 3].The results of EuReCa ONE still indicate that out-of-hospital cardiac arrest (OHCA) remains a major public health challenge which accounts for substantial deaths in Europe [2]. It was reported that survival rates increased amongst those who received bystander CPR and public access defibrillation [4, 5].Meanwhile, attitude to bystander CPR remains crucial in maximizing the usefulness of bystander CPR in increasing the survival rates across nations in the face of increasing out-of-hospital cardiac arrests (OHCA). Several studies have looked at the attitudes of different populations to cardiopulmonary resuscitation and the challenges to successful bystander CPR [6-14]. It was concluded that quality of undergraduate education affects the work of CPR trainers and the train-the-trainers courses should focus more on practical scenarios and nontechnical skills, among other things [6]. Among other barriers, fears of contracting infectious diseases, harming the victim further and legal litigation, poor CPR knowledge, lack of adequate provision of CPR skills to teachers, age of participants and poor attitudes have been highlighted as important challenges or barriers to bystander CPR and the successful implementation of CPR training in schools [7-15].School teachers play very important role in having effective school CPR programmes. Despite the global call and acceptance of having CPR training in schools [16, 17], Nigeria is yet to give adequate attention to this. Consequently, there are limited published studies on the attitude of school teachers towards cardiopulmonary resuscitation [18, 19]. Still in search of basic important data on bystander CPR for informed decision in our bid to incorporating bystander CPR training in our schools and by extension in our communities, the present study aimed at assessing the possible influence of age and gender on the attitude of a group of Nigerian student teachers.
2. Materials and Methods
- Study Design and SettingThis is part of major quasi-experimental cohort study design carried out in the Department of Human Kinetics and Health Education, Faculty of Education, University of Port Harcourt, Port Harcourt, Rivers State, Nigeria.ParticipantsForty one (41) male and forty one (41) female undergraduate students of Human Kinetics and Health Education with 40 participants in the 17-20 years age group and 42 participants belonging to the 21-28 years of age bracket were randomly selected from the larger main cohorts for analysis of the possible impact of age and sex on their pre-training and post-training attitude towards cardiopulmonary resuscitation (CPR).The student teachers in the Department were admitted in 2015 through an established quota system that ensures fair representation from all the states in Nigeria during the admission process. They are to graduate with bachelor degree in Education with bias in either Human Kinetics or Health Education. By their training they are expected to teach in the primary and secondary schools in the country.The Null hypothesesWe generated and tested the following null hypotheses:Ho1: That there would be no significant differences in the pre-training and post-training attitudes towards CPR of the student teachers with respect to sex.Ho2: That there would be no significant age impact on the pre-training and post-training attitudes towards CPR of the student teachers.Stage 1 (Pre-training)A questionnaire containing a Section for the demographic data of the participants and a Section having the questions testing their attitude towards cardiopulmonary resuscitation (CPR), as well as a Section on modified AHA ‘Skills Evaluation Guide’ for assessment of their CPR skills. Prior to the teaching and training on CPR, all of them answered the questions on attitude to bystander CPR. This paper addresses their attitude towards CPR with respect to their age and gender.Stage 2 (Training and Immediate Post-training)The teaching on CPR was carried out for 60 minutes using both power points projections and video films in line with internationally accepted standards [20]. The process of training them on hands-on and re-assessment took another 3 hours. During the re-assessment, the participants were asked again to respond to the same questions on attitude towards CPR which they had during the pre-training period on attitude towards bystander CPR.Determination of ‘Positive CPR Attitude’ and ‘Negative CPR Attitude’Four options were available to the participants for each of the fourteen items/questions testing the attitude of the participants to cardiopulmonary resuscitation: strongly agree (SA), agree (A), disagree (D) and strongly disagree (SD). Strongly agree has 4 points, Agree – 3 points, Disagree – 2 points while Strongly disagree attracts 1 point. Any score on any of the items or questions that is 3 or 4 means positive attitude while any score of 2 or 1 shows negative attitude.The methodology of this work had been previously reported [19, 21].Statistical AnalysisThe Statistical Package for Social Sciences (SPSS) was used to analyze the data. In addition to descriptive statistics, analysis of variance (ANOVA) was used in the analysis and testing of the null hypotheses with significance level set at P < 0.05.Ethics or Review Board ApprovalThis was not applicable. There was no need for Institutional Ethical Approval because the procedure was completely non-invasive and within the learning needs of the participants. However, the participants gave their consent before being allowed to participate in the study.
3. Results
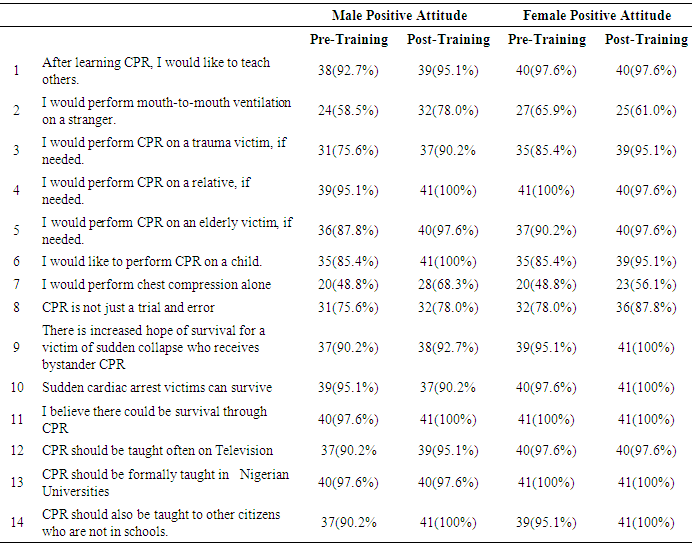
- Table 1 shows the frequency distribution of the positive responses of the participants to questions on attitude to bystander CPR in relation to gender with female participants showing better positive attitude towards bystander CPR than the male counterparts, although both sexes generally have positive attitude to bystander CPR. On willingness to give mouth-to-mouth ventilation to a stranger who is a victim of cardiac arrest during the pre-training phase of the study, more female participants (65.9%) were willing while 58.5% male counterparts were willing Willingness to provide mouth-to-mouth ventilation by the female participants dropped to 61% while the male counterparts increased to 78% after the CPR training. On increased hope of survival for a victim of sudden collapse who receives bystander CPR, the responses of the participants improved from 90.2% to 92.7% for male participants and from 95.1% to 100% for the females from pre-training to post-training phases of the study.
|
|
|
|
4. Discussion
- This quasi-experimental study has shown that neither gender nor age has any statistically significant impact on their attitude toward CPR. However, it must be noted that descriptive statistics showed that the female gender and the younger age group generally tended to show better positive attitudes to bystander CPR before the training but those were not statistically significant. However, for mouth-to-mouth ventilation on victims of cardiac arrest who are strangers, the percentage of female participants who agreed to provide such when the need arises dropped in the post-training assessment. This could be due to the fact that after the practical session of what is involved in giving mouth-to-mouth ventilation, some of the female participants who had accepted to offer the service felt otherwise either because of the fear of possibly getting infected with diseases such as human immunodeficiency virus (HIV), tuberculosis and other infectious diseases due to the level of intimacy involved. Interestingly, more of the male participants opted after the CPR training to provide mouth-to-mouth ventilation for strangers who may be victims of cardiac arrest needing bystander CPR. The reverse situation with the male participants could be attributed to male tendency to bravery.Similarly, the younger age group indicated better interest to carry out mouth-to-mouth breathing for victims before training but this dropped during the post-training assessment. The reverse was the case for the older age group. This could be because the older age group changed positively better towards this aspect of bystander CPR because of the importance, while fear must have affected the younger age group contrary. Previous reports have shown that the fear of contracting infectious diseases has been expressed as a setback to successful layperson bystander cardiopulmonary resuscitation provision [13, 14, 22]. Parnell et al [10] reported that 47% of their participants indicated unwillingness to carry out mouth-to-mouth CPR on strangers while the present Nigerian study records 41.5% (pre-training) and 22% (post-training) for males and 34.1% (pre-training) and 39% (post-training) for females.In a related University-based study in Lebanon, Shams et al [23] reported that the attitude towards the importance of bystander CPR and the need to learn CPR among the youths was very positive. However, their study did not look into gender or age differences in attitude towards cardiopulmonary resuscitation. In another similar study by Guijpers et al [24], the CPR training provided by physical education student teachers was found to be of comparable quality with that provided by nurses who were the usual providers of CPR training. They further concluded that physical education student teachers could be recruited to teach CPR to secondary school students. Our current study on the attitude of the Nigerian physical and health education student teachers supports their finding when the high positive attitude of our participants towards bystander CPR is considered. Considering the immense importance of encouraging bystander CPR training in our environment due to the fact that people who live in low income neighbourhoods that are primarily black or poor have higher tendency of having out-of-hospital cardiac arrest, and are more unlikely to receive bystander CPR as well as having less chances of survival [25], makes the present finding of no significant gender differences in attitude towards CPR from this Nigerian study a positive one. This means that both male and female student teachers promising potential bystander CPR providers in our community as well as CPR trainers in our secondary schools. However, a religious barrier to bystander CPR was documented by Schmid et al [22] where some participants believed that performing CPR was against the will of God and this was associated with unwillingness to attend CPR training class and performing bystander on strangers. The possibility of this playing a role in bystander CPR training and practice Nigeria needs to be explored considering the two major religions in Nigeria (Christianity and Islam). The current study was carried out in South-south Nigeria dominated by Christianity. An earlier related study in Nigeria [26] had reported no association between gender and the attitude of some secondary school students in Nigeria which is supported by the present study involving Nigerian undergraduate student teachers.Al-Turkistani [27] reported that 15.5% female attended CPR course compared to 6.1% male; 18.7% had watched some CPR programme /clips on television or online compared to 11.1% male, and 59.4% female were willing and eager to attend CPR courses whenever available compared to 29.3% male. The educational (postsecondary education) level of their female/male participants was 37.5% / 21.9%, respectively but 84.3% females and 91.2% of males did not know when to perform mouth-to-mouth ventilation and /or chest compression. In our present study, both the male and female participants have the same level of education and the pattern of the findings in terms of better positive attitude of the females toward bystander CPR is similar to that of Al-Turkistani [27] though not statistically significant. No statistically significant gender difference was observed in relation to attitude towards bystander cardiopulmonary resuscitation among radiology technologists in Ahvaz, Iran [28]. However, both sexes had positive attitudes to bystander CPR, just like in this Nigerian study.According to Mpotos et al [9], primary schoolteachers and the age group of 21-30 years were most willing to teach CPR. Our present study revealed that 97.5% of the student teachers in age group 17-20 years were willing to teach others both in the pre-and post-training stages of the study while 92.9% in the pre-training stage and 95.2% in the post-training stage in the 21-28 years age group were willing to teach others bystander CPR. Meanwhile, it was reported that students had better positive attitude to CPR than their parents [15].It was reported by Stroobants et al [28] that trainees of primary schoolchildren had better score for the test and positive change of attitude towards future bystander cardiopulmonary resuscitation than those of secondary schoolchildren. It must be emphasized that the trainees of primary schoolchildren were naturally younger in age than the secondary school counterparts.In a related study, Axelsson et al [30] reported, among other findings, that 97% of their participants were willing to start CPR on a relative while 91% on a known person. They reported that there was high readiness to perform CPR on a known person among the trained CPR rescuers; while hesitation about performing CPR on a stranger was evident. These findings are comparable to the findings in our present Nigerian study.Strength and Limitation of this studyAlthough a quasi-experimental study design involving participants (student teachers) from relatively many states of the country thereby making it a fairly representative sample, it must be noted that not every state in the country was represented. Therefore, the sample was not a perfect representative one. The Significance of the StudyThis study has provided important baseline data on the impact of gender and age on the attitude of Nigerian potential teachers towards cardiopulmonary resuscitation (CPR), showing that there is neither gender nor age bias in attitude towards bystander CPR. The findings in this study are encouraging for such an important subject of growing international concern, and more specifically for the success of the implementation of the programme when finally introduced into the curriculum of Nigerian schools. In addition, this study would stimulate further related research work.
5. Conclusions
- This quasi-experimental study has shown that both sexes and age groups had positive attitude to bystander cardiopulmonary resuscitation (CPR). However, none showed statistically significant association to attitude towards bystander CPR. There is need to repeat the study with a larger sample size in different communities to confirm this findings or otherwise.
ACKNOWLEDGEMENTS
- The author(s) remain very indebted to Professor C O Onyeaso for his immense guidance and support throughout the period of this work.