-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2017; 7(2): 393-399
doi:10.5923/j.ajmms.20170712.02

Reproductive Performance in Women with Fibroid
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMomen A. M. Kamel, Ahmed M. A. Nasr, Kamal M. Zahran, Sohir A. M. Ibrahim
Obstetrics & Gynecology Department, Faculty of Medicine, Assiut University, Egypt
Correspondence to: Sohir A. M. Ibrahim, Obstetrics & Gynecology Department, Faculty of Medicine, Assiut University, Egypt.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Uterine fibroid is a common gynecological problem among women of reproductive age, and there are conflicting reports of its effect on fertility and pregnancy outcome. It is a common reason for gynecological consultation in most hospitals as well as the most common benign genital tract tumor which are associated with sub-fertility and early pregnancy loss in women of reproductive age. The study was conducted at Women's Health Hospital Assiut University. This study was divided two main groups: Group I: prospective study to assess the reproductive performance of infertile women with myoma after myomectomy. Group II: This cross sectional study to assess the prevalence of myoma in women came for delivery vaginal, cesarean section or abortion. Result shows Intraoperative findings of myomectomy in study group I (45.0% of cases have myoma size in range 5-10 cm, also 45.0% of myoma location was in lower uterine segment and 50.0% was Intramural type and the great majority of women had single fibroid about 76.5% of cases. About reproductive outcome with previous myomectomy after follow up. With (52.5%) of them still have infertility and (47.5%) become pregnancy. Which (42.1%) of them had abortion, (31.5%) were delivered C.S and (15.7%) delivered vaginally and (10.5%) were diagnosed as an ectopic pregnancy. Also, complications of myoma during pregnancy in study group II majority of cases has pain with fibroid during pregnancy about 66.67% of cases, (60.0%) of cases have bleeding during first trimester, (37.61%), (27.3%) malpresentation, also there were (28.57%) have Miscarriage and lowest percentage (2.38%) have placenta abruption and (2.38%) have post-partum hemorrhage. As regard there were (30.0%) of cases have no symptoms. There was higher percentage in myoma (50.47%) in age above 36 years. Higher percentage in myoma (51.42%) in primipara.
Keywords: Fibroid, Reproductive performance, Infertility, Myoma
Cite this paper: Momen A. M. Kamel, Ahmed M. A. Nasr, Kamal M. Zahran, Sohir A. M. Ibrahim, Reproductive Performance in Women with Fibroid, American Journal of Medicine and Medical Sciences, Vol. 7 No. 2, 2017, pp. 393-399. doi: 10.5923/j.ajmms.20170712.02.
Article Outline
1. Introduction
- Uterine fibroid is a common gynecological problem among women of reproductive age, and there are conflicting reports of its effect on fertility and pregnancy outcome. It is a common reason for gynecological consultation in most hospitals as well as the most common benign genital tract tumor which are associated with sub-fertility and early pregnancy loss in women of reproductive age [1].According to a 2010 World Health Organization report, fibroids affects between 20-25% of women, and close to 235 million women which represent 6.6% of global women population are estimated to have been affected worldwide [2].Studies have shown that women with myomas are more likely to present with abdominal mass and menorrhagia, and may also present with dyspareunia, dysmenorrhoea, abdominal discomfort or bloating, painful defecation, back ache, urinary frequency or retention, and infertility. During pregnancy, fibroids may be a cause of miscarriage, bleeding, abnormal lie and presentation [3].An association between myomas and fertility has been observed but the responsibility of fibroids in infertility remains unclear and debatable [4].Fibroids are more common in obese women Fibroids are dependent on estrogen and progesterone to grow and therefore relevant only during the reproductive years [5].Myomectomy is an alternative to hysterectomy for women who wish to retain their uterus, regardless of their fertility desire. Removal of fibroids should be considered if they are thought to be associated with heavy mentrual bleeding, pelvic pain and/or pressure symptoms, and in some cases reproductive issues [6].Risk of recurrence is associated with age, preoperative number of fibroids, uterine size, associated disease, and childbirth after myomectomy. Five years following laparoscopic myomectomy, the cumulative probability of recurrence (new or unremoved fibroids) in women who subsequently gave birth was 42%. In those who did not give birth, it was 55% [7].Uterine fibriod are heterogeneous tumors in composition, size, location, and number; variations in any of these factors could possibly alter the effect on a woman’s fertility status. Recommendations as to which infertile women with fibroids would benefit from myomectomy are varied, given the potential risks and sequelae of surgery. A number of studies have been performed to determine the influence of myoma on fertility, with widely disparate findings, and many of the studies suffer from methodologic flaws. The investigations are frequently poorly designed and often uncontrolled or historically controlled, analysis often lacks correction for important confounding variables, sample size is usually small, and conclusions are often provided that are unsupported by the data at hand [8].The relationship between fibroids and infertility has been elucidated through numerous studies on ART patients, which have been summarized in several meta-analyses and systematic reviews. Although abnormal gamete transfer and blockage of fallopian tubes are circumvented by assisted reproductive technologies (ART), fibroids may also compromise fertility by altering the endometrial receptivity, thus negatively affecting embryo implantation and lowering the chances for pregnancy [9].Fibroid location is of critical importance in ART outcomes. Submucosal fibroids, in particular, significantly reduce implantation and pregnancy rates of ART. Submucosal fibroids that distort the uterine cavity have been found to carry a relative risk of 0.3 for pregnancy and 0.28 for implantation after ART, when compared to infertile women without fibroids [10].Approximately 10% to 30% of women with uterine fibroids develop complications during pregnancy. However, these adverse pregnancy outcomes have been reported in incomplete settings with selection bias, small and differing populations, varying inclusion criteria, low occurrence of adverse outcomes, and inadequate confounding variables. As a result, these studies have reported inconsistent relationships between fibroids and adverse obstetric outcomes. Although decreased uterine distensibility or mechanical obstruction may explain some adverse outcomes, the precise mechanism by which uterine fibroids induce obstetric complications is not clear [11].
2. Patients and Methods
2.1. Settings
- The study conducted at Assiut University Women's Health Hospital.
2.2. Study Design
- This study was divided two main sections:§ Group I: prospective study to assess the reproductive performance of infertile women with myoma after myomectomy.§ Group II: assess the prevalence of myoma in women came for delivery vaginal or cesarean section or abortion.
2.3. Prospective Study
2.3.1. Subjects
- Women in reproductive period with history of infertility who underwent myomectomy.
2.3.2. Inclusion Criteria
- § 1ry or 2ry infertility aged (20-35) years.§ 2000 pregnant females admitted to Women’s Health Hospital for Caesarian section and vaginal delivery each of them 1000 cases and 300 cases of abortion which were admitted to the hospital and also accept to participate in our study.
2.3.3. Exclusion Criteria
- § Age less than 20years and more than 35 years old.§ Refuse to participate in the study.
2.3.4. Selection Criteria
- § Women in group I referred to our hospital from January 2014 till January 2015 for infertility problems with concurrent myoma and planned for myomectomy. Selected women have uterine myoma (intramural, sub serous or sub mucous) with absence of other causes of infertility. myomectomy was performed and follow up was carried out for one year after the operation to check reproductive outcome (abortion, pregnancy, infertility, recurrence of myoma).§ Women in group II Intraoperative findings of myoma (site, size, number, type) during caesarian birth and also from ultrasound screening for all post vaginal deliveries and post caesarian deliveries and post abortive patient for accidentally discovered myoma.
2.3.5. Follow up
- Ÿ Follow up for those patient in group I for 1year after myomectomy.Ÿ Follow up was done in 24 hours for all postpartum and post abortive patient in group II who accept to participate in our study for post-partum or post abortive complications.
2.3.6. Outcome
- § Primary outcome in group I: The pregnancy rate within one year after myomectomy.§ Secondary outcome in group I: The rate of abortion and recurrence of myoma persistence of pain and bleeding.§ Primary outcome in group II: to assess prevalence of myoma in cases of caesarean section and vaginal delivery and abortion.§ Secondary outcome in group II: To assess the size, site of the fibriod and the post abortive and postpartum complication, need for blood transfusion.
2.4. Statistical Methods of Data Analysis
- The collected data were coded, fed to computer, organized and statistically analyzed. Statistical analysis was done using computer programs: Microsoft excel version 16 and Statistical Package for Social Science (SPSS) for windows version 25.0 [12]. Qualitative (categorical) data were presented by frequency and percentage. Quantitative data were presented by mean ± SD.
3. Results
3.1. Section I: Prospective Study to Assess the Reproductive Performance of Infertile Women with Myoma after Myomectomy
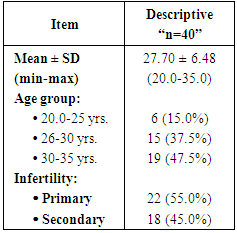
- Table (1) shows sociodemographic characteristics of the studied women. The mean value of age 27.70 years and (47.5%) of patients in age group 30-35 years. With (55.0%) of cases had primary infertility and (45.0%) with secondary infertility fibroid percentage (87.5%) have pelvic pain, (72.5%) have anemia, (27.5%) have miscarriage. As regard there were (45%) of patients have menorrhagia and (20.0%) needed to blood transfusion.
|
|
|
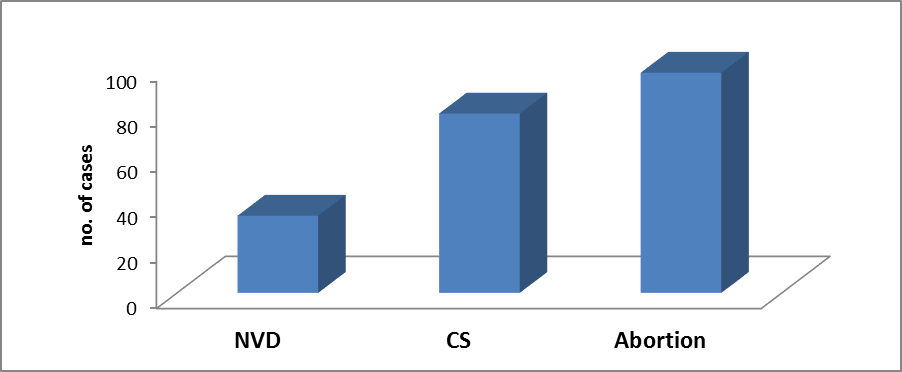
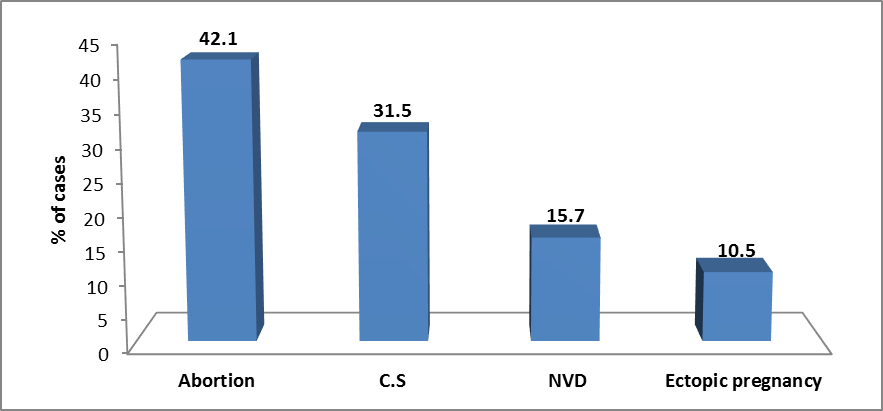 | Figure (1). Outcome of cases after pregnancy |
3.2. Section II: This cross Sectional Study Aimed to Assess the Prevalence of Myoma in Women Came for Delivery Vaginal or Cesarean Section or Abortion
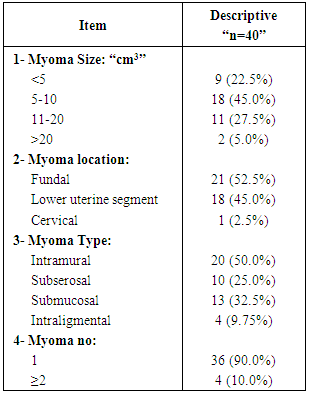
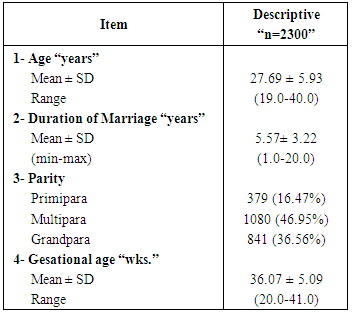
- Table (4) shows demographic data in study group. With mean age 27.69 years and mean of duration of marriage was 5.57 years, (46.95%) have multipara, (36.56%) grandpara and (16.47%) primipara and the mean gestational age was 36.07 weeks. Prevalence of myoma in study group were (9.13%) of cases.
|
 | Figure (2). Distribution of myoma in study group |
|
|
|
4. Discussion
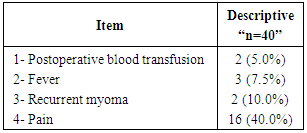
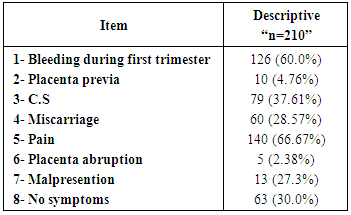
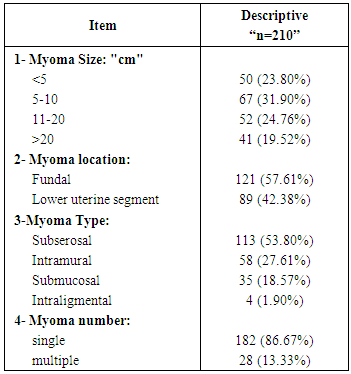
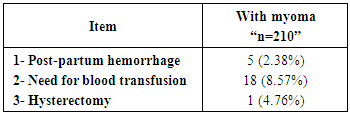
- Uterine fibroids are the most common tumors in women and are almost always benign. Moreover, they are highly dependent on the ovarian steroids. Although their cellular origin remains unknown, they are considered to be monoclonal tumors, arising from the mutation of a single myometrial somatic stem cell after multiple cycles of growth followed by involution under hormonal influence [13].The study conducted at Assiut University Women's Health Hospital. This study was divided two main sections.In present study there were mean value of age 27.70 years and (47.5%) of patients in age group 30-35years. This agree with Pritts et al. [14], they reported fibroid characteristics, factors that affect the reproductive outcome after myomectomy include age, duration of infertility, and presence of other infertility factors. Of these, age is the most important factor. Women’s fertility peaks at 20-24 years of age; fertility decreases as age increases. Fertility has an accelerated decline after age 37.However, fibroids are mostly present in women of reproductive age, and there is a higher prevalence of fibroids in women who are 30-40 years of age. Therefore, age is the critical determinant of reproductive outcome in women with fibroids [15].In present study there were reproductive outcome with previous myomectomy after follow up. With (37.55%) of them have infertility and (62.5%) become pregnancy which (56.0%) of them were abortion (28.0%) were delivered C.S and (8.0%) were normal vaginal delivery and (8.0%) were ectopic pregnancy. This agree with Shokeir et al. [16], they reported Overall, among patients with complete follow-up, a total of 93 (45.6%) pregnancies occurred 64 (63.4%) in the study group and 29 (28.2%) in the control.In present study there were Symptoms with previous myomectomy. With high percentage (87.5%) have pelvic pain, (72.5%) have aneamia, (27.5%) have pregnancy miscarriage. As regard there were (45%) of patients have menorrhagia and (20.0%) needed to blood transfusion. This agree with Lee et al. [11], they reported Spontaneous miscarriage rates are greatly increased in pregnant women with fibroids compared with control subjects without fibroids (14% vs 7.6%, respectively).In present study there were ultrasound of myoma in study group. With (45.0%) of cases have myoma size in range 5-10 cm3, (45.0%) myoma location in lower uterine segment and (50.0%) in Intramuraltype also there were (90.0%) of cases have one myoma. This agree with Marchionni et al. [17], they reported further investigated the possible impact of age (30 years), size of the largest fibroid (5 cm), location of the fibroid with respect to the uterine wall (intramural or subserous) and with respect to the uterine body (anterior, posterior, lateral, fundal). Also, Mettler et al. [18] reported were pelvic pain in 134 patients (68.7%), menorrhagia in 91 patients (46.6%).An association between myomas and fertility has been observed but the responsibility of fibroids in infertility remains unclear and debatable.at present, it is estimated that fibroids may be associated with infertility in 5 to 10% and are possibly the sole cause of infertility in 1 to 3%. The location of fibroids is implicated to play a role in infertility and miscarriages, with intramural and submucous locations identified as major risk. Sub mucous fibroids are believed to interfere with the function of the uterine lining and the ability of a fertilized ovum to implant. It is also postulated that larger fibroids may distort or block the fallopian tubes [4].In present study there were (5.0%) of patients need blood transfusion, also (7.5%) of patients have fever, (10.0%) of patients have recurrent myoma and (40.0%) of patients have pain. This agree with Mettler et al. [19], they reported that complications can arise from the location of the fibroids. These complications range from intermittent bleedings to continuous bleeding over weeks, from single pain episodes to severe menorrhagia and chronic abdominal pain with intermittent spasms, from dysuria and constipation to chronic bladder and bowel spasms and even to peritonitis. Infertility may be the result of continuous metro and menorrhagia, leading to chronic infection and uterine spasms up to non-implantation. Possible complications resulting from treatment of these disorders are haemorrhages, infection, adhesions, and secondary pain resulting from the treatment efforts.Abnormal uterine bleeding in the form of menorrhagia- seen in 95.7% of the participants in this study is a common clinical presentation in women with uterine fibroids. Menorrhagia in severe cases may result in anemia, which was noted in 32.9% of participant- consistent with the findings of other researchers [20].In present study there were reproductive outcome with previous myomectomy after follow up. With (37.55%) of them have infertility and (62.5%) become pregnancy which (28.0%) of them were abortion (56.0%) were delivered C.S and (8.0%) were normal vaginal delivery and (8.0%) were ectopic pregnancy. This agree with Desai and Patel [21], they reported approximately 50% of the women with infertility and myomas become pregnant after myomectomy. As epidemiological studies have not been able to provide unflinching evidence of the impact of fibroids on fertility, a large number of studies have been based on pregnancy rates after myomectomy.Varasteh et al. [22] reported a correlation of 65.2% between myomectomy and the accumulated rate of pregnancies.In present study prevalence of myoma in study group II were (9.13%) of cases. This agree with Olotu et al. [23], they reported Fibroid has been accounted for 7.4% of that studied population [20]. As regard Ekine et al. [24] reported Uterine fibroids are commoner among Black women than Caucasians, the incidence in Nigeria ranges from 17.9- 26%, as against 5-11% reported in Europe and United States.In present study the percentage incidence of fibroid tumours was 1.9, 47.61 and 50.47 for the three groups 16-25, 26-35 and ≥36 yrs, respectively. This agree with Olotu et al. [23], they reported the percentage occurrence for ages 16-25 yrs (3.5%), 26-35 yrs (51.9%) and 36-45 yrs (44.6%) has been put at 20–25% among white women [25].In present study there were significance difference between myoma and parity (P<0.05) which higher percentage in myoma (51.42%) in primipara. This agree with Ezeama et al. [2], they reported Uterine fibroids are reportedly commoner amongst young nulliparous women within the reproductive age of 15-49 years- consistent with the findings from this study, where over one-third of the participants were nulliparous and over 3/4 were within the reproductive age group of 31-40 years. “It is generally believed that most uteruses that fails to carry a baby, is bound to harbor fibroids”. This may be due to the prolonged effect of estrogen on the uterine smooth muscle [26].In present study there were shows complication of myoma during pregnancy in study group. With (66.67%) of cases have pain, (60.0%) of cases have bleeding during first trimester, (37.61%), (27.3%) malpresention and lowest percentage (2.38%) have placenta abruption and (2.38%) have post-partum hemorrhage. This agree with Lee et al. [11], they reported Approximately 10% to 30% of women with fibroids develop complications during pregnancy, although these adverse pregnancy outcomes have been reported in incomplete settings with selection bias, small and differing populations, varying inclusion criteria, low occurrence of adverse outcomes, and inadequate confounding variables.In early pregnancy, spontaneous miscarriage rates are greatly increased in pregnant women with fibroids compared with those without fibroids (14% vs 7.6%, respectively), and bleeding is significantly more common if the placenta implants close to the fibroid. In late pregnancy, such complications include preterm labor, placental abruption, placenta previa, and fetal anomalies [27].Also, Legendre et al. [4] reported women with fibroids have uneventful pregnancies, the weight of evidence in the literature suggests that uterine fibroids are associated with an increased rate of spontaneous miscarriage, preterm labor, placenta abruption, malpresentation, labor dystocia, cesarean delivery, and postpartum hemorrhage. Pain is the most common complication of fibroids during pregnancy. The symptoms can usually be controlled by conservative treatment, but may require definitive surgical resection in rare instances. Some women with a previous myomectomy may need to be delivered by elective cesarean delivery prior to the onset of labor, particularly if the uterine cavity was entered.Pain is the most common complication of fibroids during pregnancy. The symptoms can usually be controlled by conservative treatment (bed rest, hydration, and analgesics), but may require definitive surgical resection in rare instances [21].The symptoms can usually be controlled by conservative treatment, but may require definitive surgical resection in rare instances.In present study there were characteristics of myoma in study group. With (31.90%) of cases have myoma size in range 5-10 cm3, (41.42%) myoma location in lower uterine segment and (53.8%) in type 0 also there were (86.67%) of cases have one myoma. This agrees with Shokeir et al. [16], they reported sub mucous myoma type in relation to pregnancy rate has been evaluated.Among the patients who underwent myomectomy, the pregnancy rates obtained were 43.3% in cases of submucosal, 56.5% in cases of intramural, 40.0% in cases of submucosal–intramural and 35.5% in cases of intramural–sub serosal uterine fibroids, respectively. Among the patients who did not undergo surgical treatment, the pregnancy rates obtained were 27.2% in women with submucosal, 41.0% in women with intramural, 15.0% in women with submucosal–intramural and 21.43% in women with intramural– sub serosal uterine fibroids, respectively. Although the results were not statistically significant [28].Actually, the interpretation of these data concerning the sub mucous myoma type in relation to pregnancy rate is difficult. The difference cannot be due simply to uterine cavity abnormality [11].
5. Conclusions
- Uterine fibroids are common among young nulliparous women in group I within the reproductive age of 15-49 years. which has been implicated as a cause of infertility. Women in the study group showed a better possibility of becoming pregnant after myomectomy. in our study, 47.5% of women achieved pregnancy during one year of follow up after myomectomy.The great majority of women in group II of with fibroids develop complications during pregnancy. In early pregnancy, bleeding in early pregnancy (60%) is most common complications, followed by miscarriage and pain. In late pregnancy, other complications as preterm labor, placental abruption, placenta previa, Pain also is the most common complication of fibroids.
6. Limitation of Study
- Ÿ Missed in many cases in follow up after myomectomy.Ÿ Refuse some of patients to contact in study.
7. Future Research
- Need to further more study with large sample and continue follow up to study effect of myomectomy in reproductive health “pregnancy, abortion”.