A. D. Fayazov, D. B. Tulyaganov, U. R. Kamilov, R. S. Ajiniyazov, D. A. Ruzimuratov
Republican Research Center of Emergency Medicine, Tashkent, Uzbekistan
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The authors studied the structure and results of electric trauma treatment in 556 patients. The obtained data testify the tendency to the growth of electric burns in children and young aged able-bodied people. The study of surgical treatment results in patients with such injuries shows the necessity of a wider use of the active surgical tactics.
Keywords:
Electric trauma, Surgical treatment, Decompressive fasciotomy, Necrectomy, Osteonecrectomy, Auto-dermoplasty, Roentgen densitometric
Cite this paper: A. D. Fayazov, D. B. Tulyaganov, U. R. Kamilov, R. S. Ajiniyazov, D. A. Ruzimuratov, The Structure and Peculiarities of Surgical Treatment Tactics of the Deep Electric Burns, American Journal of Medicine and Medical Sciences, Vol. 7 No. 8, 2017, pp. 323-326. doi: 10.5923/j.ajmms.20170708.04.
1. Introduction
Electric current impacts on the victim’s organism through two pathogenic mechanisms: 1) reflex action through the nervous system leading to blood circulation and respiration disorders; 2) the direct effect of thermal, electrochemical and electrodynamic factors. The first factor evaluates a severity of body’s general reaction and is a leading one in the development of the lethal outcome which occurs due to heart ventricles fibrillation, respiratory paralysis, glottis shock, and spasm; the second-factor impacts on the intensity of the local changes [1, 3, 5].The severity of the electric injury depends on the current physical parameters and the peculiarities of the environment. Low voltage current (127-220 V) is more dangerous than a high voltage one because it frequently causes heart ventricles fibrillation. A high air humidity promotes the occurrence of arc contact which is formed at the voltage of more than 1000 V. The last type of injury should be classified as thermal but not an electrical injury [2, 4].Currently, electrical burns do not exceed 2-3%, but they often become the reason of disability, and in some cases, they lead to the death, that is why they can be put on the first places by their significance [3, 6].
2. Object
To analyze the structure, results, and peculiarities of surgical treatment in patients with electrical injuries.
3. Materials and Methods
556 patients with electrical injuries at the age from 6 months to 80 years we admitted to the department of combustiology of the Republican Research Centre of Emergency Medicine (RRCEM) from 2005 to 2016. The structure and the frequency of electrical injuries, the dynamics of clinical-laboratory rates and clinical-instrumental investigations were analyzed. Besides, the study of surgical treatment results subject to the severity of injury was carried out. All victims have performed the following investigations by the indication: X-ray, echoencephalography, electrocardiography, ultrasound investigation, diagnostic fiber-optic bronchoscopy, EFGDS, microbiologic investigations of sputum, burn wound and blood. All patients received a standard drug therapy the scope of which was depended on the condition severity, time of admission, the period of burn disease and the presence of complications. 33 (5.6%) patients with osteonecrosis of calvarium bones of postelectrotraumatic genesis were separated to a special group. X-ray densitometry method which allows to estimate the level of mineralization of affected bone after burn injury and to evaluate the rate of osseous tissue regeneration was used in those patients. Statistical results manipulation has been done with the help of variational statistics standard method. Statistical indices were calculated with the use of Microsoft Excel 2007.
4. Results and Discussion
The structure of burn injuries has been significantly changed in recent years: specific density of electrical injuries has been increased from 2.7% to 8% for the last 10 years [1, 3]. The study of RRCEM showed the tendency to the growth of electrical burn injuries (Fig.1).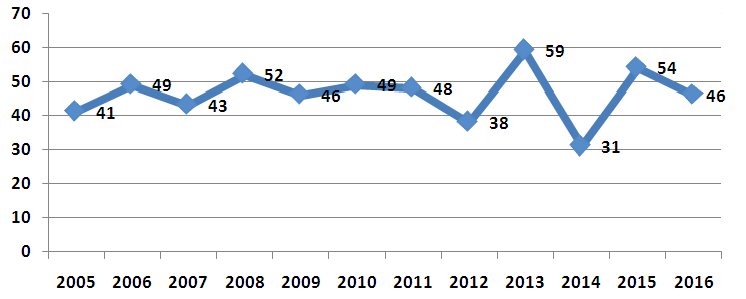 | Figure 1. The dynamics of electrical injuries |
The mean age of patients made up 17.5±16.2 years (from 6 months to 80 years). Men were 427 (76.8%), women – 129 (23.2%).Electrical injuries often occur in children and teenagers who have no enough knowledge about the danger of the current. Young age and non-disabled people in whom thermal-electric burns occur with the same frequency both at home and at work - they are also in the risk group. As it is shown in Fig.2, the biggest part of victims – 289 (52%) are the children at the age from 6 months to 18 years. The quantity of young aged non-disabled patients from 19 to 60 years made up 264 (47.5%).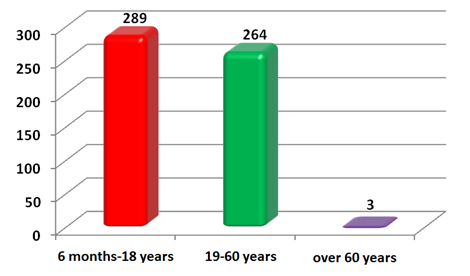 | Figure 2. The structure of victims with thermal-electric burns by age |
One of the typical peculiarities at thermal-electric injuries is a limitation of lesion area. Only in 48 (8.7%) patients, the total area of thermal lesion exceeded 10% of body surface. 128 (23%) patients had the lesion from 1 to 3% of body surface, in 150 (26.9%) cases – 4-10%. The rest 230 (41.4%) were the victims with the burns less than 1% of body surface – «electric marks» (Fig.3).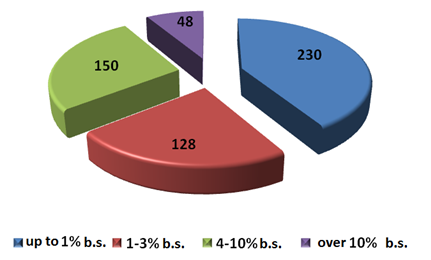 | Figure 3. Randomizing of patients by thermal-electric burn area |
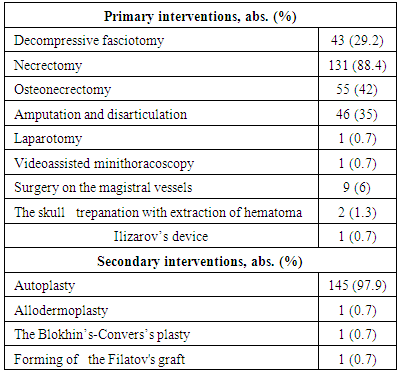
148 (26.6%) patients with deep burns were undergone an operative intervention. We followed the principles of active surgical tactics at performing operative treatment (Table 1). 43 (29.2%) victims were operated during the first 24 hours after injury – they were performed decompressive fasciotomy on the extremities. It allowed preventing the development of secondary changes due to subfascial edema. The indications to fasciotomy were: enlargement of extremity segment in the volume; absence or weakening of magistral vessels pulsation; the changes of color of extremity segment cutaneous covering (paleness, cyanosis, cutis marmorata); reduction or absence of a tactile or pain sensitivity. Any suspicion of the injury of magistral vessels is also an indication for performing decompressive surgery up to the proximal level of tissues necrosis. A compulsory condition at performing fasciotomy is a dissection of fascia above each muscles group. Table 1. The types of surgical interventions in patients with electric burns (n=148)
 |
| |
|
Necrectomy in the early period after the injury was carried out in 131 (88.4%) patients. In 55 (42%) operated cases it was completed by osteonecrectomy. In 6 patients after necrectomy on the extensive areas in the postoperative period, we used temporary wound coverings for the preparation of the wounds to plastic closing (xenoskin, pholiderm, voscopran, parapran). Amputation and disarticulation of extremity segments was carried out in 46 (35%) victims. Indications for such surgeries were the total lesions of soft tissues with the development of extremity functional unfitness. The typical feature of the thermal-electric burns due to high-voltage current is a relatively high quantity of combined and associated lesions the occurrence of which is depended from the transformation of electric energy to the other types of energy (mechanical, thermal, chemical). In 14 (9.5%) cases from total quantity of operated patients the interventions were performed due to the combined injuries: 1 patients were undergone laparotomy and closure of liver rupture; in 1 case we performed videassisted minithoracoscopy from the left, elimination of clotted hemothorax, sanation, and drainage of the left pleural cavity; in 9 cases – interventions on the magistral vessels; 2 patients were carried out the skull trepanation with extraction of hematoma; in 1 patient – Ilizarov’s device on the lower extremity. Plastic recovery of a cutaneous covering integrity is a final stage of the operative treatment in patients with thermal-electric injuries. From the total quantity of operated patients in 145 cases after forming of a granulation tissue we were performed autoplasty by split grafts, and in 1 case the surgery was completed by Allo-dermoplasty. 2 patients who were operated with the participation of a micro-surgeon were performed the Blokhin’s-Convers’s plastic and forming of the Filatov's graft. One of the most complicated forms of thermal-electric injuries is osteonecrosis of calvarium bones which was observed in 33 (5.9%) patients. In several areas of osteonecrosis, we carried out X-ray densitometry with the aim of osteonecrosis area definition. X-ray densitometry investigations show that bones mineralization which in the necrosis area is practically absent. The rate of osseous tissue regeneration was also estimated after its active stimulation by bone cutters. In the area of osteonecrosis the density of the osseous tissue was lower than the norm (0.61±0.04 arbitrary unit) in 3 times (0.22±0.03 arbitrary unit). However, in the area with bone cutter, those indices were 0.43±0.04. It testified the presence of regenerative process after application of perforated holes. At the traditional management of such type of patients, surgeries are performed in a month or later after trauma. The interventions consist of several stages with further waiting for natural, spontaneous rejection of metaphyseal osteonecrotic tissues and posterior covering of these areas with granulation. At such surgical treatment tactics, the process of wounds cleansing is delayed for several months. In contrast to the traditional method, we used active surgical tactics in these type of victims which was consisted in the early radical osteonecrotic subject to the X-ray densitometry results. 26 (78.8%) patients were intraoperatively determined a thermal lesion of an only external plate of the osseous tissue; in 7 (21.2%) cases – the lesion of the whole depth of the bone plate. The extension of necrosis on the brain tunic and substance was not registered. 24 (72.7%) patients had a limited lesion of osseous tissue (up to 1/3 of calvarium area) and they were performed radical single-stage osteonecrectomy. In 6 (18.2%) cases the area of osteonecrosis was estimated as extended and (more than1/3 of calvarium area) and those patients were undergone two and more staged operations. Only 3 (9.1%) patients had insignificant area of lesion. Some technical methods are promoting accelerated cleansing of wounds after osteonecrectomy were used in the management of such type of patients. As it was mentioned above, at the lesion up to 1/3 of calvarium area we used an early single-stage osteonecrectomy and the holes were applied closer to each other (0.1-0.5 cm). In patients with extended osteonecrosis (more than1/3 of calvarium area) bone cutters were applied in different depth. At the lesion of the only external bone plate, the bottom of bone cutter reached up to the spongy substance of the bone structure. Bone cutters were applied up to pachymeninx at the death of the whole bone thickness. 7-8 days after application of the bone cutters we observed the growth of granulation. Non-rejected bone bridges and areas of the total lesion of bone structure between cutters holes are removed by the mechanical way without any technical difficulties and significant bleeding. It leads to the accelerated preparation of wound surface to the plastic closing by free Autoplasty with split grafts. Such method allows reducing treatment period to 1-1.5 month in patients with calvarium osteonecrosis.
5. Conclusions
1. Thermal-electric burns are often followed by deep lesions of soft tissues and osseous structures. The main contingent of patients are the children, the young and non-disabled people. 2. Surgical treatment results of such patients testify a necessity of a wider use of active surgical tactics. Early operative interventions at calvarium osteonecrosis with the use of X-ray densitometry help to improve surgical treatment results, to reduce a hospital staying of patients with thermal-electric burns.
References
| [1] | Alekseev A.A., Malyutina Yu.I., Tyurnikov Yu.I. Active surgical treatment methods of deep burns in old-aged patients //Ann.surg. - 2002. - №4. - p. 58-62. |
| [2] | Zinatulin R.M., Funufin C.N. Treatment tactics of calvarium necrosis at thermal injury //Abstracts book of the 1st Congress of combustiologists of Russia. - М., 2005. – p. 164-165. |
| [3] | Paramonov B.A., Porembskiy Ya.O, Yablonskiy V.G. Burns: Handbook. St-Petersburg, 2000. - p. 64-65. |
| [4] | Fistal E.Ya., Lishenko E.A. The plasty of calvarium defects with bones uncovering by local tissues // Trauma – 2001. – V. 2. - p. 179-184. |
| [5] | Bakkali H., Ababou K., Bellamari H., Ennouhi A., Nassim sabah T., Achbouk A., Moussaoui A., Fouadi F.Z., Siah S., Ihrai H. La prise en charge des brulures electriques: a propos ge 30 cas //Ann. Burns Fire Dis. - 2009. - Vol.22. №1. - P. 33-36. |
| [6] | Buja Z., Arifi H, Hoxha E. Electrical burn injuries. An eight – year review //Ann. Burns Fire Dis. - 2010. - Vol.23, №1. - P. 4-7. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML