-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2017; 7(4): 179-185
doi:10.5923/j.ajmms.20170704.04

Destructive Cholecystitis: Peculiarities of Gallbladder Structure on the Light and Scanning Electron Microscopy
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLB. A. Magrupov1, T. A. Vervekina2, V. U. Ubaydullaeva2
1Tashkent Medical Academy, Uzbekistan
2Republican Research Centre of Emergency Medicine, Uzbekistan
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The investigation results of gallbladder on the light and scanning microscope at calculous cholecystitis were presented in the article. The light microscopy revealed that the rate of changes in the gallbladder wall varied not only subject to the inflammation type but subject to anatomic part of organ (bottom, body, neck). Investigation by scanning microscope helped to specify and to demonstrate the results of light optic research visually.
Keywords: Cholelithiasis,Calculous cholecystitis, Electron microscopy
Cite this paper: B. A. Magrupov, T. A. Vervekina, V. U. Ubaydullaeva, Destructive Cholecystitis: Peculiarities of Gallbladder Structure on the Light and Scanning Electron Microscopy, American Journal of Medicine and Medical Sciences, Vol. 7 No. 4, 2017, pp. 179-185. doi: 10.5923/j.ajmms.20170704.04.
1. Introduction
- The issue of modern diagnostics and treatment of cholelithiasis, its numerous and severe complications still is not finally solved and attracts attention of the wide circle of the researchers and practitioners [1-16].A large quantity of researches is devoted to the issues of pathogenesis, diagnostics and treatments of the biliary tracts diseases. Classical investigations were finished at the beginning of the 20th century. But this issue still remains actual as well. The conducted analysis of available literature has shown that numerous works of both domestic [1-4, 6, 10, 14, 16] and foreign [5, 7, 9, 11, 13, 15] authors are devoted to the study of cholelithiasis. Those investigations were mainly devoted to the study of pathogenesis and classification of cholelithiasis, to working-out of new methods for conservative and surgical treatment of this pathology. Pathologic anatomy of the cholelithiasis is closely connected with formation and growth of gallstone, its migration, obstruction of bile ducts lumen and the development of these phenomena outcome: atrophy and flatness of mucous membrane, sclerosis of subjacent layers, certain atrophy of gallbladder. Such changes can be coursed without inflammation, but in majority of cases the cholelithiasis is developed and it is connected with bile properties abnormality, edema of mucous membrane, occlusion of lymphatic and venous vessels promoting the development of inflammatory process. Pathomorphology at acute lesion of the gallbladder and bile ducts, and it has wide range of changes. They can be destructive and nondestructive [21-22].Subject to clinical manifestations and pathomorphologic changes in the gallbladder, independently from the etiology, they differentiate acute and chronic cholecystitis. This division is conditional, because there are interjacent forms of the disease – chronic recurrent cholecystitis. Severity rate of acute cholecystitis can be different – from catarrhal inflammation to the gallbladder gangrene [23]. The issues of morphologic changes estimation in gallbladder at different rate of bile-excreting tracts obstruction still remain unsolved. While studying recent decades literature we did not find fundamental works devoted to the morphologic and morphometric features of gallbladder at cholelithiasis. There are also no studies devoted to the comparison of the results of light optic and electron scanning investigations of the gallbladder.
2. Materials and Methods
- The research was carried out on bioptic material of the Republican Research Centre of Emergency Medicine. We investigated gallbladders of 357 patients undergone surgeries subject to destructive cholecystitis (DCh). The gallbladders taken at autopsy of the patients died from the pathology which was not related to hepatobiliary system (n=45) were investigated as a control group (CG). The shards of gallbladder tissue from bottom, body and neck, 1х1 cm in size were cut for microscopic investigation. Material was fixed in 10% neutral formaldehyde solution and conducted through alcohol of increasing concentration and was poured into paraffin by the method of Lloyd Z. et al. [17]. Sections (4-5 µm thick) were stained by hematoxylin and eosin. At performing light optic microscopy there was detected a heterogeneity of the gallbladder wall changes and 2 groups of observations were separated: acute phlegmonous cholecystitis (APCh) – (n=237) and acute gangrenous cholecystitis (AGCh)) – (n=120). For study the biological objects on the scanning electron microscope, tissue samples after fixation in 1% glutaraldehyde and additional fixation in 1% solution of OsO4 were conducted through aqueous solution of acetone of increasing concentration (up to 100%). Then the samples were conducted through the series of amyl acetate-ethanol mixtures of increasing concentration (up to 100%) [18-20]. The dehydrated samples were dried by the transition of the critical point and were covered by platinum in the “Joel” chamber. Axioskop 40 plus light optic microscope by “Carl Zeiss” and JSM-6010LV/6010LA scanning microscope by “Jeоl” were used for microscopy.
3. Results
- Numerous microscopic investigations showed that gallbladder wall had specific morphologic picture subject to not only the inflammation form, but also subject to the zone of investigation. It was revealed in the control group that in the area of the bottom a mucous membrane formed an abundance of high and narrow folds which were adjoined closely to each other (Fig.1 а). The height of the folds was preserved in the zones of the body and the neck, but their quantity was decreased per unit area (Fif.1 b,c). A muscular tunic of gallbladder was formed by longitudinal and transversal muscle fibers. Maximal thickness of the muscular tunic was defined in the body area, but at the neck and the bottom area that tunic was manifested insignificantly (Fig. 1). Inflammatory infiltration in gallbladder wall of that group was insignificant, with a predominance of mononuclear cells in all layers of the wall: by their maximal quantity in the bottom area and a sharp decrease in the areas of gallbladder body and neck.
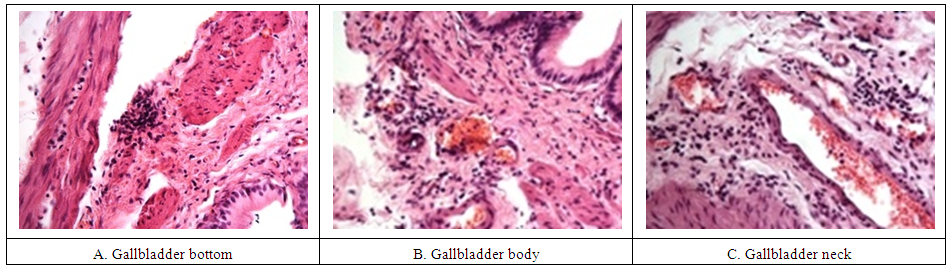 | Figure 1. Gallbladder of the control group at the light microscopy. Stained by hematoxylin and eosin, х40 |
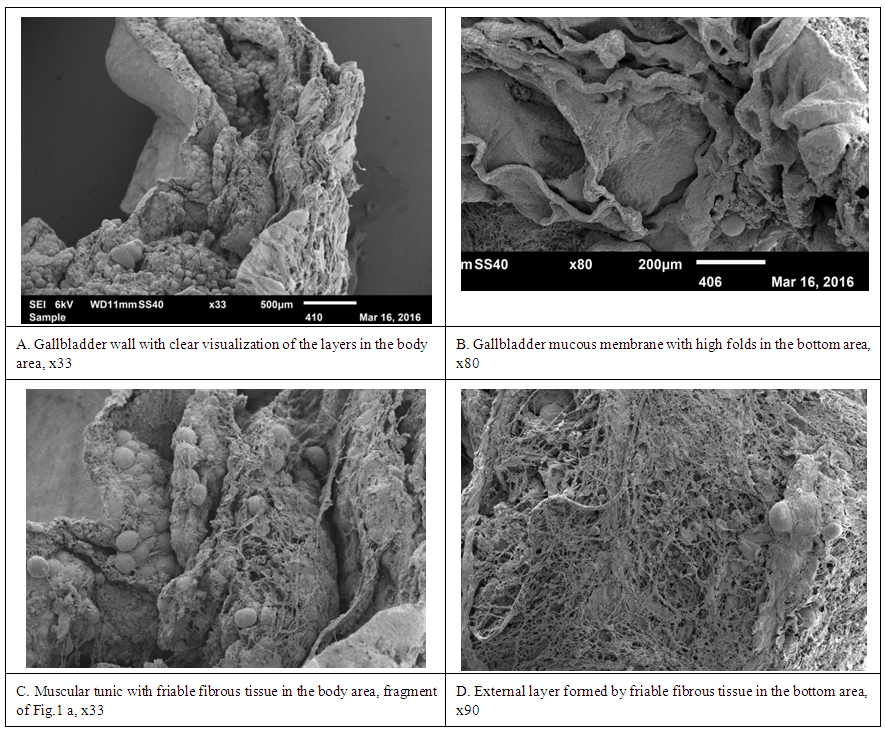 | Figure 2. Gallbladder of the control group at SEM |
 | Figure 3. Gallbladder at acute phlegmonous inflammation. The light microscopy. Stained by hematoxylin and eosin |
 | Figure 4. Gallbladder at phlegmonous inflammation. SEM |
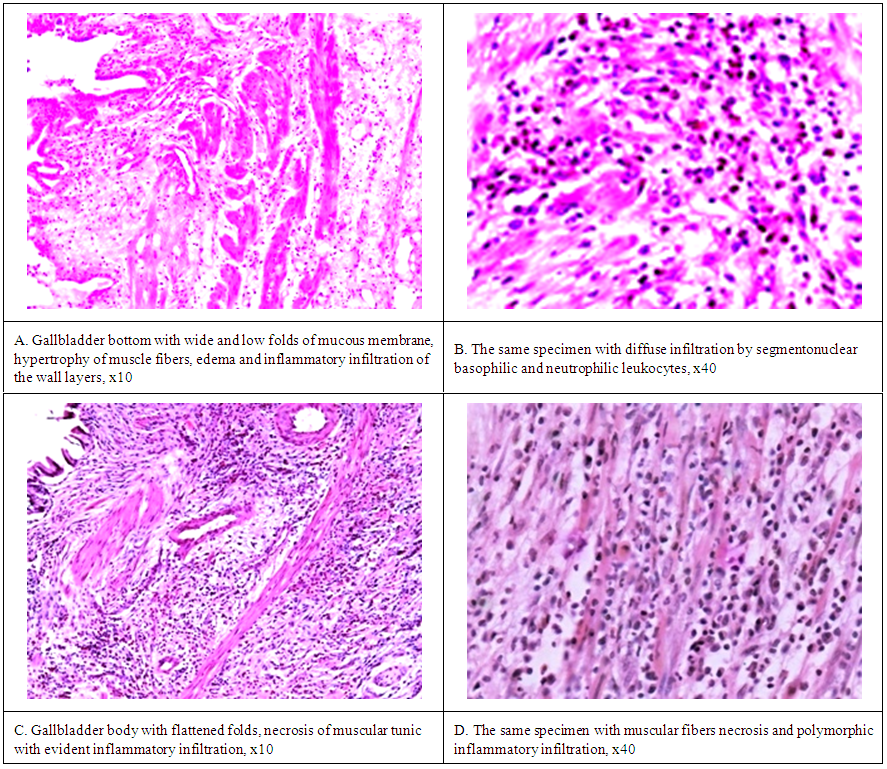
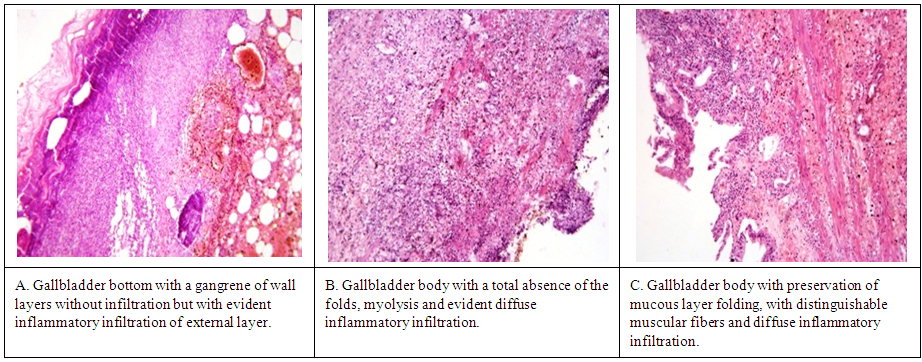 | Figure 5. Gallbladder at gangrenous cholecystitis. The light microscopy. Stained by hematoxylin and eosin, х10 |
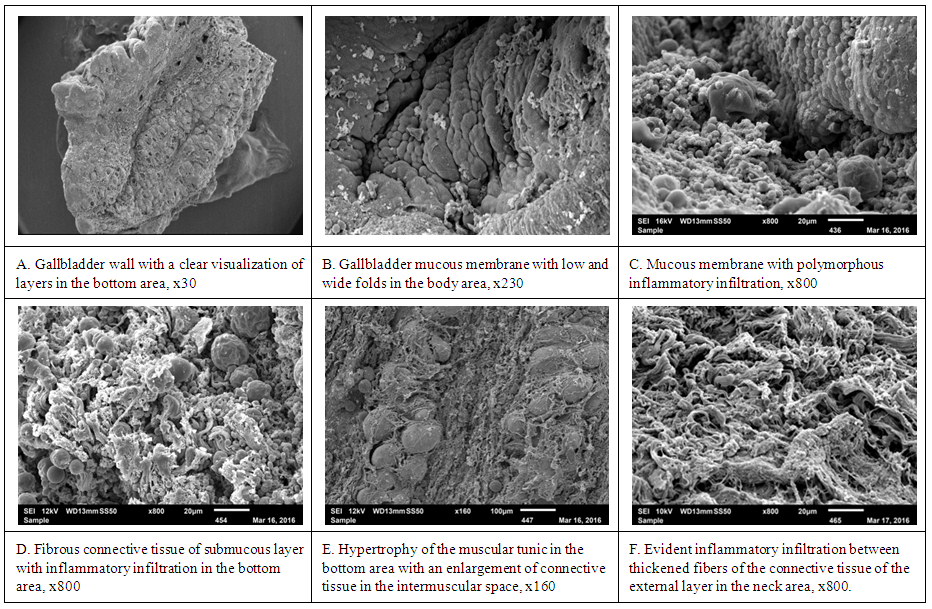
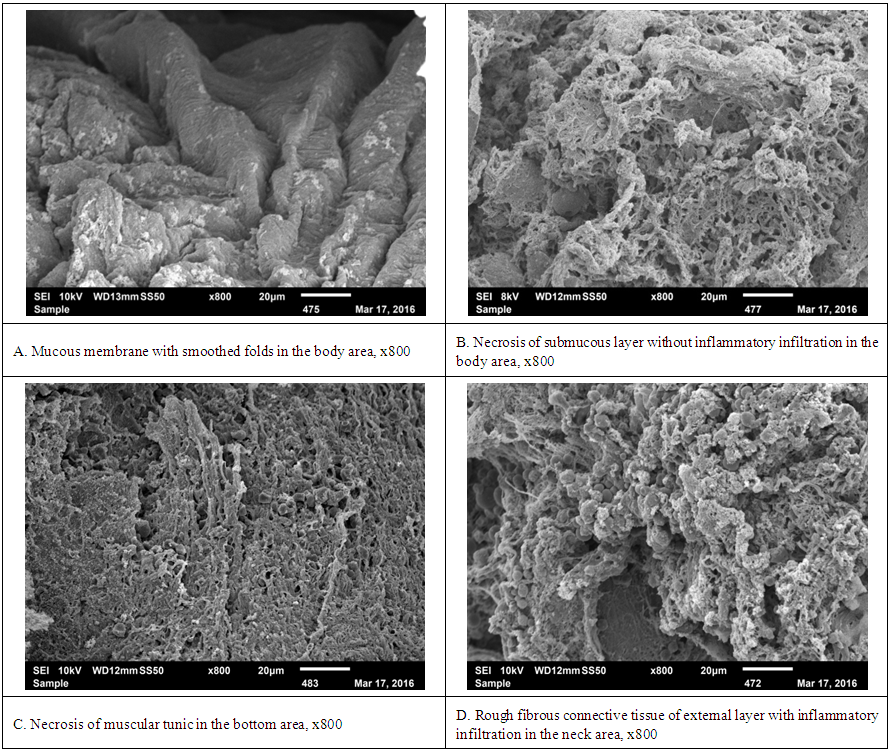 | Figure 6. Gallbladder at gangrenous cholecystitis. SEM |
4. Conclusions
- 1. The light microscopy has been remaining a basic type of investigation for diagnostics of morphologic forms of gallbladder inflammation at calculous cholecystitis in operated patients. 2. The research revealed that changes were variable subject to the areas of investigation at destructive forms of calculous cholecystitis. APhCh is specified by manifested changes in the body area, at AGCh – in the bottom area and gallbladder neck remains safer at such types of cholecystitis.3. Scanning electron microscopy being the next level of investigation gives essential information for understanding and deep analysis of tissue structural changes in different areas of gallbladder. 4. At scanning microscopy of phlegmonous-changed gallbladder there was a hypertrophy of gallbladder wall, an excrescence of connective tissue to submucous layer, sharp hypertrophy of myocytes with myolysis nidus and excrescence of rough connective tissue fibers in interstitial tissue, massive polymorphous inflammatory infiltration. At gangrenous cholecystitis there were detected smoothed relief, tissue necrosis without inflammatory infiltration. Inflammation cells were detected only in adventitia. 5. Light electronic microscopy shows the changes of layers patterns at different forms of inflammation and it is the source of demonstrable material of various structural elements correlation between each other.
5. Discussions
- Available researches devoted to the morphologic study of the gallbladder were carried out in the middle of the last century, without clear morphologic characteristics of the changes subject to anatomic part of the gallbladder. We have not also found studies which were devoted to the comparison of the gallbladder changes at the light and scanning electronic microscopy. Exactly these facts were a starting point for this research.