-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2017; 7(3): 151-155
doi:10.5923/j.ajmms.20170703.08

Are We Ordering Tumor Markers Appropriately?
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLK. Deasy1, S. Saadi1, F. Ashraf1, W. Chin1, J. Gilmore2, R. Griffiths1, 2, E. Ahmed1, 2
1The Clatterbridge Cancer Centre is an NHS Foundation Trust, United Kingdom
2Wirral University Teaching Hospital NHS Foundation Trust is an NHS Foundation Trust (WUTH), United Kingdom
Correspondence to: E. Ahmed, The Clatterbridge Cancer Centre is an NHS Foundation Trust, United Kingdom.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Serum Tumor Markers (TM) have limited role in screening, diagnosis and management of malignancy and there are international guidelines on the use of TMs. However, increasing TM orders are made in clinical practice with evidence to suggest misuse of TMs for indications not supported by guidelines. The inappropriate use of TMs not only results in waste of resources but can also generate anxiety and distress in patients. We audited the appropriateness of commonly used serum TM requests in a large acute teaching hospital and analyzed the cost implications of inappropriate use of TMs. Methods: We audited serum TM orders from the 1st to 31st of January 2010 in our hospital. Data was extracted from the clinical notes on the type of TMs requested and the reason/indication for the request and final diagnosis. Requests were judged appropriate or inappropriate based on the published guidelines on indication for the TMs. Using the tariff for individual TMs during the audit period, we analyzed the cost implication of inappropriate requests. Results: 131 TM orders were audited and 104 (79%) of these orders were judged inappropriate. Furthermore, 12 patients with the inappropriate orders who had abnormal TM result went on to have additional tests including 4 endoscopies and 5 CT scans. Based on the tariff for the TMs in the audit period, we estimated that £1107 was wasted due to the inappropriate orders of TMs alone during the audit period. Conclusion: Rationalizing the use of TMs in clinical practice can deliver substantial savings. Education and training for the clinicians is needed to raise awareness of the guidelines on appropriate use of TMs and change clinical practice.
Keywords: Tumor markers, Malignancy, Guidelines
Cite this paper: K. Deasy, S. Saadi, F. Ashraf, W. Chin, J. Gilmore, R. Griffiths, E. Ahmed, Are We Ordering Tumor Markers Appropriately?, American Journal of Medicine and Medical Sciences, Vol. 7 No. 3, 2017, pp. 151-155. doi: 10.5923/j.ajmms.20170703.08.
Article Outline
1. Introduction
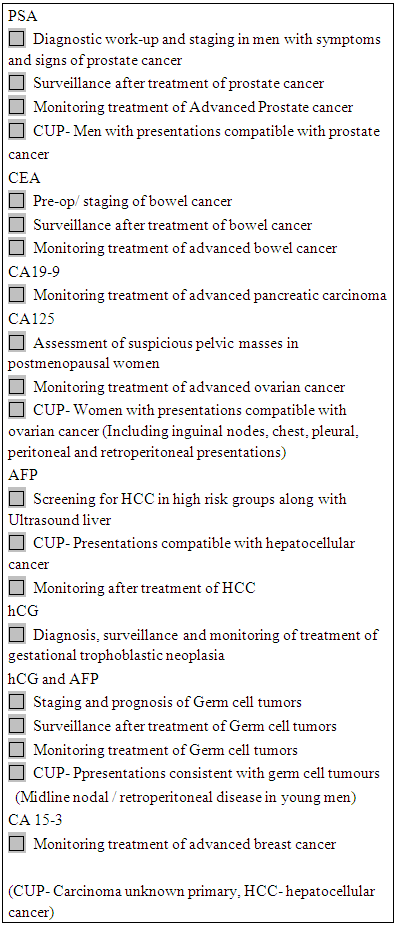
- The tumor marker (TM) can be defined as any molecule or substance produced by the tumor or the host tissue in response to the tumor that can be detected by an assay in body fluids or tissues. [1] TMs, if used appropriately could be valuable in the management of malignant diseases. Serum TMs such as AFP and HCG and PSA are extremely useful in the management of germ cell tumors and prostate cancer, respectively. Similarly, the tissue markers such Estrogen receptor and human epidermal growth factor receptor (HER)-2 have contributed enormously to tailoring treatment of breast cancer. The audit and the discussion here is restricted to commonly used serum TMs.The major limitation of the commonly used TMs is the lack of high specificity and sensitivity. Most of these TMs are not specific for one malignancy and are elevated in many non-malignant conditions. Therefore, the utility of TMs in screening, diagnosis and treatment is limited. Given these limitations, when is a TM request considered appropriate? The American Society of Clinical Oncology, [2] The National Academy of Clinical Biochemistry [3] and the European Group on Tumor Markers [4] have published guidelines on the use of TMs. Several conclusions can be drawn from these guidelines. Firstly, TMs should not be used for routine population-based screening for cancer. Secondly, some TMs could be used as an aid in diagnosis of selected cancers in conjunction with clinical examination and imaging. Thirdly, the main role of TMs is in surveillance and monitoring and finally, requesting a panel or panels of TMs, PSA in women and CA125 and C153 in men are inappropriate. Based on these guidelines on which there is a broad agreement on TM use, the indications for the common TMs are summarized in appendix 1. We audited the appropriateness of TM orders and the financial impact of inappropriate use of the TM orders in our hospital.
2. Aims of the Audit
- 1. To assess the appropriateness of TM requests2. To assess the financial impact of inappropriate use of TMs
3. Methods
- List of TM orders from 1st January 2010 to 31st January 2010 was extracted from the biochemistry laboratory data base in our hospital. We excluded requests from primary care, orders for HCG from emergency rooms and obstetrics in assessment of women with pregnancy related presentations, duplicate requests and cases where no data could be retrieved. We compiled a list of approved indications for each TM based on the international guidelines on TMs. We judged each order as appropriate or inappropriate based on the approved indications for TMs as per the guidelines.Patient notes were reviewed and data was collected on a) reason/indication for the orders b) pattern of TM orders c) additional investigations as result of abnormal TM result and d) final diagnosis. Finally, appropriateness of the TM order was judged after review of the data for each patient.Following the completion of our audit data we assessed the financial implications of the inappropriate TM orders. We used the tariff (see appendix 2) for each TM during the audit period to estimate the financial impact.
4. Results
- During the audit period, 482 TM requests were made, of which 131 TM orders that met the audit criteria were audited.a) Reason for TM request (Fig1)The reason for the request was either not clear or not specified in 57% of orders and TMs were ordered for a wide range of conditions and presentations. In around a fifth of the cases, it was for diagnosis of suspected malignancy and 7% and 2% for surveillance and monitoring of known cancers respectively. TM requests were for screening of malignancy in 10% of the cases.The five most common final diagnoses were as follows: non-malignant hepato- biliary disease (23), benign prostatic hypertrophy (9), and gastro-esophageal reflex disease (8), ‘no malignancy’ (8). Only 18 out of the 131 patients had a confirmed cancer diagnosis.
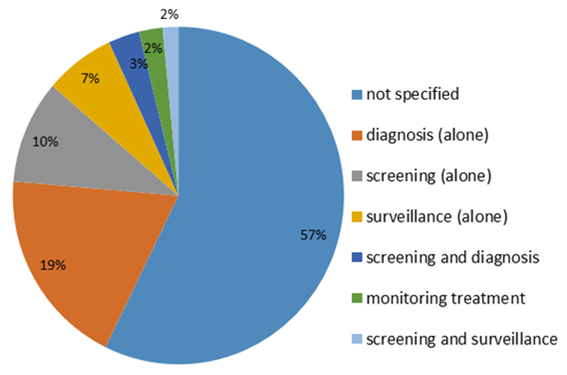 | Figure 1. Reason for TM order |
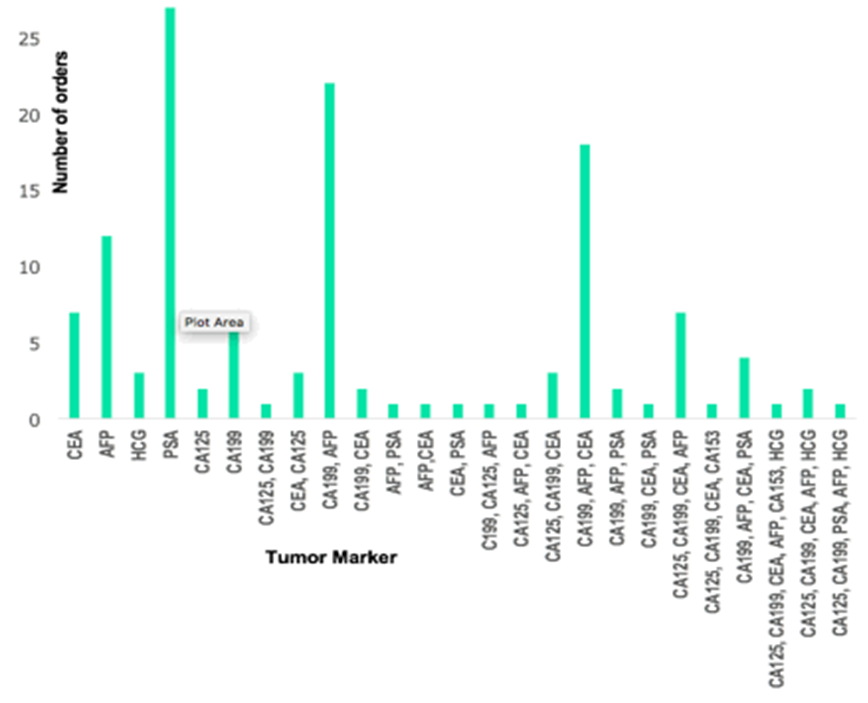 | Figure 2. Pattern of TM orders |
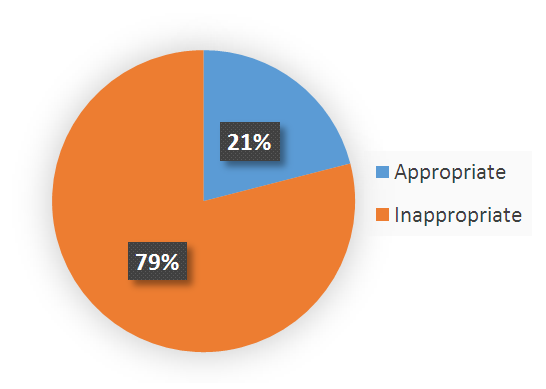 | Figure 3. Appropriateness of TM orders |
5. Discussion
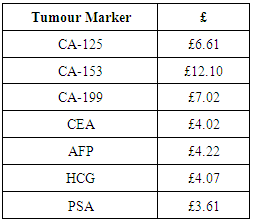
- There are limited and specific indications for TM use in screening, diagnosis and surveillance of malignancy as per the published guidelines. Despite the limitation of TMs, increasing TM requests are made both in general practice as well as in teaching hospitals. Our audit showed that 79% of the orders were inappropriate, a practice that seems to be widely prevalent as shown by numerous audits and retrospective studies. In an audit on the use of TMs in general practice, a staggering 84% TM requests were deemed inappropriate [5]. Our audit also showed multiple TM orders in more than half of the cases and in several cases a panel of TMs were ordered, a practice not supported by any guidelines. The extreme case of inappropriate requests was highlighted in an audit from a teaching hospital in Turkey where 23% of CA 125 (marker used for ovarian cancer) and 26.6% of CA 15-3 (maker used for breast cancer) requests were made in men. [6] The reason for TM orders in more than half of the cases in our audit is unclear from the notes and it appears that in many instances these were used in investigation of symptoms or presentations of suspected cancer. There is no evidence for routine use of TMs in the work up of suspected malignancy and TMs are generally not useful in identifying the primary in patients presenting with metastatic carcinoma of unknown primary. National Institute for Health and Clinical Excellence (NICE) guidance on carcinoma of unknown primary sets out the specific indications for TMs in presentations of metastatic disease with unknown primary [7]. In majority of cases in our audit, neither the presentation nor the final diagnosis justified the TM order and importantly we could not see any role for TMs in the diagnosis or the management of the patient. The inappropriate use of any test such as TM comes with consequences that could be harmful. For the patient, the abnormal results could bring unnecessary anxiety and distress. The raised TMs might prompt clinician to order imaging and investigations, many of which could be invasive with the attendant risks and this could result in further anxiety and stress for the patients. Furthermore, it can initiate inappropriate referrals. In our audit, additional investigations were performed in 12 cases as result of abnormal TMs. In a retrospective study on the utility of imaging carried out because of elevated common TMs, McMahan et el found that imaging was futile in diagnosing the malignancy or providing an explanation for the cause of raised TMs. A mean of 1.2 imaging studies were carried out per patient because of elevated TM, which is significant waste of resources as well as money. [8]The financial implication of inappropriate orders cannot be underestimated particularly in the current financial crisis, which is putting strain on the health services across the world. Extrapolating the data for the one-month audit, we estimate that over £ 12000 could be lost per year from the inappropriate orders. If we were to assume that a modest 30% of the estimated 15 million TM request made per year in the United Kingdom, [9] are inappropriate, this could result in a loss of 18 million pounds a year (an average cost of £4-5 per TM request). The financial impact could be much higher if we add other overheads such as cost of phlebotomy, transport of samples, doctors and laboratory technicians’ time and the cost of additional investigations.One of the reasons for the widespread use TMs appear to be the lack of understanding of the limitation of TMs and awareness of guidelines on the use of TMs among clinicians. Several measures have been suggested that might change clinicians’ behavior and help in curtailing the inappropriate TM requests in clinical practice. Education on the guidelines and auditing of TM’s requests is vital to change practice. Use of technology could help reduce inappropriate TM requests. Majority of hospitals now use electronic ordering system for laboratory investigations. It is possible to use flags or alerts when a TM is ordered, that will guide the clinicians on specific indications as well as the frequency of the testing of TMs. In addition to these measures, it also calls for a strong leadership from clinical biochemistry department, empowering the department to reject orders that are not in line with the guidelines. We plan to implement these measures to bring a change in the current practice of TM orders. It is imperative that we as clinicians take lead in cutting costs of unnecessary investigations including TMs.
6. Conclusions
- Routine use of TMs is unjustified and clinicians should restrict TM requests complying with the published guidelines on the use of TMs. Education and training of clinicians and strict implementation of TM guidelines could deliver substantial cost savings for the health services.
ACKNOWLEDGEMENTS
- The authors would like to acknowledge Dr. M. Leonard and Dr. M. Sargazi, Department of Biochemistry at WUTH for supplying the list of TM orders and Clinical Governance and Audit Department at WUTH for providing access to the case notes.
Appendix 1: Appropriate TM Requests
Appendix 2: Tariff for Tumour Markers (2010)