-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2017; 7(3): 119-141
doi:10.5923/j.ajmms.20170703.05

Gender Based Violence and People’s Attitudes toward Sexual and Reproductive Health in Jerusalem
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSumaya Sayej, Mohammad Qtait
Nursing Department, Faculty of Health Professions, Al-Quds University, Palestine
Correspondence to: Mohammad Qtait, Nursing Department, Faculty of Health Professions, Al-Quds University, Palestine.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Since 1967, when Israel occupied the Palestinian territories and annexed East Jerusalem illegally, the city Palestinian inhabitants have experienced multiple violations including, but not limited to; division of Arab Jerusalem governorate into two parts J1 and J2. The PCBS-Jerusalem statistical Yearbook (2010) described J1 is the part of Jerusalem that was annexed forcefully by Israel and “J2” includes the remaining of the governorate. It is worth noting that J1 area is the study target area. The study design: This descriptive exploratory study has utilized random sampling approach for targeted households as possible. The study targeted 309 households; two third of the sample from the old city and the other third from its suburbs, Al-Tor and Silwan, Shufat and Bait Hanina, Sorbaher and Biet Safafa representing “J1” areas. The study targeted one eligible respondent in each household to answer the questionnaire representing all his family members. The study utilized quantitative and qualitative. Study results: The socio-demographic and political factors indicated that East Jerusalem is fragile if not in a disaster state resulting from restrictive movement, reduction of the living spaces, house demolitions and evictions, restrictions on the right of access to basic education, and the deteriorating economic situation. In addition to social and behavioral problems such as the spread of drug abuse and alcohol consumption, early marriage, interfamily marriage and large families living in overcrowded houses, lack of security and stress are all factors combined together to be reflected on the individuals and their families in the form of gender-based violence that is directed towards the weakest in the equation, namely, women in particular and the Palestinian people as a whole. Social and behavioral problems including drug abuse, alcohol drinking and smoking are very much abundant among Jerusalem people and at increasing pace. The study revealed that family structure and dynamics of its members are reflected in behavioral practices to increase drug abuse, alcohol consumption and domestic violence when majority of participant agreed that disrupted families, divorced and separated families are more vulnerable than those large or poor families. The focus group discussion with all target groups reiterated on the disadvantaged situation of Palestinian people in Jerusalem who are living under two legal systems, the Israeli and the Palestinian but neither one of them is working on the issues discussed in this study leaving people feeling lost, insecure and unprotected as said “we are lost, we are neither under Israeli nor Palestinian Authority governance”. Complicated by the issues socio-political mentioned above have left them with the feeling of hopelessness and despair from the unclear future and with no horizon for political solution.
Keywords: Gender, Violence, Attitudes toward Sexual and Reproductive
Cite this paper: Sumaya Sayej, Mohammad Qtait, Gender Based Violence and People’s Attitudes toward Sexual and Reproductive Health in Jerusalem, American Journal of Medicine and Medical Sciences, Vol. 7 No. 3, 2017, pp. 119-141. doi: 10.5923/j.ajmms.20170703.05.
Article Outline
1. Introduction
- The Union of Charitable Societies (UCS) aims to improve living conditions of Palestinians in Arab East Jerusalem through the project “Reduction of Gender Based Violence (GBV), sexual exploitation and STDs” funded by Arab Gulf and Kuwaitis committees. Within the framework of this project, the UCS conducted a baseline survey target different population sectors from east Jerusalem including; women in reproductive age (15-49) years, men aged 25 and more, and young people aged (15-25) years. The survey strategic objective was to establish solid base information about target population demographic data and the contextual factors (familial, social and political) influencing their living conditions, and to identify their knowledge, attitudes and practices (KAP) regarding SRH, gender equality, and GBV. To have more detailed information about the study variables, interviews and group discussion was conducted with key government representatives from Ministry of Health, Ministry of Social Affairs and Ministry of Women Affairs and UCS as a steering committee, and with NGOs and civil society organizations representatives working in areas and overlapping with women empowerment, human rights, SRH issues and youth. The people living in East Arab Jerusalem have been under Israeli occupation for many decades, and their chances for intervention programs are scarce compared to West Bank. The UCS (2010) indicated in its rapid appraisal assessment for young people needs in Jerusalem that have easy access for entertainment in West Jerusalem and this may increases their vulnerability to practice unprotected sexual relations with sex workers which is likely to increase their exposure to HIV/AIDs and sexually transmitted infections. The same survey indicated high rate of unemployment among poor families, high rate of school drop out and early marriage, in addition to high rate of drug users are all factors that causes many social and behavioral problems leading to GBV, sexual exploitation and harassment.Writings on gender-based violence (GBV) are rich and varied. Joint United Nations Program on HIV/AIDS (UNAIDS, 2006) identified the term 'sex' refers to biologically determined differences, whereas the term 'gender' refers to differences in social roles and relations between men and women, learned through socialization and vary widely within and between cultures. Gender roles are also affected by age, class, race, ethnicity and religion, as well as by geographical, economic and political environments and GBV is understood as any type of violence directed at groups or individuals on these bases (UNAIDS, 2006). Harvard School of Public Health (2006) emphasized the definition of GBV as “it encompasses, but not limited to violence against women (VAW) and it is important for distinction as GBV and VAW are often, erroneously, used synonymously”. Research, policy and programmatic literature on GBV often encompass attention to human rights and to sexuality (is how people experience and express themselves as sexual beings) within their conceptual approach where this study will follow this approach highlighting gender relations within SRH and GBV.Taking into consideration the political and social factors influencing the living conditions of target people and their families in east Jerusalem, it is assumed that socio-behavioral problems such as drug abuse, alcohol consumption and unsafe sexual practices is a result of these factors. Thus, this survey aims to address these problems and their impact to predispose individuals and families to GBV and STIs.
1.1. Goal and Objectives
- The main goal of this survey is to highlight the needs of the target population in Jerusalem by establishing solid base information on knowledge, attitudes and practices of youth, women and men regarding women’s rights, GBV, and STIs. To achieve this goal, the following measurable objectives are set; 1. Assess the participants’ socio-demographic characteristics and living conditions (age, marital status, relation to spouse, number of family members, employment, education etc…) 2. Identify contextual factors (familial, political and social) influencing target group’s behavioral patterns (family environment, Israeli violations, and socio-behavioral practices etc…) and its impact on GBV 3. Assess prevalence and reasons for GBV within the participant’s home environment (reasons, perpetrators, prevalence, extent and type of violence, etc…) 4. Explore participant’s knowledge of common STIs including HIV and their availability within their communities (recognize at least 3 modes of transmission and 3 ways for prevention)5. Understand participant’s knowledge, attitudes and practices of selected SRH issues and gender equality matters (family planning, maternal health, STIs, male involvement in these matters, early and interfamily marriage etc…)6. Assess impact of GBV on women and on their choices and achievements (consequences of GBV and seeking behaviors toward health services and protection facilities as well as their availability within their communities).
2. Literature Review
- According to Rummel (1976), social practices are rules, norms, custom, habits, and the like that encompass or anticipate another person's emotions, thoughts, or intentions. Also added, considering the constituents of behavior (agents, ways and meaning), kinds of behavior (reflex, act, and practice), is what distinctively social behavior about. Regarding the socio-behavioral practices, Ramahi in its’ report (2011) “The scourge of drugs in Jerusalem” commented that increased drug use and abuse in Israel, especially post-1967, affected the Palestinian community across what was a relatively open border between Israel and the occupied West Bank including East Jerusalem. The report indicated that around 75% of known drug addicts in Palestine were people engaged in jobs in Israeli factories, farms and even settlements. The Islamic-Christian Front (August 2008) in Ramahi Report (2011) indicated that Jerusalem’s central location made it an ideal place for the distribution of illegal drugs where the numbers of drug addicts and abusers in 1986 has ranged between 200 and 300, these numbers now are more than 6,000 addicts and thousands more casual users in Jerusalem alone. In a recent report for ‘Maan’ Agency (June 19, 2012), the director of Combating Drugs Administration pointed that the numbers of addicts reached up to sixty thousand in OPT, of those twenty thousand in Jerusalem and its suburbs in 2007, and further stressed that a recent numbers of addicts in Jerusalem can’t be identified due to lack of effective institutions in this area.The role of excessive alcohol consumption or substance abuse in gender-based violence cannot be overlooked. Many studies indicated that in stressful situations, people often turn to alcohol and drugs to alleviate their stress and misery. Sometimes changes in gender roles when men are unemployed and can’t fulfill their traditional roles will lead to frustration, and thus use alcohol or drugs as a coping mechanisms and consequently will lead to gender-based violence (Whiezberg, et, al. 2008) such as the case of occupied oPt including Jerusalem.Al-Jazeera Channel report (June, 2011) and through interviews with some CBOs representatives in Jerusalem where they emphasized the lack of meaningful support from Palestinian official authorities to work on preventing drug abuse or rehabilitating abusers. One of the representatives described east Jerusalem as such “There is no authority, no security and no police and it’s easy to steal cars and rob houses” while another said “Jerusalem has become like a supermarket for drugs". Palestinian Authority Spokesman acknowledged the problem when said "these areas are suffering because we are not allowed to function there, and Israel is neglecting them as part of its eviction and marginalization policy". According to OCHA-Opt (March, 2011) the PA is not allowed to operate in East Jerusalem under the Oslo Accords and the closure of Palestinian institutions such as the Orient House are all factors that led to political and institutional vacuum in addition to restrictive residency and access policies resulting in isolation of east Jerusalem from the remainder of OPT – physically, politically, socially and culturally. The violation on the land and people has been seen on the ground and been reported by many local and international reports. The impact of the wall survey conducted by IPPC (2009) commented; construction of the separation wall was a unilateral decision by Israel and represents the maximal extent of the physical separation between Jerusalem and the area around it. It also gives the Israelis the ability to determine access to the city, thus weakening the relationship between Jerusalem and its Palestinian suburbs from the rest of the West Bank. Furthermore, the report indicated the establishment of the wall has excluded 65,000 Palestinian Jerusalemites from their own city and now they find themselves threatened with the loss of their Jerusalemite residence. The Jerusalem Statistical Yearbook (JSY, No. 13, 2011) shows the total population of Jerusalem Governorate in 2010 was 382,041 persons, of which 237,301 in the Area “J1”1 and 144,740 persons in the Area “J2” making 9.6% of the total occupied Palestinian Population. “JI” Includes that part of Jerusalem that was annexed forcefully by Israel following its occupation of the Palestinian Territory in 1967 and “J2” includes the remaining of the governorate, except J1 (please refer to the Map of Jerusalem clarifying this partition at page (ii) of this report). It is worth mentioning that “J1” the target study area constitute around 91% of Jerusalem people who live in urban areas and 9% live in camps, meaning that “JI” does no include rural areas while 30.5% of the population in J2 area are living in rural areas. The PCBS-JSYB, (No. 10 report 2008) reported on Israeli violations regarding houses and people in Jerusalem Governorate as; the number of demolished houses was 1,501 houses affecting 7.413 persons while the violation on the people existence within these houses was indicated by the increasing number of confiscated identity cards (ID) or Hawieh. This was confirmed B'Tselem (2008) when indicated that Israeli Ministry of Interior announced the confiscation of 14.138 identity cards for the heads of households during the period 1967-2010, which means this number is much more considering the number of their families. Same source reported on 4.672 confiscated ID for the year 2008 only (the Israeli Information Center for Human Rights - B'Tselem, 2008). Such political discrimination and power exertion by the Israeli occupier on the weak Palestinians have left them to encounter social and behavioral problems manifested by increased poverty and unemployment rate, increased number of drug users, alcohol consumers. Al-Saiegh (2006) study on drug abuse in Jerusalem found that 72.4% of drug users are unemployed and 70.8% has quitted their jobs because of drug addiction and 53.6% were illiterate leaving a large sector of young people to loose interest in values and achievements with the aim of the occupier to keep them in a weak character away from social and national matters. The estimated population at end of 2010 in the OPT was 4.1 million with a sex ratio of 103.1 male to female (PCBS, women and men in Palestine, 2011). The average population growth in the OPT is one of the highest in the world: it reached 2.66%, while the yearly average population growth worldwide is 1.4%, in Jerusalem 1.84% according to PCBS-JSY statistics for the year 2010. The fertility rate is 4.2 in OPT; 3.8 in West Bank and 4.9 in Gaza Strip as indicated by the Family Heath Survey (2010). The median age of first marriage 19.9 years among women according to 2009 PCBS statistics. The Jerusalem statistical yearbook (2011) indicated that registered marriages in Shariah Courts and Churches for females aged 15-19 years in the year 2009 was 9283 or 46.8% of all marriages in the West Bank while the number of marriages for females in same age group in Jerusalem governorate was 1588 representing 54.6% of the total marriages meanwhile for same age group among males was 5.2% of all registered marriages in WB and Jerusalem. The average household size in Jerusalem Governorate is 5.2 persons compared with 5.8 persons in the Palestinian Territory, 81.1% are nuclear families, 9.0 extended families, and 10% polygamous and single. Regarding housing and housing conditions; average number of rooms in Jerusalem governorate houses is 3.3 rooms for the year 2007 (3.1 rooms in J1 Area and 3.8 rooms in J2 Area), the average housing density reached 1.6 persons per room while 38.5% of the households live in housing units with two persons and more per room (PCBS-JSYB, No. 13, 2011). During 2010, about 8 out of every 100 females aged 15 years and above are illiterate; which is four times higher than males in the same age group. In the same context, the gender gap has decreased during the past 10 years where the percent increase in the literacy rates of females 15 years or above is about four times higher than that of males during the period 2000-2010 (PCBS-JSYB, No. 13, 2011). Gender-based violence is violence against women based on women’s subordinate status in society. It includes any act or threat by men or male dominated institutions that inflict physical, sexual, or psychological harm on a woman or girl because of their gender. In most cultures, traditional beliefs, norms and social institutions legitimize and therefore perpetuate violence against women. Gender-based violence happens in all societies, across all social classes, and with women particularly at risk from men they know (UNIFEM, 2002, UNICEF 2003). According to Miftah study (2006), the relationship between occupation, patriarchy and GBV is clear; rising poverty and unstable living conditions have placed a tremendous socio-economic pressure on families where women and children have been deeply affected by the widespread violence resulting from all these factors. On the one hand, the prevailing culture and gender stereotypes in the OPT undermine women enjoyment of their rights and equal participation with men. On the other hand, the unstable geo-political and socio-economic situation, reinforce legal instability and disrupt human security in ways that are particularly detrimental to women. Miftah (2006) also indicated that GBV do exist in the Palestinian society due to the conservative nature and the patriarchal culture, it is difficult to find out the real numbers of women exposed to violence. A study conducted by Sayej (2008) for the Palestinian Family Planning and Protection-PFPPA on “the impact of the separation wall on youth and parents perceptions and practices toward SRH and gender relations in Jerusalem Governorate” indicated a clear relationship between occupation and GBV and that the impact of the political and social factors has increased poverty and unstable conditions among families increased the chance for extra social problems including GBV. Gender inequality and male dominance in decision making regarding women sexual and reproductive health and rights was exemplified by the increased level of early marriage and interfamily marriage compared to national surveys, also youth and their parents lack knowledge regarding SRH and rights matters and have difficulties in information exchange regarding these matters.
3. Study Methodology
3.1. Study Design
- This descriptive exploratory study has utilized quantitative and qualitative methods for data collection in a complementary manner to comprehensively cover the research components and to have information about the availability, extent and severity of GBV including domestic and sexual violence and STIs. The target groups were women (15-49) years, men aged 25 and more, and young people (15-25) years, living in Area around of Jerusalem governorate.
3.2. Development of the Research Tools
3.2.1. Development of the Questionnaire
- The questionnaire was based on the study objectives and concepts. The preliminary findings of FG discussion with CBOs’ representatives working in the area were of great help in structuring the qualitative information in a quantitative approach. The quantitative questionnaire included 3 major parts; first one was on socio-demographic variables, the second part was contextual factors (familial, social, and political) affecting the living conditions of the target groups where most of the items were dichotomous on yes and no with some open questions for further explanation of responses. The last part was 62 items constructed under subcategories and arranged in a 5-point response Likert scale format ranging from strongly agree to strongly disagree on items reflecting target groups’ perception and practices of selected SRH and gender relation, some social and family issues related to selected negative socio-behavioral practices and drug abuse. Another 37 items arranged in a 3-point response format reflecting participants’ experiences of selected domestic violence issues, their knowledge of accessibility and availability of health and social information and services.
3.2.2. The Questionnaire Validity and Reliability
- The content validity was established when experts in research, health and gender studies, the steering committee and UCS administration revised and approved the questionnaire. The questionnaire was tested for Cronbach coefficient alpha reliability through SPSS analysis. Cronbach coefficient alpha is a measure to assess the internal consistency of the instrument by correlating each item with all other possible combinations of other items (LoBiondo-Wood and Harber, 2003). The tool was developed in English first, translated into Arabic to collect the data for the pilot study and to ensure reliability again prior to its distribution to target groups into the field.
3.2.3. The Qualitative Data Tools
- The qualitative data was semi-structured open-ended questions aimed at obtaining detailed information about the study concepts, difficulties and constraints that CBOs and institutions may encounter, and lastly their future recommendation regarding health, social services and policies to reduce incidence of social problems and GBV within the scope of their work. A similar open-ended questions aimed at obtaining detailed information through FG discussion with study participants’ to complement quantitative data responses.
3.3. Participant’s Selection and Sampling approach for Quantitative Data
- A stratified random sampling approach for selection of households was utilized as possible. According to TOR, the study aimed to target 300-350 households from east Jerusalem; two third of households from the old city and the other third from its suburbs; Al-Tor and Silwan, Shufat and Bait Hanina, Sorbaher and Biet Safafa aiming at obtaining information on the study concepts from all Jerusalem “J1” areas. The study targeted one eligible respondent in each household to answer the questionnaire representing all its members. Thus the study aimed at representing data sufficient enough to reflect the demographic characteristics and contextual factors affecting the Jerusalemite living conditions including gender equality and GBV, SRH and STIs.
3.4. Accessibility and Ethical Consideration
- The data collectors went directly to the selected accessible households explained the purpose of the study and ensured participants for anonymity and confidentially, they further explained that results and conclusions made through information obtained will be used for the research purposes only. A letter of agreement was signed by the researcher supported by a formal letter signed by the UCS management describing the purpose of the study and asking for permission to conduct the study was another ethical safeguard (Please refer to the permission letter from UCS A-1 and letter of agreement attached with each questionnaire in annex 2).
3.5. Data Collection Procedures
3.5.1. The Quantitative Data Collection
- The quantitative data collection from study participants was obtained after one day training workshop held with the data collectors and the statistician. There were two teams for data collection; one male and one female in each to ease their accessibility into the households. There was one field supervisor to double check the data collection process, the principle researcher of the study has coordinated the activities of data collection with the research team to have a consensus on obtaining the data from respondents as close as possible. To this end, they explained the purpose of the questionnaire, encouraged all participants to voice their opinions and share in the study.
3.5.2. The Qualitative Data Collection
- The qualitative data included one FG discussions with CBOs and institutions’ representatives working in areas and overlapping with women and youth issues where information obtained have helped in identifying the concepts under study and been utilized for structuring the questionnaire. Another 4 FG discussion were conducted with target groups (1 FG with young girls in private school, 2 FG (focus group) with youth centers included males and females and 1 FG with abused women) aimed to complement the participants’ responses in the questionnaire and will be reiterated upon in the discussion chapter. The focus group discussion was conducted by the principle investigator and field supervisor to have reliable and consistent information on the study objectives. Some of the responses were documented by using the same phrases of the participant through the text.
3.6. Data Analysis Procedures
3.6.1. Quantitative Data Analysis
- After the data collection completed, the complied data was assembled, cleaned, and analyzed using SPSS program (Statistical package for Social Science No.20). 324 questionnaires were collected from households in the targeted localities, 15 were discarded because of incompletion. The data results were compiled into tables and their interpretation presented into narrative style in the analysis and discussion chapters.
3.6.2. Qualitative Data Analysis
- A thematic analysis approach was utilized guided by the objectives and key questions of this research study. All data collected was assembled (the field notes, transcripts, personal comments) and carefully read through and thoroughly until the investigator become intimately familiar with them. This process facilitated the formation of the themes by clustering and coding the statements expressed by the respondents under each question. This process guided the researcher to describe and discuss the results explicitly and to develop recommendations. Also the findings were compared and contrasted with existing literature and other theoretical perspective of the proposed study.
4. Analysis and Findings
4.1. Statistical Analysis and Results
4.1.1. Socio-Demographic Data
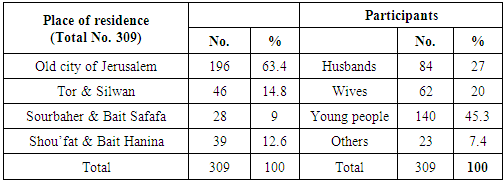
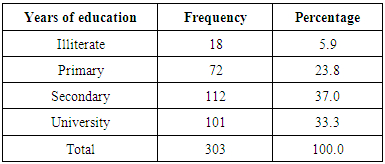
- Sample distribution and sample size (Table 1): 309 households were accessed and involved in the study; around 63.4% are residing in the old City of Jerusalem, and 36.4% are residing at the suburbs of east Jerusalem or what is called “JI” area (Tor & Silwan 14.8%, Sourbaher & Bait Safafa 9% and Shou’fat & Bait Hanina 12.6%). The household’s represented by; 27% husbands, 20% wives, and 45.3% young people and 7.4% for others, which means either divorced, widow or separated. The participant’s age has ranged from (15- 61) years with an average of 27 years and the higher frequency of participants was for the age 20 years.
|
|
|
|
|
|
|
|
|
4.2. Data Analysis of the Contextual Factors Questions
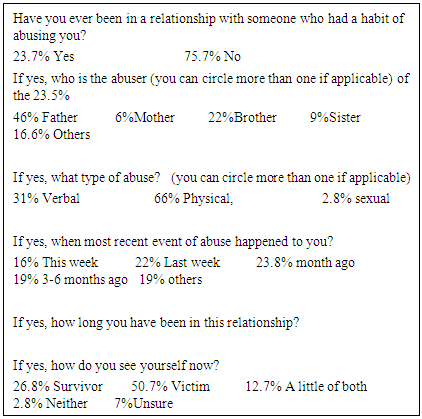
- To measure the second and third objectives of the study, contextual factors (home, social and political) and their impact on target groups and their families were identified in terms of behavioral patterns, and availability, extent, forms and perpetrators of GBV. There are 8 subcategories to identify these factors and most of the items are dichotomous on yes and no response with some open questions for further exploration of the responses. Domestic violence within the home environment (Table 4.2); around 24% of the participants have indicated their responses to being abused within their home environment. Of those, 66% were exposed to physical violence and 31% to verbal/emotional violence knowing that verbal abuse will precede the physical one; this explains that domestic violence is available abundantly and extensively within their home environment for long time that ranged from few weeks to few years as they mentioned in the open ended questions. Of those abused, 46% claimed that fathers were the abusers, to less extent 22% for brothers, 16.6% were for others category (more than one person, grandfather, uncle and few said the in laws), followed and 9% for sisters and 6% for mothers. Around 3% reported sexual abuse, and this could be due to participant’s reservation on answering this private question. These figures indicate GBV is a fact taking its place among them when the majority 51% consider themselves victims, and 26.8% survivors. When they were asked about last time they were abused; 24% reported a month ago, 22% a week ago, 19% 3-6 months ago, and 16% reported this week and at any time when 19% reiterated under others category as (at any time, when father feel frustrated, when brother’s orders are not met etc…)
4.2.1. Domestic Violence within the Home Environment
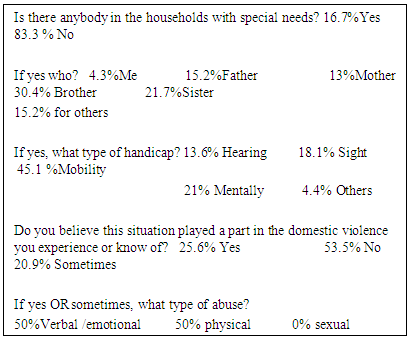
 Prevalence of persons with special needs (handicaps) within the households (table 4.2.2); 17% of participants agreed to the availability of persons with special needs. Of those, 4.3% were the participants; the majority was for brothers 30.4% followed by 21.7% for sisters, 15.2% for fathers, 13% for mothers and 15.2% for others (grandfather/mother or relative etc…). The handicaps were of different types but mobility problems rated the highest among all reaching 45% among all, followed by 21% for mental health problems, 18% for sight problems, and 13.6% for hearing problems. When participants were asked if this situation played a part in the domestic violence they experience or know of; 25.6% agreed and 21 agreed on sometimes with 50% for emotional/verbal abuse and 50% for physical abuse.
Prevalence of persons with special needs (handicaps) within the households (table 4.2.2); 17% of participants agreed to the availability of persons with special needs. Of those, 4.3% were the participants; the majority was for brothers 30.4% followed by 21.7% for sisters, 15.2% for fathers, 13% for mothers and 15.2% for others (grandfather/mother or relative etc…). The handicaps were of different types but mobility problems rated the highest among all reaching 45% among all, followed by 21% for mental health problems, 18% for sight problems, and 13.6% for hearing problems. When participants were asked if this situation played a part in the domestic violence they experience or know of; 25.6% agreed and 21 agreed on sometimes with 50% for emotional/verbal abuse and 50% for physical abuse. 4.2.2. Persons with Special needs in Each Household
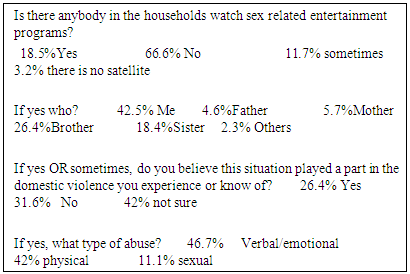
 Persons watching sex related entertainment programs (table 4.2.3); around 19% of participants reported yes and 11.7% reported sometimes. Of those who watch such programs, 42.5% were the study participants, followed by 26.4% for brothers and 18.4% for sisters. When participants were asked if this situation played a part in the domestic violence they experience or know of; 26.4% agreed and 42% were not sure. When asked about the type of abuse; 46.7% was for verbal/emotional, 42% for physical and 11.1% sexual abuse where this is only factor that triggered the participants to mention sexual violence. It is noteworthy that 3.2% of the participant does not a satellite at home.
Persons watching sex related entertainment programs (table 4.2.3); around 19% of participants reported yes and 11.7% reported sometimes. Of those who watch such programs, 42.5% were the study participants, followed by 26.4% for brothers and 18.4% for sisters. When participants were asked if this situation played a part in the domestic violence they experience or know of; 26.4% agreed and 42% were not sure. When asked about the type of abuse; 46.7% was for verbal/emotional, 42% for physical and 11.1% sexual abuse where this is only factor that triggered the participants to mention sexual violence. It is noteworthy that 3.2% of the participant does not a satellite at home.4.2.3. Persons Watching Sex Related Entertainment Programs
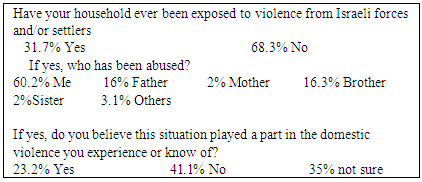
 Exposure of households to violence from Israeli forces and/or settlers (table 4.2.4); around 32% of the participants’ households were violated by the Israelis. Within this violation 60% of the study participants were abused, followed by 32% for males (16% for fathers and 16% for brothers), 4% for females (2% for mothers and 2% for sisters) and 3% for others (extended family members). Furthermore, 23.2% agreed that Israeli violations have contributed in the domestic violence they experience or know about.
Exposure of households to violence from Israeli forces and/or settlers (table 4.2.4); around 32% of the participants’ households were violated by the Israelis. Within this violation 60% of the study participants were abused, followed by 32% for males (16% for fathers and 16% for brothers), 4% for females (2% for mothers and 2% for sisters) and 3% for others (extended family members). Furthermore, 23.2% agreed that Israeli violations have contributed in the domestic violence they experience or know about. 4.2.4. Exposure of Households to Violence from Israeli Forces and/or Settlers
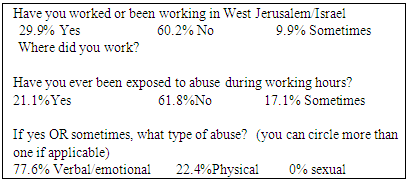
 Persons worked or been working in West Jerusalem/Israel (table 4.2.5); around 30% of participants worked and still working in West Jerusalem/Israel and 10% have worked occasionally in restaurants, factories and as laborers but no one mentioned night clubs. When asked if they were exposed to abuse during working hours, 21% said yes and 17% said sometimes and the type of abuse they were exposed to was 78% for verbal/ emotional and 22.4% for physical abuse.
Persons worked or been working in West Jerusalem/Israel (table 4.2.5); around 30% of participants worked and still working in West Jerusalem/Israel and 10% have worked occasionally in restaurants, factories and as laborers but no one mentioned night clubs. When asked if they were exposed to abuse during working hours, 21% said yes and 17% said sometimes and the type of abuse they were exposed to was 78% for verbal/ emotional and 22.4% for physical abuse.4.2.5. Persons Worked or been Working in West Jerusalem/Israel
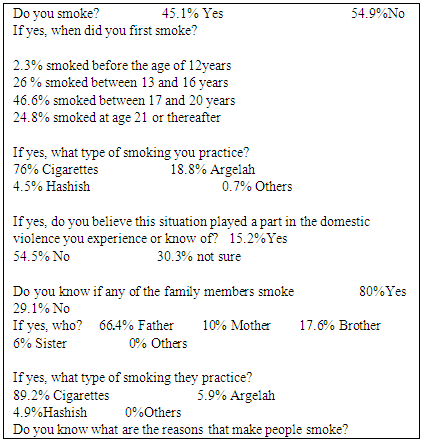
 Smoking questions (table 4.2.6); 45% of participants are smokers. Of those, 2.3% smoked at age less than 12 years, 73% smoked at age between (13 and 20 years) and around 25% smoked at age 21 years or thereafter. Of those smokers; 76% smoke cigarettes, 18.8% smoke Argelah. Furthermore, 80% of the participants’ family members are smokers too; of those smoking; 89% smoke cigarettes, 6% smoke Argelah. 15.2% of participants agreed that smoking have played a part in the domestic violence they experience or know of. It is noted that that 4.5% of the participants and 5% of their family members’ smoke Hashish, and Argelah smoking is increasing too. The participants justified reasons for smoking as; unemployment, bad economic conditions, stress and psychological pressure and some young people through the FG discussion added “like to try new things” and “peer pressure”.
Smoking questions (table 4.2.6); 45% of participants are smokers. Of those, 2.3% smoked at age less than 12 years, 73% smoked at age between (13 and 20 years) and around 25% smoked at age 21 years or thereafter. Of those smokers; 76% smoke cigarettes, 18.8% smoke Argelah. Furthermore, 80% of the participants’ family members are smokers too; of those smoking; 89% smoke cigarettes, 6% smoke Argelah. 15.2% of participants agreed that smoking have played a part in the domestic violence they experience or know of. It is noted that that 4.5% of the participants and 5% of their family members’ smoke Hashish, and Argelah smoking is increasing too. The participants justified reasons for smoking as; unemployment, bad economic conditions, stress and psychological pressure and some young people through the FG discussion added “like to try new things” and “peer pressure”.4.2.6. Smoking Behaviors Questions
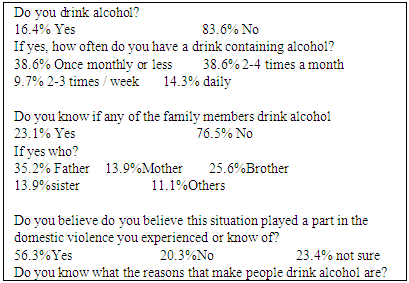
 Alcohol drinking behaviors questions (table 4.2.7); 16.4% admitted to have a drink containing alcohol; 14.3% drink on daily basis, 9% (2-3) times a week, 38.6% (2-4) times a month and 38.6% once monthly or less. Furthermore, 23% of participants family members drink alcohol, of those; 35% fathers, 25.6% brothers, 14% mothers, 14% sisters and 11% for others (other extended family members). When participants were asked if this situation played a part in the domestic violence they experience or know of; 56% agreed to yes, 20.3% no and 23.4% were not sure. The participants justified the reasons for such behaviors as; family problems, lack of religious commitment, lack of moral commitment, unemployment and economical situation, stress and psychological pressure, imitate others, try to have leisure and entertainment activities, try new things and bad companions. Within this context, it is worth mentioning that 5 Christian households only participated in this survey and the rest are Muslims.
Alcohol drinking behaviors questions (table 4.2.7); 16.4% admitted to have a drink containing alcohol; 14.3% drink on daily basis, 9% (2-3) times a week, 38.6% (2-4) times a month and 38.6% once monthly or less. Furthermore, 23% of participants family members drink alcohol, of those; 35% fathers, 25.6% brothers, 14% mothers, 14% sisters and 11% for others (other extended family members). When participants were asked if this situation played a part in the domestic violence they experience or know of; 56% agreed to yes, 20.3% no and 23.4% were not sure. The participants justified the reasons for such behaviors as; family problems, lack of religious commitment, lack of moral commitment, unemployment and economical situation, stress and psychological pressure, imitate others, try to have leisure and entertainment activities, try new things and bad companions. Within this context, it is worth mentioning that 5 Christian households only participated in this survey and the rest are Muslims. 4.2.7. Alcohol Drinking Behaviors Questions
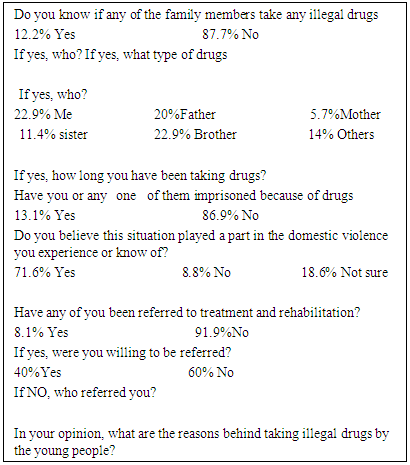
 Illegal drug use questions (table 4.2.8); 12.2% of participants knew about household members use of illegal drugs. Of those; 30% were the study participants, 20% were the fathers, 5.7% were the mothers, 23% were the brothers, and 1.4% were the mothers and 14% for others. The time for drug users has varied from months to years where some of them are known figures in the old city. Around 72% of the participants agreed this situation played a part in the domestic violence they experience or know of. Furthermore, they justified the reasons that make people take illegal drugs as; family problems, lack of religious commitment, lack of moral commitment, unemployment and economical situation, psychological pressure, imitate others, try to have leisure and entertainment activities, try new things and bad companions. As for the possible actions to reduce drug abuse 13% of the participants or their family members were imprisoned as a result of using illegal drugs and 8.1% were referred to treatment and rehabilitation, of those 40% were willing to be referred. Most participants reiterated on the role of civil society institutions in taking care of drug users and referring them to appropriate agency.
Illegal drug use questions (table 4.2.8); 12.2% of participants knew about household members use of illegal drugs. Of those; 30% were the study participants, 20% were the fathers, 5.7% were the mothers, 23% were the brothers, and 1.4% were the mothers and 14% for others. The time for drug users has varied from months to years where some of them are known figures in the old city. Around 72% of the participants agreed this situation played a part in the domestic violence they experience or know of. Furthermore, they justified the reasons that make people take illegal drugs as; family problems, lack of religious commitment, lack of moral commitment, unemployment and economical situation, psychological pressure, imitate others, try to have leisure and entertainment activities, try new things and bad companions. As for the possible actions to reduce drug abuse 13% of the participants or their family members were imprisoned as a result of using illegal drugs and 8.1% were referred to treatment and rehabilitation, of those 40% were willing to be referred. Most participants reiterated on the role of civil society institutions in taking care of drug users and referring them to appropriate agency. 4.2.8. Illegal Drug Use
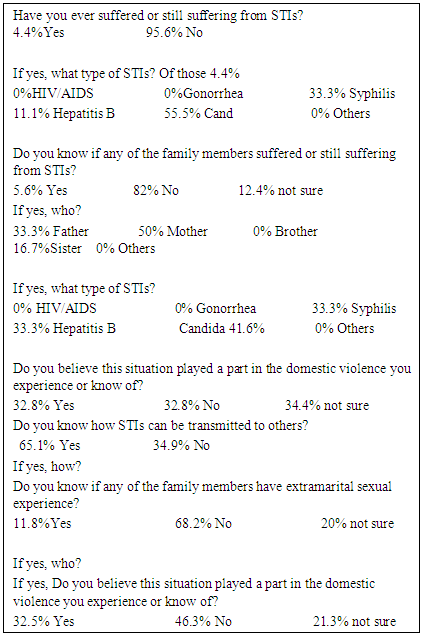
 Sexually transmitted infections and HIV questions (table 4.2.9) To achieve the fourth objective of the study and to understand the extent of STIs and HIV transmission, 4.4% of participants claimed that they suffered or still suffering from STIs. Of those; 33% suffered from syphilis, 1% suffered from hepatitis B, and 56% suffered from Candida while NO one reported on contracting HIV/AIDS. Around 6% of other family members contracted STIs, of those; 33% the fathers, 50% the mothers and 16.7% the sisters. To identify the types of STIs that family members are suffering; there was 33% for Syphilis, 33% for hepatitis B and 41.6% for Candida. Around 33% of the participants agreed this situation played a part in the domestic violence they experience or know of. The participants were assessed for their knowledge about STIs transmission modes, 65% reported yes and when asked to mention these modes, the most statements mentioned by the majority; illegal sexual relationships, having sex with multiple partners and blood transfusion. Very few mentioned that transmission can be through food, drinking or touching the patients. To identify factors that help in transmitting these diseases; the participants were asked about their knowledge of extramarital relations among family members, 12% agreed and 20% were not sure about it. But when asked who that family member was, the majority of responses were for brothers and fathers and very few said mothers and sisters and 32.5% agreed that this situation has played a part in the domestic violence they experience or know of.
Sexually transmitted infections and HIV questions (table 4.2.9) To achieve the fourth objective of the study and to understand the extent of STIs and HIV transmission, 4.4% of participants claimed that they suffered or still suffering from STIs. Of those; 33% suffered from syphilis, 1% suffered from hepatitis B, and 56% suffered from Candida while NO one reported on contracting HIV/AIDS. Around 6% of other family members contracted STIs, of those; 33% the fathers, 50% the mothers and 16.7% the sisters. To identify the types of STIs that family members are suffering; there was 33% for Syphilis, 33% for hepatitis B and 41.6% for Candida. Around 33% of the participants agreed this situation played a part in the domestic violence they experience or know of. The participants were assessed for their knowledge about STIs transmission modes, 65% reported yes and when asked to mention these modes, the most statements mentioned by the majority; illegal sexual relationships, having sex with multiple partners and blood transfusion. Very few mentioned that transmission can be through food, drinking or touching the patients. To identify factors that help in transmitting these diseases; the participants were asked about their knowledge of extramarital relations among family members, 12% agreed and 20% were not sure about it. But when asked who that family member was, the majority of responses were for brothers and fathers and very few said mothers and sisters and 32.5% agreed that this situation has played a part in the domestic violence they experience or know of.4.2.9. STIS and HIV Questions
4.3. Knowledge, Attitudes and Practices Questions Reflecting SRH, Gender Relations and GBV
- To achieve the fifth objective of the study; this part of the questionnaire is divided into 3 subcategories and graded under 5 points Likert scale from strongly agree to strongly disagree and given a value label coded from (1-5) sequentially. Each subcategory presented into table, responses with agree and strongly agree were combined together and responses with disagree and strongly disagree were combined together too since it gives almost the same value on the statement presented unless otherwise required to be indicated as it is.
4.3.1. Selected SRH and Gender Relation Issues (FP and Maternal health)
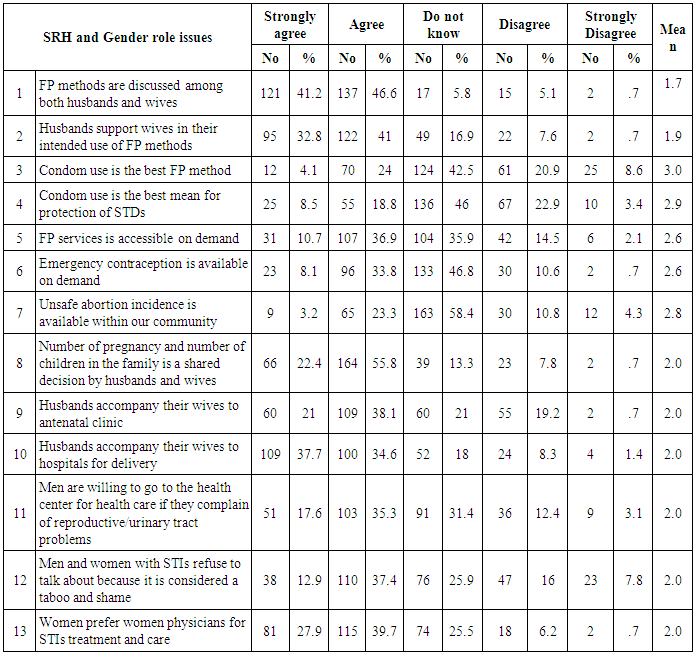
- To identify the participant’s knowledge, attitudes and practices (KAP) of selected SRH and gender relation issues, the level of male involvement was highlighted and the results were encouraging when more than 88% agreed that family planning methods are discussed among both husbands and wives and 74% agreed that husband’s support their wives on their intended use of FP. On the contrary, the situation is different when 28% agreed that “condom use is the best FP method”, and 27% only agreed on the statement “condom use as the best mean for protection of STIs”. Participants were asked about their knowledge regarding accessible family planning services on demand; around 48% agreed, 40% didn’t know. Also 42% agreed and 46% didn’t know about availability of emergency contraception when needed while 26% agreed and 58% didn’t know about the availability of unsafe abortion. With high level of “don’t know response” in this regard, means that participants are less knowledgeable about the importance of men’s FP methods use that need more focus through SRH awareness and services programs. To identify the participant’s attitudes on maternal health matters; 78% agreed that "number of pregnancy and number of children should be a shared decision among both spouses", 72% agreed that “husbands accompany their wives to hospitals for delivery”, and to less degree 59% agreed that “husbands accompany their wives to antenatal clinic” and 68% agreed that women prefer women physicians for STIs treatment and care indicating an attitude among men that need further involvement in SRH matters. Regarding men attitude toward their own SRH matters indicated that 53% only agreed on the statement “men are willing to go to health center if they complain of reproductive/urinary tract problems” and 31% didn’t know. Another attitude question regarding STIs “Men and women with STIs refuse to talk about because it is considered a taboo and shame”, 50% of agreed, 25% didn’t know and 25% disagreed. Such indicators emphasize the need for men awareness programs to take care for their own health and to understand their roles which ultimately will reduce the gender gap among both husbands and wives in SRH matters where this will be reflected on the family and the society as a whole.
4.3.2. Questions Reflecting Selected SRH and Gender Relation Issues
4.3.3. Selected Family Dynamics and Its Impact on Gender Relations
- This section started with identifying participant’s knowledge regarding marriage issues and gender relation (please refer to table 4.3.2). Majority of participants 84% agreed on the availability of interfamily marriage within their communities, 79% agreed on the availability of early marriage, and 72% agreed that early marriage is more happening among relatives. To further identify the political impact on early marriage, the responses were scattered; 40.6% agreed on the statement “Early marriage prevalence among girls is more noticed since the wall erupted and mobility restriction increased”. To identify participant’s attitudes toward marriage issues; 75% disagreed and 7.6% agreed on the statement “I’m in favor of early marriage”, and 71% disagreed vs. 16% agreed on the statement “I’m in favor of interfamily marriage”. Such responses reflect positive attitudes of participants but negative societal practices that require intervention programs in terms of awareness and law enforcement. Regarding family dynamics; only 63% agreed on the statement “decisions regarding family matters are shared within family members” and only 67% agreed on the statement “decisions regarding the marriage of the girls are shared with them” and to less extent when 39% agreed vs. 32% disagreed that “decisions regarding marrying the girls or boys are the father’s responsibility”.
4.3.4. Questions Reflecting Selected Family Dynamics and Its Impact on Gender Relations
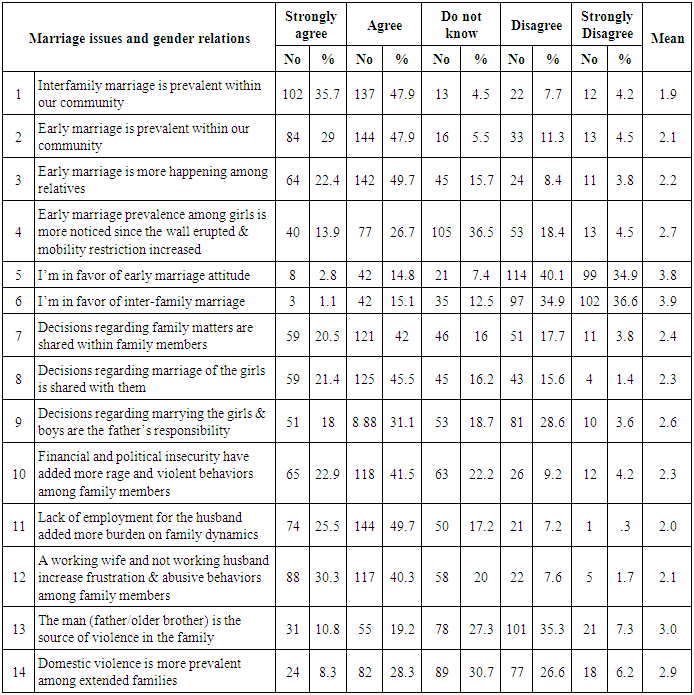 To identify the political and financial impact on participant’s violence attitudes and practices, 65% agreed on the statement “Financial and political insecurity have added more rage and violent behaviors among family members” and approved when 76% agreed on the statement “lack of employment for the husband added more burdens on family dynamics”. Within the same domain 71% agreed on the statement “A working wife and not working husband have increased frustration and abusive behaviors among family members”.Furthermore, there was a variation in responses of participants regarding home environment and GBV when 30% agreed, 43% disagreed and 27% didn’t know “the man (father/older brother) is the source of violence in the family”, also this variation was clear on the statement “domestic violence is more prevalent among extended families” when 37% agreed, 33% disagreed and 31% didn’t know.
To identify the political and financial impact on participant’s violence attitudes and practices, 65% agreed on the statement “Financial and political insecurity have added more rage and violent behaviors among family members” and approved when 76% agreed on the statement “lack of employment for the husband added more burdens on family dynamics”. Within the same domain 71% agreed on the statement “A working wife and not working husband have increased frustration and abusive behaviors among family members”.Furthermore, there was a variation in responses of participants regarding home environment and GBV when 30% agreed, 43% disagreed and 27% didn’t know “the man (father/older brother) is the source of violence in the family”, also this variation was clear on the statement “domestic violence is more prevalent among extended families” when 37% agreed, 33% disagreed and 31% didn’t know.4.3.5. Selected Family Factors and Drug Abuse
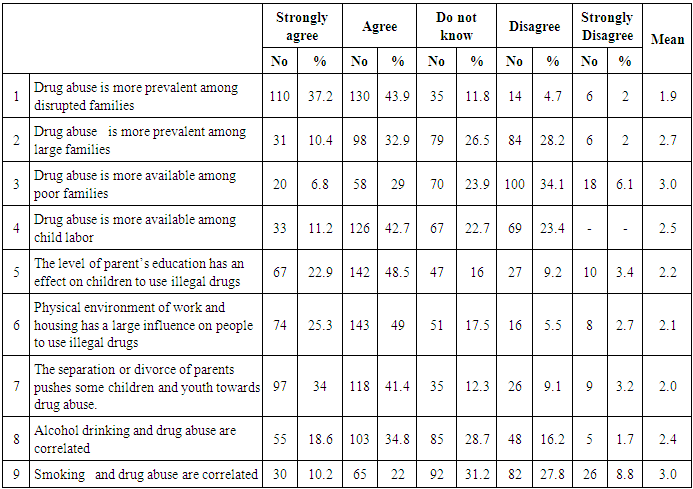
- This part of the questionnaire examined the societal and family issues and its impact to use illegal drugs (table 4.3.3). To identify the family characteristics and dynamics and the use of illegal drugs, 81% agreed on the statement “drug abuse is more prevalent among disrupted families”, and 75% agreed on the statement “the separation or divorce of parents pushes some children and youth towards drug abuse”. Furthermore, around 74% agreed that “the physical environment of work and housing has a large influence on people to use illegal drugs”, and to less extent 54% agreed vs. 23% disagreed on the statement “drug abuse is more available among child labor”.There was variation among participants’ responses regarding family characteristics and the use of drugs; 43% agreed, 30% disagreed and 27% didn’t know that “drug abuse is more prevalent among large families”, followed by 36% agreed, 24% did not know, and 40% disagreed on the statement “drug abuse is more available among poor families”, while 71% agreed and 13% disagreed on the statement “the level of parent’s education has an effect on children to use illegal drugs”. To identify participants’ knowledge on some social habits and drug abuse; 53% agreed, 29% didn’t know and 18% disagreed that “alcohol drinking and drug abuse are correlated”, 32% agreed, 31% didn’t know and 37% disagreed that “smoking and drug abuse are correlated” indicating that alcohol drinking is more associated with drug abuse than with smoking.
4.3.6. Questions Reflecting Selected Social and Family Dynamics and Drug Abuse
4.3.7. Participants KAP of Domestic and Sexual Violence; Consequences and Choices
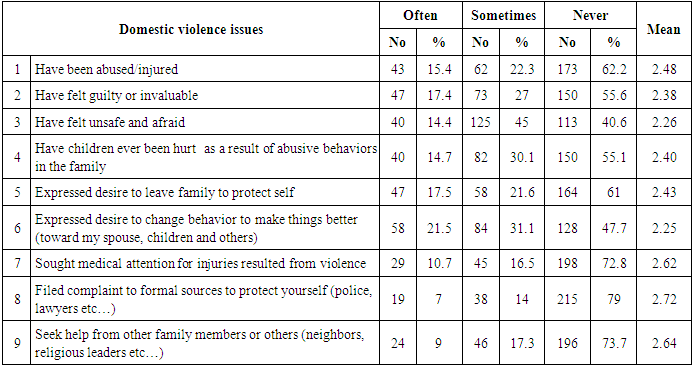
- To achieve the sixth objective, impact of GBV on women choices and achievements (availability of domestic and sexual violence, consequences and seeking behaviors toward health services and protection facilities) was identified. The questionnaire items in this regard are presented into 3 subcategories and the responses has been rated on 3 point scale where the value label coded from (1-3) to obtain the mean of responses for each item. The responses were relatively less than other responses and mostly for women and young girls, yet it complements the participant’s responses in section (4.2.1). The “never” option rated the highest among all because many participants refused to answer or denied the issue by saying never as been noted by the data collectors, thus the often and sometimes options will be reiterated upon. It is worth mentioning that 76.8% of the responses were females whether married or single. First, regarding availability of domestic and GBV (table 4.3.4.1); to identify participants’ experience of domestic violence, they were asked “have you been physically abused /injured”; 15.4% reported often and 22.3% reported sometimes, while the psychological /emotional abuse slightly higher as indicated in the statement “Have felt guilty or invaluable”; 17.4% reported often and 27% reported sometimes. Also 14.4% of the participants reported often and 45% reported sometimes on the statement “have felt unsafe and afraid”, complementing this feeling, 17.5% of the participants reported often and 21.6% reported sometimes on the statement “expressed desire to leave family to protect self”. Furthermore, the participants were asked “have children ever been hurt as a result of abusive behaviors within the family”; 17.4% reported often and 30% reported sometimes indicating the impact of domestic violence on children where this need to be highlighted in programs and strategies set for combating violence.To have an impression of the participant’s willingness to change behaviors in attempt to reduce violence within their home environment as in the statement “expressed desire to change behavior to make things better toward family members”; 21% reported often and 31% reported sometimes. But when asked about their seeking medical attention for injuries resulted from violence were less when 11% who reported often and 16.5% reported sometimes, and to much less extent their responses on the statement “filed complaint to formal sources to protect yourself (police, lawyers etc…); 7% reported often and 14% reported sometimes. While when asked about “seek help from other family members or neighbors, religious leaders etc…) the responses rated slightly higher; 9% reported often and 17.3% reported sometimes. 1) Questions reflecting selected domestic violence issues; Please indicate your response by marking (×) as follows: often means more than (5 times), sometimes means (2-4 times or less), never means (0 times)
 2) Questions reflecting Sexual violence among spousesThe following 6 items reflected the spouse's perception and practices of domestic violence with emphasis on sexual abuse (table 4.3.4.2). Although the responses were minimal, yet it indicated some kind of sexual abuse among them; for the statement "have been forced to have sex"; 6.7% reported often, 18.3% reported sometimes. Regarding violence and pregnancy, 11.5% reported often, 28.8% reported sometimes on the statement "violence is worse when wife was pregnant" 11.5% reported often, 28.8% reported sometimes, and a similar response was for "violence causes miscarriage for pregnant wife", 10.8% reported often and 31.8% sometimes. The question on sexual problems and violence was indicated in the statement "desert you because of sexual problems"; 12.5% reported often and 20% reported sometimes. Sexual violence as part of punishment among spouses was indicated when 7% reported often and 29.4% reported sometimes on the statement “deprive you from sexual act as a punishment”. The least responses were for the statement "have extra marital relationship" 7.5% reported often and 14.4% sometimes, this could be explained as either it’s the reality or the other spouse do not know much about his partner relationships which is expected. 3) Questions reflecting Sexual violence among spouses
2) Questions reflecting Sexual violence among spousesThe following 6 items reflected the spouse's perception and practices of domestic violence with emphasis on sexual abuse (table 4.3.4.2). Although the responses were minimal, yet it indicated some kind of sexual abuse among them; for the statement "have been forced to have sex"; 6.7% reported often, 18.3% reported sometimes. Regarding violence and pregnancy, 11.5% reported often, 28.8% reported sometimes on the statement "violence is worse when wife was pregnant" 11.5% reported often, 28.8% reported sometimes, and a similar response was for "violence causes miscarriage for pregnant wife", 10.8% reported often and 31.8% sometimes. The question on sexual problems and violence was indicated in the statement "desert you because of sexual problems"; 12.5% reported often and 20% reported sometimes. Sexual violence as part of punishment among spouses was indicated when 7% reported often and 29.4% reported sometimes on the statement “deprive you from sexual act as a punishment”. The least responses were for the statement "have extra marital relationship" 7.5% reported often and 14.4% sometimes, this could be explained as either it’s the reality or the other spouse do not know much about his partner relationships which is expected. 3) Questions reflecting Sexual violence among spouses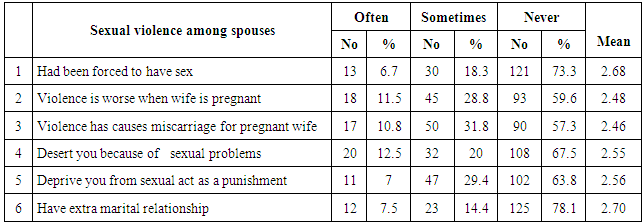 4) Availability and provision of health and social services This part of the questionnaire examined the participant’s knowledge regarding the availability and provision of health and social services (table 4.3.5). Regarding protection facilities; around 50% of the participants reported yes vs. 45% no and 8% not sure on the statement “Protection facilities for abused women are available within your locality”, and 22% reported yes vs. 45.5% no and 32.6% not sure about “protection facilities are sufficient and meet the needs of the abused women”. Furthermore, 36% reported yes vs. 40.3% no and 23.7% not sure on the statement “Protection facilities provide psychological counseling and health information to abused women and youth”. To understand the women attitude toward being abused or violated, participants’ response to the statement “abused women face difficulty admitting abuse” was; 49% reported yes vs. 26% no and 25.5% not sure.
4) Availability and provision of health and social services This part of the questionnaire examined the participant’s knowledge regarding the availability and provision of health and social services (table 4.3.5). Regarding protection facilities; around 50% of the participants reported yes vs. 45% no and 8% not sure on the statement “Protection facilities for abused women are available within your locality”, and 22% reported yes vs. 45.5% no and 32.6% not sure about “protection facilities are sufficient and meet the needs of the abused women”. Furthermore, 36% reported yes vs. 40.3% no and 23.7% not sure on the statement “Protection facilities provide psychological counseling and health information to abused women and youth”. To understand the women attitude toward being abused or violated, participants’ response to the statement “abused women face difficulty admitting abuse” was; 49% reported yes vs. 26% no and 25.5% not sure. 4.3.8. Participants Perception toward Accessibility to Health and Social Information and Services
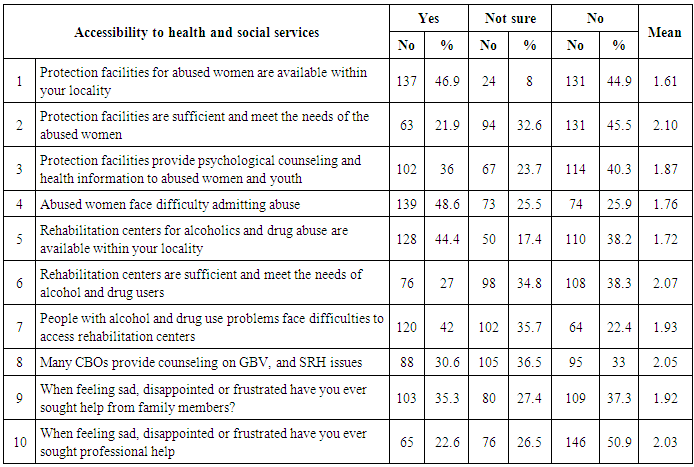 There were also differences on the agreement on statements related to the availability of Rehabilitation centers within their area of residency, 44% reported yes vs. 38% no and 18% not sure, and when asked about rehabilitation centers if sufficient and meet the needs of alcohol and drug users; 27% reported yes vs. 38% no and 34% not sure. Furthermore, they were asked “People with alcohol and drug use problems face difficulties to access rehabilitation centers”, 42% reported yes vs. 22% no and 36% not sure. Only 31% agreed that many civil organizations provide counseling on GBV, and SRH issues.To understand the participants’ attitudes toward seeking help from their families when they are sad, disappointed or frustrated, their responses were scattered 35% reported yes vs. 37% no and 27% not sure, for the same feeling, they were asked “When feeling sad, disappointed or frustrated have you ever sought professional help” 22.6% reported yes vs. 51% no and 26% not sure.
There were also differences on the agreement on statements related to the availability of Rehabilitation centers within their area of residency, 44% reported yes vs. 38% no and 18% not sure, and when asked about rehabilitation centers if sufficient and meet the needs of alcohol and drug users; 27% reported yes vs. 38% no and 34% not sure. Furthermore, they were asked “People with alcohol and drug use problems face difficulties to access rehabilitation centers”, 42% reported yes vs. 22% no and 36% not sure. Only 31% agreed that many civil organizations provide counseling on GBV, and SRH issues.To understand the participants’ attitudes toward seeking help from their families when they are sad, disappointed or frustrated, their responses were scattered 35% reported yes vs. 37% no and 27% not sure, for the same feeling, they were asked “When feeling sad, disappointed or frustrated have you ever sought professional help” 22.6% reported yes vs. 51% no and 26% not sure. 4.4. The Qualitative Data Analysis
- The qualitative data included 5 FG discussions; one with NGOs and CBOs representatives and 4 with target groups including young people and abused women. This variation aimed to collect information as much as possible to draw on the study concepts from different resources and localities.
5. Discussion
5.1. Discussion of the Socio-Demographic Data
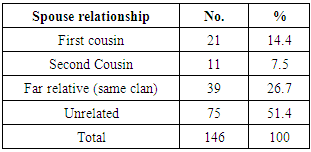
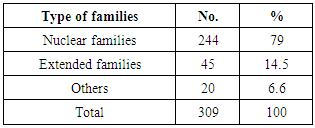
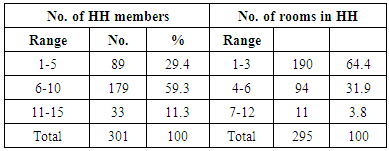
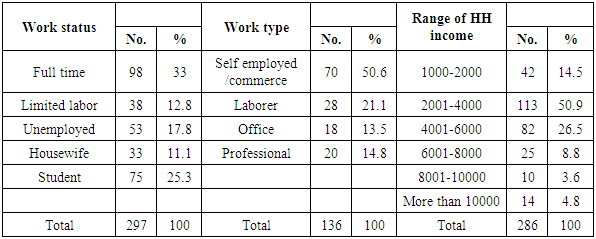
- Out of the 309 participants from the randomly selected households in 4 localities from East Jerusalem where two third of the sample from the old city were; 27% husbands, 20% wives and 45% youth. The overall socio-economic, political and humanitarian situation in the Occupied Palestinian Territory remained challenging and continued to adversely affect the situation of Palestinians in general and Palestinians in Jerusalem in specific. The findings indicated that 79% of participants live within nuclear families, 14.5% live within extended families and 6.6 are either living in compounded or single families compared to 81% for the general population in Jerusalem according to PCBS-JSYB (2010).There is no doubt that age at first marriage is an indicator of fertility rate, and early marriage lead to increase this rate because of longer fertility period for the woman. According to PCBS-JSYB (2010) the average population growth in Jerusalem 1.8% compared to 2.66% for oPt, this was approved in this study when found that the average age of marriage was 23.19 years compared to 18 years in oPt according to the statistics of the year 2007. Yet, early marriage constitutes 18% for ages 17 years and less in this survey and this is very much consistent with 54.6% of the total registered marriages in Shariah Courts and Churches in Jerusalem for ages (15-19) years in 2010 where males represent 5.2% of the total marriages as reported by PCBS-JSYB (2010). Interfamily marriage is another concern, out of 146 spouses interviewed around 49% were married to relatives of whom 14.4% were married first cousin, 7.5% were married second cousin, and 26.7% were married a far relative or from the same clan. Indicating a higher level for the general public when compared to 43%, of whom 26% were married to first cousins, and 17.3% were married to a relative from same clan according to FHS (2006). Furthermore, the FHS reiterated on the reasons for interfamily marriages could be a result of the socio-political constraints and consequently mobility restriction contributes to enforce such phenomenon. Also the low economic conditions where expenses for relative marriages are less, coupled with the societal traditions of interfamily and cousin's marriage are all factors that needs further investigation for this issue. The obtained figures requires the attention of formal governmental and non-governmental organizations and particularly religious institutions to play a part in reducing this phenomena and to lay advocacy campaigns, religious and social awareness programs targeting all groups in the society on the consequences of early and interfamily marriages.Given the special circumstances of Jerusalem and its annexation to Israeli Government and its partition by the segregation wall where all of this documented by confiscation of land and houses in addition to house demolition as indicated earlier leaving east Jerusalem households to live in an over crowded houses and with an average of 3.3 rooms. The study found 64.4% for surveyed households live in (1-3) rooms, 5.4% live in one room and 20% live in two rooms. The average household members were 7 (average 3.53 male and 3.51 female). Another important indicator for poor living conditions was found when 59% of the households are having (6-10) members and 11.3% are having (11-15) members indicating large families living within small houses. Such poor living conditions with over crowded houses can be justified due to Israeli political impact which is characterized by discrimination imposed by Jerusalem municipality on Palestinians where they are only allowed to build on 17% of the land in east Jerusalem and not given permits to expand their houses or to build new ones. 13% of the building permits issued by the municipality between 2005 and 2009 as reported by Al-Quds newspaper (June 6th. 2012). For social issues that need to be highlighted is the polygamy and divorce. Study findings indicated that 5% of spouses were divorced. According to the PCBS (2009), less than 4% of men in the West Bank and Gaza have multiple wives but this study indicated much higher rates when 13% of husbands were having two marriages and 2% were having three marriages. Studies about polygamy and divorce have highlighted that it lowers women’s self-esteem, it is insulting to women, it increases family problems, poverty, and psycho-social problems and that it further reflects negatively on society as a whole. It decreases empowerment and participation of women in public life and is a clear violation to women’s human rights. For economic status, around 46% of participants were working; 33% having full time job and 12% work on sometimes basis, in addition there was 18% not employed. Of those working, 51% were self-employed or work in commerce, followed by 28% professionals and office workers and 14% were laborers. The study indicated that only 8% are currently working in Israel or east Jerusalem which is very much less than 32.6% as reported by ILO (2008). The unemployment rate is very much higher than what the World Bank reported on unemployment rate for the general population; 15.9% in the second quarter of 2009 and dropped to 15.2% in the second quarter of 2010. The average income per household was 4826 NIS per month; around 51% of households income has ranged from (2001-4000) and 14.5% was (1000- 1800) vs. 17% with 6000 and more. Such low figures in terms of employment and income indicate poverty within the households surveyed and very consistent with Al-Quds Newspaper report (May 16th. 2012) on poverty reaching 78% of the total population of Jerusalem are living under the poverty line. In addition, this decrease in income and employment are exacerbated by increases in rents, consumables, and higher transportation costs to access education, work, health services, and even entertainment. For education; 37% of participants are educated at the secondary level, followed by 33.3% at the university level, 23.8% are educated at the primary level followed by 6% are illiterate. The shortage of over 1,000 classrooms leaves approximately 12,000 children out of the education system (IPPC, 2009). Marginalization of education particularly shortage in the number of classrooms and the lack of funding and as a consequence for this shortage made student’s school dropout rate 40% (Al-Quds Newspaper, 2012). Complemented by the report of the ILO mission about the fact that over half of those at the age (15-29) years are neither in education nor in employment and such findings evoke the concerns of each institution and responsible person for the waste of precious human resources because they are neither in education or employment, it’s a “A dangerous mix” as ILO stated.
5.2. Discussion of the Contextual Factors Questions
- Discussion of the participants’ responses on contextual factors will be gathered under 4 themes; home environment, Israeli violence, societal factors and STIs issue that influence GBV.
5.2.1. Domestic Violence within the Home Environment
- Exploring violence within the home environment; the study results indicated that 24% of the participants agreed on being abused within their home environment, much less than 37% PCBS Violence survey (2010) statistics. Of those, 66% reported physical abuse compared to 23.5% of PCBS same report. Only 2% reported sexual abuse, and this could be due to participant’s reservation on answering this private question. For abusers, 68% of the participants claimed that males within the families (46% for fathers and 22% for brothers) and 16.6% claimed that others (mean more than one person, grandfather, uncle and few said the in laws) are the abusers compared to 6% for mothers and 9% for sisters. Their exposure to abuse has varied from months to years where 16% have reported their recent exposure was during collecting the data. Such figures ultimately indicate the availability of GBV intimidated by male partners within the households surveyed and being approved when 51% of abused participants who felt being victims and 27% who felt being survivors. Availability of persons with special needs (handicaps) and domestic violence; 17% of participants agreed to the availability of persons with special needs. Of those, 45% were having mobility problems, followed by 21% for mental health problems and then to less degree for sight and hearing problems. People with special needs within the households were distributed among family members with slight variations among all. To identify the impact of these conditions on domestic violence; around 26% agreed and 21% agreed on sometimes that having persons with special needs within the households have contributed in the domestic violence. The abuse that special needs persons have been exposed to was 50% for verbal/emotional abuse and 50% for physical abuse. Since this concept is out of the scope of the study, it added value to further explore the social and health problems that may contribute to impact the living conditions of targeted people. Within the home environment, domestic violence was examined for the availability of persons watching sex related entertainment programs; around 19% of participants said yes and 12% said sometimes. Of those who watch such programs, 42.5% were the study participants followed by 44% for brothers and sisters, indicating that younger generation are more aware of these entertainment programs either through net or satellite that need to be taken into consideration in any future preventive measures programs. To identify the impact of such behaviors on domestic violence; 26% agreed that such practices within the households have contributed in the domestic violence with 47% for verbal/emotional abuse, 42% for physical abuse and 11.1% sexual abuse which logically speaking can be a contributing factor in sexual abuse. It is noteworthy that sexual abuse is mentioned within this area.
5.2.2. Israeli Violence and Its Impact on Domestic Violence
- The findings indicated that 32% of the participants’ houses were subjected to Israeli violence less than 47.8% for West Bank population according to violence survey (2011). Within the exposure to these houses; 60% of the study participants and 32% of the males within the families were abused. Such figures emphasize the different forms of GBV imposed on the Palestinians; in this case, the man is the one being abused more than women indicating GBV not only male and female issue rather than power issue. To identify the impact of these conditions on domestic violence 23.2% agreed that exposure to the houses by Israeli forces have contributed to increase the domestic violence. Israeli violence within the work sphere; 30% of participants have worked and/or still working in West Jerusalem/Israel and 10% work on sometimes basis. Of those, 38% were exposed to abuse during working hours; 78% were exposed to verbal/emotional abuse and 22.4% were exposed to physical abuse. Such results indicate Israeli violation behaviors on the dignity and human respect for the Palestinian individual, beside all other violations mentioned earlier that need to be focused upon by national and international communities for the application of human rights conventions to support Jerusalemites suffering all kinds of human rights violations.
5.2.3. Social and Behavioral Patterns and Its Impact on Domestic Violence
- Policy of racial discrimination and exploitation of the Israeli occupation authority over the weak Palestinians left Jerusalem people face serious social and behavioral problems manifested in increased number of people who smoke, use illegal drugs and smoking in addition to poverty and widespread unemployment among them where these behaviors are anticipated to play a part in the domestic violence. Investigating the prevalence of smoking behaviors among target groups found that 45% of participants admitted to smoking, double the findings for the national statistics 22.5% as indicated in PCBS–FHS (2010). Of those smokers, 2.3% started smoking at less than 12 years of age, and 73% smoked during adolescent period (13 and 20 years). Furthermore, 80% of family members were smoking, of those 84% for males and 16% for females, where only 0.8% of women are smokers as indicated in the PCBS–FHS (2010). Yet, smoking was found to be the least to provoke violence among family members when only 15% agreed to that. Examining the kinds of smoking, the majority were cigarette smokers while Argelah smokers are on the rise comparing 18% of participants vs. 6% for their family members noting that 46% of the study participants are young people. Worse of all is the availability of Hashish smokers when 4.5% of the participants and 5% of their family members indicated their use of Hashish (for details please refer to 4.26 table in Ch.4). When participants were asked for the reasons that make people smoke, they indicated the most common reasons are; unemployment and bad economic conditions, psychological pressure, like to try new things and the peer pressure. Such socio-behavioral attitudes need a lot of attention by social and health institutions to work on this problem extensively and consistently with the minimal cost such as awareness including families especially the majority smoked during their childhood and adolescence.Investigating the prevalence of Alcohol drinking behaviors, 16.4% of study participants and 23% of the participants’ family members drink alcohol. Surprisingly and knowing the cultural, religious and traditional practices among Palestinians regarding these matters, it was found that both genders consume drinks in a varying degrees (35% for fathers, 25.6% brothers, 14% mothers and 14% daughters). Drug abuse is one of the most visible social problems and a center of attention by many communities and societies. This study found that 12.2% of study participants know about drug abuse among the households’ members; of those, 23% were the participants themselves, followed by 43% males within the household (fathers and brothers) and 7% for mothers and sisters where their use has varied from months to years. This is very much congruent with release of center of Arab youth survey in Jalil (26th. Of June 2012) that indicate 12% of Arab youth aged of 12-18 years are drug users. There was 13% of the drug users imprisoned as a result of using illegal drugs. Yet, there was a scarce positive indicator for actions to be taken whether at the legal or preventive measures when only 13% have been imprisoned and 8.1% have been referred to treatment and rehabilitation. Of those 40% were willing to be referred and 60% were not. But most of the participants reiterated that civil society institutions are taking care of this social problem, minding these institutions lack the resources for sustainability and continuity as been reiterated upon in the FG discussion. Although 72% agreed that drug use and 56% that alcohol drinking play a part on domestic violence, the participants justified the reasons for its use to be family problems, lack of religious commitment, lack of moral commitment, unemployment and economical situation, psychological pressure, imitate others, try to have leisure and entertainment activities, try new things and bad companions. These indicators are serious and considered an alarming signs for governments and institutions to work collaboratively on preventing these unfavorable social behaviors through awareness raising programs, and finding alternatives for their wasted time through structured entertainment and beneficial activities such as sport clubs, educational activities, volunteerism and civil society engagement. Also, there is a need for treating and rehabilitating people already in addiction for smokers, alcohol consumers and drug abusers.
5.2.4. Discussion of Questions Related to STIs and HIV/AIDS
- The participants were asked about their knowledge regarding the availability and types of STIs; Only 4.4% of the participants and 5.6% knew about other family members to suffer from STIs; they complained mainly from Candida, to less degree from syphilis and then the least was for hepatitis B and no one reported on HIV/AIDS. The mostly affected were the mothers 50%, father 33% and sisters 18%. Only 15% of the participants agreed and 33% agreed for other family members if having STIs play a part in the domestic violence. Around 65% the participants were able to recognize STIs transmission modes, and the common statements were; illegal sexual relationships, having sex with multiple partners and blood transfusion. Very few mentioned that transmission can be through food, drinking or touching the patients.To understand if there is undesirable behavior like extramarital sexual experience by any of family members that may lead to STIs; around 12% agreed that they know and 20% were not sure. But when asked who that family member was, the majority was for the males to practice such relations. When participants were asked if this situation played a part in the domestic violence they experience or know of; 32.5% agreed to yes, and 34.4% were not sure.Having 4.4% of the participants and 5.6% of their family members with STIs is not easy and considered an alarming sign to tackle this problem. Also the number of people could be questionable since many local studies believe that talking about such diseases is a stigma and can be a sign of undesirable behaviors in the Palestinian conservative society and thus many cases were denied. Therefore what ever the size of the problem found it is very necessary for those in power to tackle this problem by further assessment to find the appropriate intervention measures including preventive and curative.
5.3. Discussion of KAP toward SRH and Gender Relation Issues
5.3.1. Selected SRH Issues and Gender Relation
- Participants agreed with a balanced attitude among both genders for FP methods as approved by spouses’ discussion and support of the husbands. On the contrary, the participant’s knowledge indicated high level of “do not know” responses on the condom use as best FP method and the best mean for protection of STIs. Participants’ knowledge about availability of unsafe abortion, accessibility to and availability of FP services was relatively limited. This “do not know” response among participants requires the attention of health providers to launch awareness programs regarding the importance of condom use and to promote men's attitude toward its utilization. These programs should target couples and young unmarried people as well who constitute half of the society and are the near future husbands and wives. In general, it was noted that husbands were supportive to their wives during their pregnancy and delivery; the majority agreed that number of pregnancy and number of children in the family is decided by husbands and wives, men accompany their wives for delivery, and around 50% accompany them to maternal health care. More than half of respondents agreed on men willingness to go to health center if they complain of reproductive/urinary tract problems and the same for the issue of STIs where people refuse to talk about because it is considered a taboo and shame complemented by 68% agreement among participants regarding women preferences to women physicians for STIs treatment and maternal care. Concluding the findings on SRH and gender relation matters, worth the attention on male involvement in SRH matters (males do not know about females and visa versa) with consistent awareness and service programs for both sexes and for all generation on same reproductive health issue so each will know about the other needs rather than dealt with separately.
5.3.2. Selected Family Dynamics and Its Impact on Gender Relations
- Majority of participants agreed on the availability of early marriage and interfamily marriage within their communities, and so on early marriage is more happening among relatives indicating huge unhealthy familial and societal practices toward these matters. To examine the political impact on early marriage the responses were scattered on the statement “early marriage prevalence among girls is more noticed since the wall erupted and mobility restriction increased”. The participants expressed positive attitudes toward marriage issues when 75% disagreed on statement “I’m in favor of early marriage”, and 71% disagreed on the statement “I’m in favor of interfamily marriage”. Such responses reflect positive attitudes of participants but negative societal practices that require intervention programs in terms of awareness and law enforcement. Also requires law and policy makers, religious and institutional leaders to work collaboratively toward reducing the incidences of early and interfamily marriages. Regarding family dynamics and gender relations was found that two third of participants agreed that decisions regarding family matters are shared within family members and decisions regarding the marriage of the girls are shared with them. About half of the participants agreed "decisions regarding marrying the girls or boys are the father’s responsibility". Such figures indicate gender power dominance by fathers to take decisions on behalf of their sons and daughters regarding their future marriage and thus their future lives, where this issue should be discussed among societal and religious figures and awareness programs. Regarding the impact political and financial situation on violence was expressed when more than two third agreed that it increase rage and violent behaviors among family members. This agreement was much higher for the impact of unemployed husbands and working wives to increase frustration and abusive behaviors among family members. On the contrary, there was a variation in responses on the statement “the man (father/older brother) is the source of violence in the family” and on the statement “domestic violence is more prevalent among extended families”.
5.3.3. Selected Family Factors and Drug Abuse
- Regarding family dynamics and the use of illegal drugs; majority agreed that drug abuse is more prevalent among disrupted families, separated or divorced parents where it pushes some children and youth to use illegal drugs, physical environment of work and housing has a large influence on people to use illegal drugs. More than half agreed that drug abuse is more available among child labor. On the contrary, 43% agreed that drug abuse is more prevalent among large families and36 % among poor families while 71.4% agreed that the level of parent’s education has an effect on children to use illegal drugs. More than half of the participants’ agreed that alcohol drinking and drug abuse are correlated and one third agreed that smoking and drug abuse are correlated. Although participants are very well aware of the circumstance that influences young people to use drugs, yet alcohol drinking and drug use on the rise that need to urgent attention by policy makers, health and social institutions and CBOs to intervene at all levels to prevent further spread, and rehabilitate affected people.
5.3.4. Participants KAP of Domestic Violence
- Although the ratio of responses were minimal regarding domestic violence, yet it indicated its prevalence among wives; 14.5% reported often and 29.6% reported sometimes on being physically abused and similar responses of being psychologically /emotionally abused. The PCBS domestic violence survey (2006) indicated that 23% of surveyed women had experienced physical violence and 61.7% had experienced psychological violence. Perception and practices of domestic violence is a family matter and many participants were reserved to respond to these questions and preferred the never option as been noted by the data collectors. The low rate at which women and girls report such matters is a symptom of the significant social and legal obstacles to the way of meaningful gender-based violence prevention and response in the Palestinian territories. Although the ratio of domestic violence responses was the least among other responses, yet, in this section complements the participants responses in the previous section (refer to 4.21. in results chapter) when 24% admitted their exposure to physical violence. Combining the often and sometimes responses; around 28% of the participants reported physical abuse and injury, 44.4% emotional abuse, and 45% reported abuse on their children where this need to be highlighted in programs and strategies set for combating violence. Around 27% of abused participant’s agreed often and sometimes to seek behaviors toward medical care, 21% filed complaint to formal sources to protect self (police, lawyers etc) and 26% were seeking help from other family members or neighbors and religious leaders. According to Al-Muntada domestic violence report (2008), a woman [victim of violence] thinks a hundred times before going to court, she thinks it will only result in scandalizing herself. The same report indicated that legislation dealing with the protection of women is stalled due to the immediate, more “important” concerns of the Palestinian National Authority whose priorities do not include social issues and domestic violence which is of marginal concern. Given the fact that traditional Palestinian cultural values have viewed violence as a ‘private and family’ affair, and women usually do not want to leave the children behind, thus they feel no other option left other than to remain in a violent marriage (Al-Muntada, 2007). For a better solution of the problem, 56% of the participants expressed the desire to change behavior to make things better (toward spouse, children and others) which indicates positive attitudes of both genders to resort to more positive behaviors that can make their lives better.
5.3.5. Sexual Violence among Spouses
- Six statements were specified to husbands and wives to assess their perception and practices on sexual abuse, the responses were very minimal and few, participants were reserved to respond to the question as many commented "this is a private matter", others said “we do not like people to know about these matters". Yet, the results indicated some kind of sexual abuse inflicted mostly on wives; for the statement "have been forced to have sex"; 6.7% reported often and 18.3% reported sometimes, and "deprive you from sexual act as a punishment" 7% reported often and 29% reported sometimes. Yet, the given figures are less than PCBS violence survey (2010) which indicated that 11.5% had experienced sexual violence at the hands of their husbands. Connecting violence and pregnancy, 11% of spouses reported often, 18.3% reported sometimes for the statement "violence was worse when wife was pregnant", and 10.8% reported often and 32% reported sometimes for the statement "violence has caused miscarriage for pregnant wife".The question on sexual problems and violence was indicated in the statement "desert you because of sexual problems"; 12.5% reported often and 20% reported sometimes. Sexual violence as part of punishment among spouses was indicated when 7% reported often and 29.4% reported sometimes on the statement “deprive you from sexual act as a punishment”. The least responses were for the statement "have extra marital relationship" 7.5% reported often and 14.4% sometimes, this could be explained as either it’s the reality or the other spouse do not know much about his partner relationships which is expected. Although the spouses were reserved to give such confidential information about this private matter, yet the given data indicates the availability of sexual abuse particularly among spouses but does not indicate the size of this problem.
5.3.6. Availability and Provision of Health and Social Services
- Regarding availability of protection facilities for abused women within their locality of residence; around 50% of the participants agreed, 22% reported that they are sufficient and meet the needs of these people and 36% agreed that these facilities provide psychological counseling and health information to abused women and youth. To understand participants’ attitudes to the statement “abused women face difficulty admitting abuse” was; 49% reported yes vs. 26% no and 25.5% not sure. Yet, there was a scarce positive indicator where only 8.1% of the drug users have been referred to treatment and rehabilitation, where most of the participants reiterated on the civil society institutions for taking care of drugs users. Regarding rehabilitation centers for people with alcohol and drug users within their locality of residence; 44% of the participants agreed and 27% reported that they are sufficient and meet the needs of these people. To understand the accessibility to these facilities, 42% agreed that people with alcohol and drug abuse problems face difficulties to access rehabilitation centers. Regarding seeking help and psychological support; 35% reported yes to seek help from their families and 22.6% reported yes to seek help from professionals leaving large number without any help and here what needed to be reiterated upon by all concerned people.
5.4. Discussion of the Qualitative Analysis
5.4.1. FG Discussions with NGOs and CBOs Representatives
- This FG was with 12 representatives from NGOs and civil society organizations in east Jerusalem working in the areas and overlapping with youth and women empowerment, human rights, psychosocial counseling and SRH issues and youth. This FG was conducted prior to any step taken for the study; it was the basis for clarifying the concepts under study and laying the ground for structuring the quantitative questionnaire. These institutions are working on many levels and for different target groups, some emphasized women empowerment strategies socially and economically, gender equality and human rights through awareness and education programs such as Youth Women Christian Association and Youth Women Muslim Association. Others are working on youth empowerment programs through launching extra curricular activities, sports, and awareness programs regarding alcohol drinking and drug abuse such as Al-Sarraya while Rua’aya association in addition works on empowerment and job opportunities for young adults. Some are working on management and rehabilitative services for abused women and children and offer individual and group counseling and follow up for abused people like Makassed hospital and Al-Quds Society for Women Counseling while Sheikh Jarrah Women Forum work on women empowerment in addition to preventive and protective services for abused women. No one of these institutions offers SRH and STIs services, but some mentioned their collaboration with other health institutions regarding these matters for awareness and referral if appropriate. There was a consensus among all representatives about youth involvement in social and behavioral problems where they emphasized the spread of drug abuse, alcohol drinking and violence. Some said “young people became an integral part of these problems- and a product of the social and political problems”. Others indicated the availability GBV manifested in all forms and reiterated upon as said “these social and behavioral problems are available abundantly but hidden under the rug as pretext for the honor and family dignity particularly for issues of GBV, sexual violence, incest and unsafe sexual practices”. On the contrary, others said “NO, these problems are surfacing and people talk about them but we do not know their extent and severity” while many commented on the spread of these problems and the lack of measures taken to contain them. The representatives were competitive in describing the availability of GBV and it’s widespread among family members, in the streets, work environment in addition to violence imposed by Israelis. They were able to categorize its types as physical, psychological, economic, social and sexual violence and were aware of its impact on the well being of the abused individuals particularly women and children.There was a variation in responses regarding women choices and practices in case they were exposed to violence as some said; "there is intervention at family level, intervention by local committees for community reform and intervention at institutions level to solve problems arising from violence, “a temporary intervention that does no resolve the whole issue” as said by one of them. Others reiterated on the importance of women empowerment through increased self-confidence and financial independence which should be worked on by all particularly local and international NGOs and institutions. Few representatives reported their collaboration and coordination with other institutions such as the universities, Makassed hospital and Palestinian Family Planning and Protection Association regarding SRH issues while others have some collaborative programs on gender issues. It was noted that gender relations is a cross cutting issue among most of these institutions.Challenges that encounter these institutions activities • Limited resources and lack of sustainable programs and funding • Very minimal community responsiveness toward these activities • Lack of commitment by targeted women or youth toward the activities they are invited to• Lack of clear laws and policies as real intervention strategies toward the available social and behavioral problems • The proposed intervention programs in East Jerusalem are scarce and not focused “whatever available we take it” as said, they are not sustainable neither effective because they lack the comprehensive and collaborative approaches in dealing with such matters • Few networking and collaborative approaches among each other and among other UN agencies or national institutions. Recommendations by representatives • Increase the level of coordination and collaboration among Jerusalem institutions working in the areas of GBV, social and behavioral problems to complement each other activities aiming at introducing comprehensive intervention strategies regarding these issues • Networking with other institutions at national and UN agencies to have financial and expertise support regarding these matters • Each institution should have a division for women • Engage young people with beneficial activities such as extra curricular activities and voluntary work to increase their community participation, with more programs on empowerment and awareness regarding these matters • Involvement of schools targeting the teachers and students to involve largest number of young people in awareness and empowerment programs • The Palestinian authority should be more involved in Jerusalem matters, intervention programs are not political and can be implemented the way it is in Ramallah as many said.
5.4.2. Focus Group Discussion Young People
- The FG discussion with young people entailed; 14 young girls from private school (aged 15-18 years), 14 young people from a youth club in the old city (8 males and 6 females aged 17-26) and 9 young people from a neighborhood in Siwaneh, a suburb of the old city. The data will be presented collectively or otherwise as indicated by each. FG discussion with women subjected to violence will be narrated aside. Questions related to GBV; the young people agreed on availability of GBV and it’s widespread among family members, in the streets, work environment in addition to violence imposed by Israelis. Many girls commented on verbal sexual harassment they face in streets “silly words and comments”.There was variation on the reasons of violence, but the most common answers were; family problems, poverty, ignorance and occupation, while some of them pointed to male dominance within the Arab society allowing for more spread of GBV. Most of them referred that males are the source of violence while others referred to women especially if she was a stepmother, an aunt and a teacher etc... In other words when women are in power position they can inflict violence. They were able to categorize the types of violence and could define them. They defined physical violence as hitting and kicking, while defined psychological/emotional could be verbal abuse, lack of essential needs like clothing and schooling. They commented on sexual violence, though it is available but it’s not reported, they further defined sexual violence as a kind of rape and assault. The majority were able to describe the impact of violence and the common themes were; that it leads the abused individual to have low self-esteem, depression, and isolation from others at home, school or university, and to feel lonely and fearful, run away from any problems he/she faces and ultimately will lead to psychological and physical and social problems. When asked about the exiting services; some of them agreed on its availability while the others did not know. The services they know about are awareness, rehabilitation and few mentioned the helpline. The young people only know that civil society institutions offer services regarding GBV and few said about religious people interventions among families. But majority claimed these services do not meet the needs.Perception of participants of the social and behavioral problems among people; they heard and knows about other young people, men and women using illegal drugs, some said “those who take illegal drugs usually do not admit that”. They heard of STIs but do not know much about people having these illnesses, but also commented that it’s a result of low morality and unsafe sexual conduct, drug users of injections and contaminated blood transfusions. Regarding alcohol drinking, they mostly referred to those working in West Jerusalem, or going there to entertain themselves. The majority pointed out that these three problems (drug abuse, alcohol and STIs) are interrelated and those who experience them have some kind of relation on the Israeli side either working or going there for entertainment, some said “we know about these people but we avoid them”, other said “they are shame for us” and many said “the occupation promote the use of illegal drugs”. There was variation on the reasons for social and behavioral problems, but the most common answers were; peer pressure, and imitation of others, entertainment, family problems, psychological problems, unemployment and working in Israel. The young participants’ knowledge was assessed for consequences of these social and behavioral problems by asking them to mention 3 problems for each; for drug abuse they mentioned; addiction, Schizophrenia, economic problems due to loss of money for buying drugs where he/she will resort to theft, which could lead to prison. For alcohol use they mentioned physical problems and liver cirrhosis, psychological problems and loneliness. For unsafe sex practices they mentioned; STIs, low self esteem and lack of trust in others, stigma and shame. They reiterated on this part as said “STIs and HIV in particular mostly are results from lack of commitment to societal and religious morality where our culture revolve about it”. The participants emphasized the consequences of these social and behavioral malpractices are reflected not only on them but also on their families financially and socially exposing them to being embarrassed and stigmatized. The young people recommendations • Awareness and dissemination of knowledge about the dangers of these social and behavioral problems among young people and their families • Full cooperation among children families and school administration to discipline and control children behavior • For prevention of STIs as said “the best way to avoid these illnesses particularly AIDS is Taqwa Allah and to stay away from illegal sexual relationships” • Encourage people who are subjected to these problems to seek help for treatment and for rehabilitation • Invite some prominent professionals in the area of SRH and gender issues to conduct sessions among young people and in civil societies• Launch awareness programs for young people on SRH matters and gender equality so young people can understand these concepts as soon as possible.
5.4.3. Focus Group Discussion with a Group of Abused Women
- There was a discussion among the study investigator and 7 women of whom 3 were severly abused. Two ladies expressed their problems and talked about the violence they are experiencing easily and without reservation. The 3 ladies have been living in this condition for many years; they are in mid forties to mid fifties and were abused physically and sexually. Two were abused sexually by their fathers when they were young girls. The reserved one expressed anger, rage and cried most of the time, because it was her first experience to talk about her long and complicated experience and to express her feelings explicitly to outsiders. Sheikh Jarrah Women forum with its capacities in terms of empowering women have always gathered these women where they found it very helpful for abused women to share experiences and to support each other. There was some professional help in terms of support, individual and group counseling, awareness sessions and some entertainment activities that help these ladies to feel good. A success story was found that one of abused ladies have a strong personality and voluntarily wherever she knows about other abused women she willingly help them and bring them to this center so they can be part of support and help. Such independent civil organization can make a difference in the lives of these abused women and with minimal costs, is an experience that should be supported by all means possible and repeated by other organizations.